Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Effects of Epinephrine on Frog Ventricle
By
RICHARD A. HENXACY, P H . D .
pressure drop between the heart container and
beaker was used to measure the flow rate.
The extracardiac pressures (within heart container) and the lateral isotonic pressures were recorded by means of 2 Statham gages (F and G)
and a Hathaway recorder with a paper speed of
either 4 or 10 inches per second (fig. 1). In some
experiments, valves (J and K) were introduced in
both the inflow and outflow channel, which permitted an additional resistance (hypodermic needle) to be inserted on the outflow side. Isoehoric
(isovolumetric)2 pressures were often recorded.
When the extracardiac pressure (P n ) dropped
below the base line (fig. 2), the heart was actively
expelling its contents back into the reservoir.
Pressures above the base line indicated filling.
Since the filling pressure is constant, the rate of
change of the transmural pressure is indicative of
the relaxation rate, and is calculated from the
pressure-time curve from manometer F (fig. 1).
Whereas this is usually approximated as the difference between the pressure recorded by an intraventricular manometer and either atmospheric or
intrapleural pressure, such an approach did not
seem feasible in these experiments. Since the extracardiac pressure in this preparation is constantly
changing and it was not possible to use an intracardiae transducer, transmural ventricular pressures, and flow rates were calculated from the
information obtained from the manometers and
the resistance of the inflow cannula and "U" tube.
FR = Po/Wo whore Fli is the flow rate, Po is
the pressure outside the heart as related to the
surface of the fluid in the beaker, and Wo is the
resistance of the "U" tube and attached resistor.
W
T
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
HE possible methods by which epinephrine may increase cardiac output, though
in practice they are not completely independent, can be separated for purposes of discussion as follows: (1) increase in end-diastolic
volume; (2) decrease in end-systolic volume;
and (3) increase in heart rate.
The first 2 factors determine the stroke
volume. Assuming a constant heart rate, the
end-diastolic volume can be increased by only
one of the following factors: (1) an increase
in diastolic time by shortening systole; (2)
decrease in the average resistance to filling
(renitenee) either by decreasing the average
resistance of the myocardium during diastole
(an increase in distensibility) or by hastening
relaxation after contraction, or both; and (3)
by increasing the filling pressure.
A decrease in the end-systolic volume (assuming constant end-diastolic volume) can be
accomplished by an increase in the strength
of contraction, an increase in its duration,
a decrease in the opposing (aortic) pressure,
or by atry combination of these.
It is well known that epinephrine increases
the strength of contraction and the heart rate.
However, little conclusive evidence has been
presented about the effects of epinephrine on
relaxation and resistance to filling. The present series of experiments were performed in
order to determine these effects.
Pc = Po X — --- , Pc = pressure drop through
''' o
the heart cannula, Wc = the resistance of the inflow cannula. Pv = 1\ - Pc - Ph - Po (Wc/W0)
where Pv is the true intraventricular pressure and
Ph is the head of pressure in the reservoir. The
transmural pressure (Pt) at any instant is Pv - Po
= Ph - Po (1 + WC/WJ. The rate of change
d P,/dt — K APJAi since Ph is a constant, and
Methods
The methods wore similar to those used in the
preceding- experiment;1 however, some changes
were lmidc. Instead of a recording pipette, a "U"
tube with a 16 gage needle attached was used to
connect the heart chamber to a beaker, and the
K =
From the Department of Physiology, Ohio State
University, Columbus, Ohio.
Supported by a grant from the National Institutes
of Health, U. S. Public Health Service.
Research performed during Dr. Hennaey's tenure
of a Post-Doctoral Fellowship of the Central Ohio
Heart Association.
Received for publication March 28, 19G0.
Circulation Research, Volume VIII, .Inly lltoo
-1-WC/WO.
As the pressure outside the ventricle increases,
the drop in pressure across the ventricle decreases.
At the time of the greatest extra cardiac pressure
the diastolic flow rate is maximum. This is the
point of minimum renitenee (R,,,) and it is calculated as previously reported.1
The volume difference between the end of systole
and the end of diastole was determined by use of a
831
HENNACY
832
.2
,B
i)
1
c
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
I
-A
4
fi
B
1.0 1.2 1.4 1.6 1.8 2.0 2.2 2.4 2.6 2fl 3.0
—-5TS—1 G
^
.
1
1 p
•
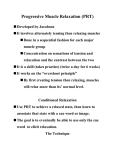
Figure 2
N
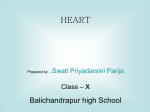
Figure 1
Apparatus used icith the isobaric and isochoric
heart preparation. In certain experiments, a valve
J and a return flow tube I with valve K icere used.
Otherwise, the heart pumped fluid bach into the
reservoir except during isochoric contractions. A =
Heart cannula. B and C = Three-way stopcocks.
D = U tube. E = Resistor. F — Statham gage (venous) measures extracardiac pressure. G — Statham gage (venous) measures intracardiac pressure.
H — Outflow resistor. I = Outflow tube. J = Inflow valve. K — Outflow valve. L = Tube from
oxygen tank. ]\[ — Reservoir. N = Heart container.
planiineter, since during diastole the area of the
P0-timo curve is proportional to the total flow.
Another measurement of relaxation is the time required from the beginning of filling until the
plateau is reached (fig. 2 A-B, relaxation time)
at which time the resistance is at a minimum and
inflow rate becomes constant.
Results
Without Valves or Added Kesistors
Effect of Pressure Changes on the Relaxation Rate
Normal ventricle. Within a range of small
filling pressures (1 to 2 cm.) the rate of relaxation is constant, and therefore independent of the pressure. However, with higher
filling pressures gradually applied, the rate
of relaxation becomes proportional to the
pressure. Previous experiments have established that sudden pressure increases lead to
increases in the minimum renitence.1 How-
Comparison of isobaric to isochoric (isorolumetric)
transmural pressures. Ordinate, pressure in grams/
t:m..1; abscissa, time in seconds. Solid line, normal;
dashed line, after 0.2 [x.g. of
epinephrine/ml.
Upper. Isobaric contractions. Transmural pressures
above 0 line are positive, obtained during filling;
pressures below the 0 line are negative, obtained
during systole. A-B = Diastolic relaxation time.
Lower. Isochoric contractions. Transmural pressures are measured relative to the filling pressure
at the commencement of contraction.
ever, the first effect of a pressure increase is
an acceleration in the rate of relaxation, followed by a decrease if high (> 8 cm. H^O)
pressures are used. If the pressure is then
reduced, the rate of relaxation continues to
be slower than that previously observed for
the lower pressure, but the relaxation rate
returns to normal over a period of 5 to 10
minutes.
I-Iypodynarnic ventricle. In a ventricle with
a small stroke volume, the relaxation rate is
small, and initially proportional to the filling
pressure. "With higher pressures, the relaxation rate increases, but still remains relatively
small if the ventricle does not respond to increased filling pressure by an increased ejection (hypodynamic heart). This may be
related to the low pll and hypoxia which
accompany small stroke volumes in this
preparation.
Effect of Frequency on the Rate of Relaxation
If the filling pressure is low or medium (1
to 8 Gm.), the rate of relaxation is slowed by
both fast and slow contraction rates, and has
Circulation Research, Volume Vlll, July 1900
833
EPINEPHRINE IN DIASTOLE
a particular rate at which the most rapid
relaxation occurs. Thus, with about 5 cm. of
filling pressure, the maximum relaxation rate
is observed at about 15 to 20 contractions a
minute. In contrast to low pressures, in 1 experiment in which the filling pressure was
.15 cm., the slowest relaxation rate occurred
when the contraction rate was 30 beats/min.
Higher or lower rates of contraction resulted
in a great increase in the relaxation rate.
Effects of Epinephrine on the Relaxation Sate and
Diastolic Relaxation Time
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
Low pressures (1 to 2 cm.) and a contraction rate of 12 beats/min. At low pressures,
the normal relaxation is sometimes greatly
slowed, even without epinephrine. In hearts
with a fairly rapid relaxation at low pressures, epinephrine greatly lengthens the diastolic relaxation time and greatly reduces the
maximum relaxation rate (fig. 3). However,
if sufficient time is given for complete filling
by adjusting the contraction rate, the volume
intake during diastole will usually be slightly
increased, in spite of the slowing of relaxation. This indicates probably a decrease in
the end systolic volume as a result of the
inotropic effect of epinephrine.
At 5 cm. filling head, contraction rate 12
to 30 beats/min. In 9 out of 13 cases, the
maximum rate of relaxation was slower with
epinephrine. In 2 instances, the maximum rate
remained the same. In only 2 experiments did
the rate increase. In one of these experiments,
the stroke volume was small. In the other,
the beginning of the relaxation was considerably slower. In all but 2 cases, the relaxation time (time from the beginning of filling
to the plateau) increased.
At pressures from 8 to 15 cm. and contraction rate from 12 to 30 beats/min. With
the filling pressure at 8 cm., 3 out of 4 experiments showed an increase in the maximum
rate of relaxation, while 1 experiment showed
no change. "With new preparations, 2 out of
4 at 10 to 15 cm. of filling pressure showed
no change, while the other 2 showed a
decrease in maximum rate of relaxation.
However, in all experiments the diastolic reCirculation Research. Volume VIII, July 1060
r*
^
—
•
T.-.-C
1
2
3
4
!
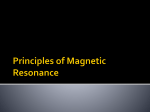
Figure 3
Effect of epinephrine and pressure changes after
epinephrine on the relaxation rate. Solid line, normal (5 cm. JJ^O pressure); dashed line, 0.2 jxg.
epinephrine/ml. added; dotted line, pressure raised
to 9 cm. JJ^O. Ordinate, renitenee in Gm. sec. cmr"
laxation time was increased after using epinephrine. At continuous filling pressures of
10 cm. or greater, the heart appeared distended and gradually contracted less effectively, which was irreversible upon reducing
the pressure. It is presumed that these hearts
were damaged by the high pressure.
Effects of 'Epinephrine on the Minimum Renitenee
In table 1 are the values of the minimum
renitenee (P/Flow) of the heart at 20 to 22
C, before and after the addition of 0.2 ^g
of epinephrine per ml. ("Winthrop Laboratories). The last 2 columns in the table show that
there is no consistent change in this value due
to epinephrine, though the dosage consistently
increased S3-stolic pressure. In hearts that are
hypodynamic either naturally or from the effects of sodium pentobarbital, epinephrine
does lower the Em toward the normal value.1
Effect of Valves and Added Outflow Resistance on
the Relaxation Rate
With the insertion of valves, it is possible
to have a low filling pressure, and yet insert
resistance into the outflow channel. The addition of a resistor (no. 18 needle attached to
reservoir return tube) to the system only
slightly affected the rate of relaxation of the
normal heart. In some cases, the relaxation
rate continuously decreased, because of probably a reduction of stroke volume and the
effects of hypoxia. With epinephrine and
valves but no resistor the rate of relaxation
was greatly slowed, as in the case of those
834
HENNACY
Table 1
Effect of Epinephrine on Rm and the Maximum Rate of Relaxation'"'
Experiment
no.
Heart rate
Cont./min.
1
2
20
4
5
12
12
20
12
6
24
7
8
IS
3
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
9
10
:n
12
13
12
12
12
12
20
20
Stroke volume
After
Norm.
.2/iEp.
.71
.40
.81
.74
.27
.24
.90
.75
.41
.77
.71
1.00
.69
.26
.28
.75
.41
.82
Maximum relaxation rate
K - j — Cm./sec.
After
.2 ii Ep.
Norm.
10.7
28.5
20.S
29.6
13.3
10.7
14.5
9.1
13.8
16.0
8.0
5.9
20.S
44.9
12.8
20.S
20.S
2.6
6.2
2.1.6
64.0
14.0
.SI
.SO
7.6
.85
.92
.50
1.00
3.1.2
27.0
22.0
.60
.50
Relaxation time (sec.) Min.— (dm. sec.cm.-°)
Flow
After
.2 n Ep.
Norm.
.6
.3
.4
1.0
.4
0
3.1
0
3.1
.5
.1
1.1
.4
4.6
2.2
2.7
12.0
3.S
1.6
2.9
9.9
3.3
8.3
5.9
Norm.
1.4
.5
.2
.5
.45
.13
.3
.25
1.00
.7
.7
.1
.25
.30
.4
3.3
3.1
9.4
1.00
2.0
l.S
2.0
.60
6.0
After
.2
IL
Ep.
l.S
1.6
1.0
6.0
"Filling pressure 5 em.; no valves.
experiments without valves. "With the addition of the resistor, however, the rate of relaxation usually approached the normal rate
(before administering epinephrine and inserting resistance), and in some cases was more
rapid.
Effect of Epinephrine on Isochoric and lsobaric
Contractions
Epinephrine increases the maximum rate
of relaxation in isochoric contractions. However, contraction time (period of positive tension greater than the filling head) appears to
remain constant, although Segall and Anrep
reported a lengthening of contraction time
with epinephrine.8
In comparing isobaric to isochoric contractions, it can be seen (fig. 2) that the maximum
rate of volume change (isobaric) occurs before the maximum tension (isochoric), and
after administering epinephrine, this difference becomes even more pronounced so that
the isobaric volume change is completed considerably earlier than the corresponding contraction time of the isochoric heart.
Discussion
Several investigators4"0 have stated that
epinephrine has a direct effect on cardiac
muscle during diastole. Luudin7 and F. Moore
(personal communication) have shown that
the resistive properties to stretch, and thus,
stiffness and viscosity, are not changed in
frog ventricular tissue by the addition of
adrenaline or epinephrine, respectively. The
present experiments on the intact frog ventricle substantiate these conclusions.
In comparing the maximum rate of relaxation of the isochoric contraction in the normal and epinephrine-treated heart, it is obvious that the rate of relaxation is increased
to a greater extent than the pressure is increased after epinephrine. Therefore, it seems
probable that, epinephrine increases the relaxation rate independently of its inotropic
effect in increasing pressure.
Epinephrine may influence the relaxation
in the isochoric contraction by prolonging the
contraction time of some elements in a similar
fashion to that observed by Goffart and
Ritchie with skeletal muscle.s However, none
of the elements must be prolonged beyond the
maximum time of the elements of the normal
heart, or else the total positive tension time
would be prolonged. If certain elements were
prolonged, while others are unchanged, subsequent relaxation would apparently be rapid
as more elements would relax together.
Circulation Research. Vohtmc VIII, July J!)GO
835
EPINEPHRINE IN DIASTOLE
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
The slowing of relaxation during diastole
with epinephrine iu isobaric contractions may
seem at first to be contradictory to the above
conclusions. Lundin,7 however, has shown that
a cardiac fiber in the contracted state can lose
its tension when released, but when subsequently stretched, develops a greater tension
at a given length than the isometric tension
at that length. Thus, a heart contracting with
much force can reach a sufficiently small volume so that most of the tension disappears,
and filling can then commence before the diastolic state is fully established. Onflow would
then lead to a re-establishment of some tension, due to the stretching of fibers. Also,
since epinephrine increases the amount of
tension per unit stretch of contracted fibers,
this would further increase the resistance to
filling so long as there is any residual tension
from the preceding systole. By these means,
filling would be slowed and controlled by the
relaxation rate. In fact, pressure changes
have little effect on the initial relaxation rate
after epinephrine, (fig. 3) or at very low
pressures. At a large volume, however, the
linear stretch of a heart during filling may
be too slow to produce tension if relaxation is
also occurring. For a given flow rate, the rate
of linear stretch would be inversely proportional to the square of the heart's radius (assuming the heart to be spherical). Epinephrine, by accelerating the relaxation rate of
contractile units, would then accelerate the
relaxation rate during filling. A resistance in
the outflow channel would serve to increase
the end systolic volume, and thus, enhance
relaxation.
Increasing the filling pressure, in the preparation without valves, however, would act in
2 opposite directions, since not only will the
outflow resistance increase, but also the inflow rate. This is probably the reason for the
conflicting results using high filling pressures
without valves.
The contraction time is decreased with increasing contraction rates." This would be
expected to accelerate the relaxation rate. By
this means, a heart with a small end-systolic
volume may fill rapidly, even with epinephCirculation Research, Volume VJIT, Jvly 19fiO
vine. At low contraction rates, however, tiie
treppe effect will produce weak contractions
which would have 2 effects on increasing the
relaxation rate: (1) increasing the size of the
heart at the beginning of filling, and (2)
prolonging the ejection time so that filling
only occurs after the residual tension from
the preceding systole is over. There are, therefore, both high and low rates of contraction
that will produce rapid relaxation at least
with some filling pressures.
Summary
Thirty-six isolated frog ventricles were attached to an inflow cannula with stopcocks
that could permit direct systolic ejection back
into the reservoir, return flow back to the
reservoir by another route through a valve,
or isochoric contractions. The heart, enclosed
in a container with a " U " tube outlet, produced pressure changes (extra-cardiac) which
could be used in determining the in-flow rate
and transmural pressures. The rate of change
of the transmural pressure was calculated for
the frog ventricle during early diastole. This
value was taken as a measurement of the rate
of relaxation. The effects of epinephrine (.02
/xg./ml.) Avere studied. At low filling pressures without valves (and therefore with outflow pressure equal to inflow pressure), epinephrine slows the rate of relaxation, although
other inotropie effects, such as an increase in
stroke volumes, are present. If, however, the
heart contracts against a high outflow pressure or resistance the rate of relaxation is increased by epinephrine. The slowing of relaxation in the former case is a result of filling
commencing before relaxation is complete. In
the isochoric heart, epinephrine does not
change the time of positive tension, but does
accelerate the relaxation after contraction.
Summario in Interlingua
Treiita-sex isolate ventriculos do rana ossovii attaeliate a un cannula de influxo con obturatores que
pcrmittcra lo directo retro-ejection systolic a in le
reservoir, lo refluxo al reservoir per un altcre circuito
via un valvula, o contractiones isochoric. Le corde,
includite in un receptaculo con un eflluxo a tubo in
" U , " produceva altcrationcs do prcssion (extra-cardiac) que poteva esser usate in determinar le intensi-
836
HENNACY
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
tate del influxo e le pressiones traiisiuural. Le magnitude del alteration in le pression traiisiuural essev.a
calculate pro le ventriculo del rana durante le eodiastole. Iste valor esseva acceptate eomo mesura del
magnitude del relaxation. Lc effeeto de epinephrina
(0,02 /ig/ml) esseva studiate. A basse pressiones de
rcplenaniento sin valvulas (e assi sin pression de
cffluxo equal al pression de influxo), epineplirina relenta le progrosso del relaxation, ben que altere
effectos iuotropic—conio per exemplo un augmento
del voluinines per pulso—es presente. Tnmen, si lc
conic so eontralie contra un alte pression o resistentia
de eflluxo, le relaxation es promovite per epineplirina.
Le relentaniento del relaxation in le prime de istc
cases cs le resultato del facto que le replenamento
coinencia ante que le relaxation es complete. In lo
corde isochoric, epineplirina non altera le temporo
de tension positive sod accelera le relaxation post,
contraction.
References
1. HENNACY, E. A., AND OGDEN, E.: Factors affect-
ing the filling of the f.rog's ventricle after isotonic contraction. Circulation Research 8:
825, 3960.
2. CLARK, A. J., ET AL.: Metabolism of the Frog's
Heart. London, Oliver & Boyd, 1938.
3. SEGALL, H. N., AND ANREP, G. V.: Isometric con-
traction of the frog's ventricle. Heart 12: 61,
1926.
4. WIGGERS, C. J.: Cardiodynamic action of drugs.
J. Pharmacol. & Exper. Therap. 30: 217, 1927.
5. OFDYKE, B. I"1.: Effect of changes in initial tension, initial volume, and epinephrine on the
ventricular relaxation process. Am. J. Physiol.
169: 403, 1952.
0. BUCKLEY, N. M., SIDKY, M., AND OGDEN, E.: Fac-
tors altering the filling of the isolated left ventricle of the dog heart. Circulation Kesearch 4:
148, 1956.
7. LTJNDIN, G.: Mechanical properties of cardiac
muscle. Acta physiol. scandinav., Suppl. 20, 7:
1, 1944.
8. GOKPART, M., AND EITCHIK, .1. M.: Effect
of
adrenaline on the contraction of mammalian
skeletal muscle. J. Physiol. 116: 357, 1952.
9. CLARK, A. J.: Effect of alterations of temperature upon the functions of the isolated heart.
J. Physiol. 54: 275, 392L
Circulation Research, Volume VIII, July I960
Effects of Epinephrine on Frog Ventricle
RICHARD A. HENNACY
Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017
Circ Res. 1960;8:831-836
doi: 10.1161/01.RES.8.4.831
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1960 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/8/4/831
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/