Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
MODUL 1
Main topics of modul:
1. Fundamentals of aseptic and antiseptic.
2. The apparatus, equipment and organization of the surgical departments.
3. Structure and organization of the operation unit
Main sections:
1. History of question ( Background.)
2. The main sources and ways of spread of infection
3. Hospital (nosocomial) infections.
4. Organization of work of surgical departments.
5. Cleaning of the surgical Department.
6. The purpose of the basic premises of the operational unit.
7. Prevention of contact of the implant and endogenous infection
8. Sterilization dressings, surgical linen.
9. Processing of hands.
10. The process of donning on surgical clothing
11. Prevention of endogenous infection.
12. The problem of AIDS in surgery.
13. The problem of viral hepatitis in surgery.
Lecture course module topics.
ASEPSIS. Antiseptics (Part 1)
Historical Review.
Organization of work of the surgical Department
Any surgery is accompanied by a physical intrusion in the internal environment of
the body and destruction of the barrier, that separates the the body of the
patient from the external environment. The operation, which is intended to cure
the patient, may present a threat to life. One of the dangers with which the
surgeon found during surgery, is the penetration of infection in the body. The
development of infectious complications can lead to death, despite well-executed
surgery. Therefore, the prevention of development of infectious complications is
one of the basic principles of surgery. The success of modern surgery would be
impossible if it was not developed methods to combat microorganisms that cause
the development of severe infectious processes in the operating wound.
Any surgeon in his work is faced with two problems:
- the need to avoid the penetration of microorganisms during operatsii the body
of the patient.
- the need to control microorganisms in the case that began to develop infection.
The solution to these problems is a difficult task and can be carried out by
application of complex of preventive and therapeutic measures. The set of
methods aimed at prevention and elimination of micro-organisms caught in the
body is united by the concepts of aseptic and antiseptic.
ASEPSIS - is a complex of preventive measures aimed preventing the spread of
infection in the wound in the body of the patient creating a sterile environment
for a surgical operation through the use of organizational measures, chemical
substances, physical factors.
ANTISEPTIC- a complex of measures aimed at the destruction of microorganisms
in the wound, the pathological focus in organs and tissues, as well as in the body
as a whole, through the use of chemical, biological, mechanical and physical
factors.
The terms aseptic and antiseptic of Greek origin. Translation: antiseptic - anti against, sepsis - rotting; aseptic - and - a negative particle, sepsis - rotting. Thus,
methods of aseptic provide microorganisms entering a warning into the body of
the patient, and antiseptic techniques aimed at the destruction of the microbial
factor that has entered the wound or tissue. However, in some cases the
distinction between aseptic and antiseptic difficult. Aseptic and antiseptic
represent a single set of measures, they can not be divided. This is due to the fact
that aseptic and antiseptic directed to combating infection and are often based
often based on the the same methods of influence on microbial cell, use the same
antiseptic factors (antiseptic).
History of the question
Science passes certain stages of development. Root revolution in surgery came
with the introduction of antisepsis and asepsis, divide the whole history of
surgery on for up antiseptic and antiseptic periods. The introduction of aseptic
and antiseptic opened a new era in the development of surgery. Currently,
aseptic and antiseptic is foundations upon which the surgery.
It is believed that asepsis and antisepsis arose in the late 19th century. However,
the origins of the struggle with purulent infections back to ancient times. In
ancient ancient times, it was known much that now no one remembers. Even
Lucretius Carus, who lived in the first century BC put forward the idea of the
existence in nature of tiny, invisible “seeds”, some of which are pathogenic and
cause infectious diseases. For ten centuries BC professional surgeons disinfected
surgical instruments, passing them through the flame. heating on fire, washing
with hot water and the juices of plants. About antiseptic substances mentioned in
the writings of Hippocrates. He washed the wound only boiled water, used in the
treatment of linen bandages, which are well absorbed from the wound discharge .
The bandages he was soaked with wine to enhance the action disinfecting. It was
millennia before the beginning of the antiseptic era of medicine. In the middle
ages, the French surgeon Henri de Mondeville (1320) insisted on stitching of
wounds to avoid their contact with air, which was considered the source of
infectious origin. His compatriot, Guy de Chauliac (1363) in the treatment of
wounds used alcohol, vinegar, tar. Because of this, even in those days, the
wounds are often healed by primary intention, i.e. without suppuration.
Unfortunately, until the 19th century, these proposals have not been popular
with surgeons, and the development of septic complications was perceived as
inevitable. Up to 70-80 gg the last century it was possible to observe that after
simple operations the wounds were festering, and in most cases, patients died.
During this period, the majority of the operated patients died in connection with
the development of purulent and septic complications of surgical wounds, the
causes of which were unknown. During the Crimean company,1854-1855 , every
second person injured who was taken to hospital died of the infectious process.
High mortality rates were in the stationary civilian hospitals. According Malgenya
in 1850 in Paris from 560 hospitals operated 300 people died. According to the
report of hospital Pirogov Surgical Clinic in 1852-1853 gg. 159 of the 400 patients
died operated. Fatal in the majority of cases were associated with infectious
complications operations. Surgeons almost never took risks and did not carry out
operations related to the opening of the cavities of the human body, as the
intervention in these cavities gave almost one hundred percent mortality of
surgical infection. The reason for such a large number of complications was the
fact that surgeons knew nothing about the infection and the actions they
themselves contributed to its introduction into the wound, themselves provoked
the sad outcomes of their brilliant on technique of operations.
The largest Russian surgeon Villaminaya describes what happened in the
surgeon's clinic Basov in Moscow: "What we've seen at this clinic? - Amazing
technique, such what is now, perhaps, not to see ... and Pius, septicemia (blood
infection), erysipelas, sometimes diphtheria wounds ... gnoekrovie, hospital
gangrene and tetanus sometimes.
High mortality rates were in the stationary civilian hospitals. According Malgenya
in 1850 in Paris from 560 hospitals operated 300 people died. According to the
report of hospital Pirogov Surgical Clinic in 1852-1853 gg. 159 of the 400 patients
died operated. Fatal in the majority of cases were associated with infectious
complications operations. Surgeons almost never took risks and did not carry out
operations related to the opening of the cavities of the human body, as the
intervention in these cavities gave almost one hundred percent mortality of
surgical infection. The reason for such a large number of complications was the
fact that surgeons did not know anything about the infection and the actions they
themselves contributed to its introduction into the wound themselves provoked
the sad outcome of his brilliant technique for performing operations.
The largest Russian surgeon Villaminaya describes what happened in the
surgeon's clinic Basov in Moscow: "What we've seen at this clinic? - Amazing
technique, such what is now, perhaps, not to see ... and Pius, septicemia (blood
infection), erysipelas, sometimes diphtheria wounds ... pus spread, hospital
gangrene and sometimes tetanus .
Bass operated in uniform , most old, just rolled up their sleeves. During
operations of a ligature (i.e. threads for the ligation of vessels) removed one of
the paramedics, due to anything soaked lapel of his jacket. Needle with red silk
adorned immediately on the table, stuck in a tallow candle, which served to
lubricate them and silk to the needle and silk to glide easily through fabric. The
same picture describes the famous Kharkov Trinkler surgeon in the clinic Grube.
He says that the threading of silk thread in the needle, was charged paramedics
performed in advance, and the tips of the thread, for better passage in the ears,
or bites, or moistened with saliva.
Now we understand that in these conditions, the little incision opened the gates
for infection. Together with the sicks died, and many surgeons. Accidental scratch
or prick of the finger during the execution of purulent surgery was cost life of
surgeon.
Nikolay Ivanovich Pirogov, one of the last representatives before the antiseptic
era in surgery sadly wrote: “If I look back to the cemetery, where infected in
hospitals, I don't know what's more surprising, the stoicism if surgeons in even
the invention of new operations or the trust and confidence that continue to use
the hospitals, the government and society.”
The surgeons had then a reliable methods of prevention of sepsis and the
treatment of infected wounds. The best minds of the time tried to find an
explanation for the failure of the surgeons.
Advanced surgeons of the era, had a strong thought about getting some started
from outside the wound. In the eighteenth century, surgeons were identified
purulent septic complications from rotting due to exposure to the wound air. So
they recommended to apply an occlusive, airtight bandage, in order to limit the
time of exposure to air (especially "unclean") on the wound. The English surgeon
Benjamin bell were advised to make the dressings as quickly as possible. His
compatriot Pringle believed that for air purification it is necessary to better
ventilate the hospital premises. French surgeon PUTEAUX established facts of
contact infection of wounds. Purulent wound discharge from one patient when
hit in the wound of the other causes of purulent inflammation. Wound infection
also occurs when using the dressing material, used, or material contaminated
hands, contaminated with bad air sick." A German doctor of Henle in 1840
suggested the presence of a living contagious, which is transmitted by contact. N.
I. Piwigopress to the conclusion that the source of infection is the pus of wounds,
getting to her through the dressing, care items and personnel. Even three years
before Joseph Lister in 1864 he wrote: “we Can safely say that most of the
wounded dying not so much from the injuries as from a hospital infection.. . From
us close to the time when a thorough study of traumatic and hospital miasma
(Greek “miasma” – pollution) will give surgery another direction,” and then ...
“purulent infection spreads not only through the air, which is obviously harmful
only when occuring wounded in an enclosed space, as the surrounding objects:
linen, mattresses, dressings, walls, floors, and even sanitary staff”.
N. I. Pirogov tried to solve the problem of prevention of surgical infection
requiring device "special compartments" for infectious patients, he isolated
patients with gangrene of hospital in a separate room. Put forward demands to
separate the gangrenous offices, to give them special dressings, and special
surgical instruments. In addition, N. I. Pirogov in the treatment of wounds before
Lister used to disinfect alcohol, silver nitrate and iodine. V. A. Oppel wrote: "Pie is
actually knocking at that door, behind which was a scope surgery, he toyed with
the thoughts on the prevention of infectious complications, but has not made a
final conclusion . ".
A maternity ward, where a leader was a professor Земмельвейс, was not better
and not worse than any other separation in any other hospital of the world. And
nobody of professors took no notice on such fact: why women, who give birth
whith assisted by midwife died much rarer, than those, that came running to the
help of professors and students. A secret opened up simply, and opening of this
question treated him expensive. Midwifes knew healthy womans giving births,
healthy babies only. And anymore with anybody did not have business: not with
those, who had festering inflammations, nor with those, who was ill a maternity
fever nor with those, that already perished from her and who was unsealed on an
anatomic tables. This was done by professors . From contagious festering
patients, from an anatomic theatre they passed to the maternity table, and a
single touch of their hands was enough to make a healthy woman who had just
became a mother , condemn to death . In 1847 in a clinic, where Semmelweis
worked, suddenly a pathologist died: at necropsy he cut a finger. Semmelweis
was present on dissection of colleague and saw the same picture that so much
times looked after at dissection of the dead from a maternity fever women. Death
of pathologist came, as Semmelweis understood, from an infection a ptomaine.
Young mothers perished from the same infection. They did not know the causes
of puerperal fever. Empirically, Semmelweis concluded: Now, before, go to the
maternity, it carefully for a few minutes, scraping brushes, hands and drenched
them in a strong chlorine solution. His hands, of course, spoiled, delicate and
sensitive hand surgeon, skin on them Grubel and cracked; but the death rate in
his department immediately dropped ten times. From only one careful hand
washing! In addition, he restored order in the maternity hospital. It was a huge
win. And Semmelweis was schastliv.He persuading doctors of Vienna to follow
the example, But doctors mixed Semmelweis with mud.
They shouted that "all these inventions do not have any scientific basis that the
surgeon's hands - well-groomed hands - spoiled by a long washing and especially
by chlorine water ; puerperal fever that occurs by itself and no one, not a single
soul in the world would dare to blame the doctors, which are the most humane
people on earth. What nonsense - wash hands because of non-existent infections:
the fruit of imagination that maniac ... ". Fruit of the imagination ", which could
significantly reduce their income, . All of the innovations that have entered
Semmelweis ,made an alarm in the minds of current and future patients and their
husbands.. To surrender to his demands - is to recognize that he was right,
including the validity of the charges in the murder of ignorance. No, no they will
not allow changes. And Semmelweis should expel from the hospital to continue to
nobody povadno was to break the usual ages steady flow of life and medical
practice.
"Things are moving" only after the great discoveries of Louis Pasteur in 1863,
proved that the cause of fermentation and putrefaction bacteria are trapped
outside. He found that these processes occur as a result of vital activity of
microbes and stop them can only live by killing pathogens.
Pasteur who was not a doctor, rightly praised the importance of his discovery for
surgeons. Addressing the members of the Paris Academy of surgery in 1878, he
said: “If I had the privilege to be a surgeon, aware of the danger which threatened
the germs of the microbes present on the surface of all objects, particularly in
hospitals, I would not stop caring for all the instruments before each operation I,
first, carefully washed my hands and then held them for a second over the flame;
lint, bandages and sponges previously warmed up I would in dry air at a
temperature of 130-150; I never used water without first boiling it at a
temperature of 110-120. Thus, the wound could get only the germs that are in
the air near the patient's bed. The number of these microbes is quite insignificant
compared to those that are on the surface of various objects and in the most
clean drinking water.. . ”.
Paster with brilliant insight correctly identified not only the basic principles
(everything that comes in contact with the wound must be clean), but the basic
methods are established after surgical asepsis, to ascertain the relative
importance of aerial and contact infection of wounds and, in addition, absolutely
correct, in modern, much deeper than many of his followers have formulated the
role of the relationship of micro - and macro-organisms in the pathogenesis of
surgical infection.
The first surgeon who have had the ideas of Pasteur in surgical practice and
created the first, based on the scientific basis of the system of infection
prevention, who gave a quick practical effect was the English surgeon Joseph
Lister (1827-1912) He came to the conclusions, that the microorganisms get into
the wound from the air and from the hands of the surgeon.
John Lister based his system fight against infection of wounds put the idea of the
destruction of microorganisms by chemical means, having chosen as antimicrobial
agent 2-3% solution of phenol (carbolic acid).
Making sure the antiseptic action of carbolic acid in Glasgow in 1865, he applied
the bandage in the treatment of open fracture and sprayed carbolic acid in the
operating theatres. In the historical work “On a new method of treatment of
fractures and ulcers with remarks on the causes of suppuration” (1867) Lister
stated basis for his proposed antiseptic method. Later Lister had perfected the
technique, and in full it included for a whole range of activities. Antiseptic of
Lister's activities included:
• spraying carbolic acid in the air of the operating
• handling of instruments, suture and dressing material, as well as the surgeon's
hands 2-3% solution of carbolic acid;
• treatment with the same solution of the surgical field;
• the use of special multilayer bandage soaked in carbolic acid
He has allocated for operating a special room, which was maintained maximum
purity in the air of the operating room during surgery using special sprayer (spray)
made by spraying a 3% solution of carbolic acid Spray is a unit, which was sprayed
a solution of carbolic acid. This solution not only saturated the air in the operating
room, but was treated with the surgeon's hands, operating field, instruments for
dressing and bandaging material. The trinkler, describing the method of Lister,
remembers that “there was a time when operating in the heat of passion
antiseptical was a real steam bath, where surgeons was choking from the tight
saturated vapor of carbolic acid: solutions of buckets poured on the sick and
wounds. Everything was swimming...”
Nesterovskaya bandage consisted of several layers.
• fine silk, impregnated with 5% carbolic acid with a resinous substance;
• eight layers of cheesecloth soaked in a mixture of carbolic acid with rosin and
paraffin;
• rubberized cotton fabric or mat;
• bandage impregnated with a solution of carbolic acid.
To apply it is not for therapeutic purposes, as well as a prophylactic to prevent
penetration into the wound of the infected air.
Efficiency Lister System proves conclusively decrease in deaths from several times
suppurative complications. Its use has improved the results of surgical operations
and ushered in a new era in the development of surgery.
Thus, the merit of John Lister is that it is not just used antiseptic properties of
carbolic acid, and created a solid way to fight infection. Therefore, it is considered
the founder of antiseptic. The key to his method was disinfecting chemical
methods that come into contact with the wound. The main point of his teaching
was the thesis "Nothing should touch the wound, without being
obesplozhennym". In fairness it should be noted that all the elements of the
antiseptic method of Lister, with the exception of air spray, formulated I.
Semmelweis relation to obstetric practice.
Pioneers antiseptics in Russia were Pelehin (St. Petersburg), Burtsev, Levshin
(Kazan), Sklifosovsky (Moscow), Grube (Kharkiv) and others.
PP Pelehin studied antiseptic directly from Lister, but in the first years of the
method, when Lister is not yet fully designed their ideas. Pavel Petrovich Pelehin
began fervently preach antiseptics. He is the first article, published in Russia,
dedicated to the topic. Pelehin shaved his mustache, hair and even his eyebrows.
But at the same time in its operating drank tea, smoked and examined the urine.
The method of Lister was supported by a number of major surgeons of the time.
But there were irreconcilable opponents. Famous Kiev surgeon Karavaev ironically
treated antiseptic method . Going to the operating room and watching the action
, he invariably said, “Well, the parrot of these animals’. Famous surgeon Theodor
Billroth ironically called antiseptic method "listerianum".
Wide application of the method of Lister identified deficiencies. Uses
solutions of carbolic acid, except
positive, had a negative effect – caused General intoxication of patients, the burn
of the tissue in the wound area, kidney disease, disease of surgeons (dermatitis,
burns, eczema of hands). Attempts to replace carbolic acid with other substances:
solutions of corrosive sublimate, boric or salicylic acid, potassium permanganate,
etc. showed that the stronger antimicrobial effect of the means employed, the
more pronounced toxic effect on the body they have.
Surgeons gradually began to abandon the method of Lister, as in its application
died not only microbes, but also living tissue. Schleich compared to antiseptics of
the time with a gun, one barrel of which is directed forward and the other back
and every shot with a single bullet strikes the enemy (germ) and other (tissue).
The method of Lister lasted about 15 years. Quickly abandoned the use of spray,
Lister multilayer bandage, the introduction of strong antiseptics into the wound.
Despite the fact that the proposals methods Lister have been forgotten, his
merit is that he first developed and applied a set of measures aimed at combating
infection. The figurative expression of V. A. Oppel, inestimable merit of Lister is
that he “opened wide before surgeons the door of human suffering. Like a
hurricane, broke in the door of the surgery and have done wonders.”
Further development of Microbiology, the work of L. Pasteur and R. Koch, showed
that destruction of microbes can be achieved using high temperature, and this
method is more reliable, than use of chemical substances.
Replaced the antiseptic method, came the aseptic. The main principles were: to
prevent contamination by microorganisms of the surgeon's hands and all items in
contact with the wound. To surgery came the processing of surgeon's hands ,
sterilization of the instruments, the dressing material, linen etc. The main merit
in the development of the aseptic method belongs to Ernst Bergman, the
Professor of Dorpat and then at the Berlin universities, his student K.
Shimmelbush. Professor Bergman has performed and published a number of
studies on putrefactive infection. His method of aseptic technique was based on
the destruction of microbial flora by high temperature (boiling, hot steam, etc.),
on all objects in contact with the wound. E. Bergman began to promote the idea
of asepsis and with tireless energy was introduced asepsis, both on the field of
hostilities and a peaceful environment. The merits of Professor Bergman in the
introduction and promotion of aseptic technique are so great that he is
considered the father of asepsis. In 1886 an employee of the Professor in
Bergman's Shimmelbush has been designed sterilizer for boiling instruments,
where in order to protect surgical instruments from corrosion was applied 1%
solution of soda. Still used for sterilization bix bears his name - Bix shimmelbush
X International Congress of surgeons in Berlin in 1890 E. Bergman has
demonstrated patients operated in aseptic conditions, without the use of
antiseptics nesterovskay. Since then, the asepsis has received universal
recognition. Here was formally adopted its basic tenet: "Everything that comes in
contact with the wound must be sterile". Presided over the Congress John. Lister.
Despite the fact that asepsis forever consign to oblivion his antiseptic method He
correctly assessed the work of E. Bergman and congratulated him on his great
success, calling aseptic technique brilliant conquest surgery.
prevention system entry of microorganisms in wounds created by Bergman and
Shimelbushem has been very perfect, gave excellent results and in its main
features preserved to date.
It should also remember the name of assistant professor of surgery Gustav
Neuber, who in 1884-1891 was the head of a private surgical clinic in Kiel. He well
understood the new requirements imposed on the surgical clinic, and the first
time allocated a separate operating for septic operations
Since 1892 aseptic techniques became widely implemented in many clinics
around the world. Surgeons, correctly assessed the value of the works of Bergman
and Shimelbusha, we put a lot of efforts in the further development of aseptic
techniques.
R. Koch and E. Esmarch offered flowing steam sterilization method. In Russia, LL
Geidenreich designed steam sterilization under high pressure and in 1884 he
proposed the use of an autoclave for sterilization. This method proved to be more
perfect. In view of the aseptic requirements gradually evolved structure operating
and dressing. Mikhail Subbotin and LL Levshin created operating, which
essentially became the prototype of the modern. NV Sklifosovsky first proposed
to allocate for operational transactions, which differ in their infectious
contamination.
The results of the application of aseptic techniques were so successful that some
surgeons began to call to completely eliminate antiseptic agents of surgical
practice and to abandon the antiseptic method. Priority was given to methods of
aseptic and antiseptic questions were referred to the background. But this
misconception was soon abandoned. Heat can not be used for treatment of living
tissues, the treatment of infected wounds. Therefore completely dispensed with
antiseptics in surgery was impossible.
The processing of the surgeon's hands , the surgical field, debridement of
purulent wounds. it is impossible to produce without antimicrobials . Due to the
success of chemistry has a new low-toxic antiseptic. They were used for the
treatment of hands, the operating field, surgical instruments and other patient
items. Gradually, asepsis closely intertwined with antiseptics.
Opening and introduction of methods of asepsis and antisepsis has determined a
qualitatively new stage in the development of surgery, was developed aseptic
period. Theodore Billroth, in his time, has been a negative attitude to the
antiseptic of Lister in 1891. said, "Now clean hands and a clear conscience
inexperienced surgeon can achieve better results than before with a famous
Professor of surgery". This statement of the famous surgeon far from the truth.
The ordinary modern surgeon, having the methods of asepsis and antisepsis, the
patient can have a much greater help than surgeons of the mid-19th century.
As can be seen from the foregoing, in the history of surgery in parallel developed
two ways of dealing with a surgical infection: the destruction of microbial factor,
trapped in the wound or body tissues, called an antiseptic, and preventing ingress
of germs into the wound is aseptic. This circumstance was not accidental, as
asepsis and antisepsis aimed at combating infection, and is often based on the
same methods of influence on microbial cell, i.e., use the same antiseptic factors
(antiseptic). It is currently impossible to share the asepsis and antiseptics. The
section of surgery, on which is based the whole modern surgery.
ASEPSIS
Asepsis- is a complex of preventive measures aimed at the preventing of infection
hit in the wound in the body of the patient, creating a sterile environment for a
surgical operation through the use of organizational measures, chemical
substances, physical factors.
Modern asepsis is based on two main principles:
1. Everything that comes in contact with the wound must be sterile.
2. All surgical patients should be divided into two streams: the "clean" and
"purulent".
THE MAIN SOURCES AND WAYS OF SPREAD INFECTION
For effective prevention of infection in the wound and the body of the patient,
you must first know its sources and ways of distribution. Under the source of
infection understand the habitat, development, and reproduction of
microorganisms. In relation to the patient's body (the wounded) to distinguish
between two basic kinds of sources of infection - endogenous and exogenous.
Exogenous – sources outside the patient's body. Endogenous- is the sources in
the body of the patient.
The main exogenous sources: 1) patients with purulent-septic diseases, 2) bacilli
carrier, 3)animals. It should be remembered that the danger for the surgical
patient can present not only pathogens, but also opportunistic, and saprophytic
bacteria, which are on surrounding objects. From patients and bacilli carriers or
microorganisms fall into the environment from mucus, sputum, pus, and other
secretions. Less common sources of surgical infection are animals. From external
infection in the body can go several ways - by air, droplets, contact, implant.
1. Air path. The microorganisms pass from the surrounding air, where they
are the freely suspended or adsorbed on dust particles. Air, as a means of
transmission plays an important role, especially in operating rooms,
resuscitation departments and intensive therapy.
2. Drip path. In to the wound penetrate the pathogens contained in the
smallest droplets of secretions from the upper airway into the air, when
talking, coughing, sneezing.
3. The contact path. Microorganisms get through objects in contact with the
wound in the process of operations or other manipulations (the surgeon's
hands, instruments, dressings, etc.);
4. Implantation path. The pathogen enters into the tissues of the body in the
case of willful abandonment there is foreign material (suture material,
metal rods and plates, artificial heart valves, synthetic vascular prostheses,
pacemakers, etc.).
Endogenous infection is inside the body or on the surface of the skin. The main
endogenous source of infection are: 1) inflammatory processes of the
integumentary epithelium (furuncles, carbuncles, pyoderma, eczema, etc); 2)
focal infection of the gastrointestinal tract (dental caries, cholecystitis,
holangit, pancreatitis, etc); 3) infection of the respiratory tract (sinusitis,
frontal sinusitis, tracheitis, bronchitis, pneumonia, bronchiectasis, lung
abscesses); 4) inflammation of the urogenital tract (pielity, and cystitis,
prostatitis, urethritis, salpingo); 5) lesions is unknown (cryptogenic) infection.
Major pathways for endogenous infections are contact way , hematogenous,
lymphogenous. When of the contact ways microorganisms can get into the
wound: from the surface of skin in close proximity of operating cut, from the
clearance of organs that has been unsealed during an operation. (e.g.
intestines, stomach, esophagus, etc.) from the inflammatory focus located in
the area of operations. At hematogenic or lymphogenic ways,
microorganisms can fall into the wound via the blood or lymphatic vessels.
To successfully fight the infection, you need to implement it at all stages, the
source of infection-route of infection - the patient's body.
HOSPITALIC (INSIDE THE HOSPITAL) INFECTION.
Hospital (nosocomial) infection - is an infectious disease caused by infection
of the patient, which occurred during his stay in the hospital. Currently, the
development of purulent-septic diseases caused by hospital acquired
infection, is regarded as an iatrogenic complication, as is due to flaws and
errors in the work of health workers.
Hospital (nosocomial) infection - is a serious problem of modern surgery.
Despite the improvement methods of asepsis and the emergence of modern
powerful antiseptics, until now ,to completely avoid septic complications is not
possible. This is due to the fact, that the inside hospital infection has a
number of features.
At first, the infections agents are usually opportunistic microorganisms
Secondly, the main pathogens resistant to most antiseptic means.
Thirdly, the possible outbreaks of purulent-septic diseases with similar clinical
picture caused by a single strain of microorganisms.
Fourth, often develops in immunocompromised patients.
Modern hospital acquired infection in surgical clinics cause various
microorganisms, sometimes antibiotic-resistant (strains of Staphylococcus
aureus, Pseudomonas aeruginosa, Proteus, Escherichia coli, Klebsiella, fungi
Candida, etc.); clinically they are manifested mainly with sepsis syndrome and
septic lesions. Sources of nosocomial infections in surgical hospitals are
patients with acute and chronic forms of purulent-septic diseases, or
asymptomatic carriers of pathogens (including medical staff).
The latter are of great importance, to take into accounting the spread of
pathogens of nosocomial infection occurs mainly by airborne droplets (the air)
and the contact (hands, clothes, dressing, instruments, equipment, and so on.
D.) ways.
Zones of increased danger are infectious wards and department of surgical
infections, "dirty"areas of operation units : laundry and toilets, showers and
wash basins in general hospitals, particularly in pediatric wards and intensive
care units.
To prevent and control the spread of in-hospital infections developed a set of
sanitary measures aimed at the identification and isolation of sources of
infection and interruption of transmission paths. Among other, activities it
involves timely detection of bacilli carrier and sanitation of foci of chronic
infection, the use of highly effective hand decontamination methods of
medical personnel handling the surrounding objects (bedding, soft equipment,
footwear, tableware and so on. D.) With epidemiological importance in the
mechanism of transmission of nosocomial infections. In practice, the fight
against nosocomial infection - is a conscious behavior and uncompromising
control in all departments of the hospital, especially in surgical wards, strict
implementation of measures aimed at compliance with the hospital hygiene,
antisepsis and asepsis.
Among the activities to combat in-hospital infection should include and
shorter hospital stay, early discharge of patients to outpatient treatment.
Prevention of Air and respiratory infections
Air -droplet infection -causes 10% of infections of surgical patients. To prevent
it applies a set of measures, including arrangements relating to the feature of
the surgical wards and the hospital as a whole, and measures aimed at
reducing air pollution and the destruction of micro-organisms already present
in the bacteria therein. Effectiveness measures for the prevention of airborne
infection in surgical departments and operating units depends on the devices
and equipment, work in them and implementationof measures aimed at
reducing the pollution of air microbes. Of particular importance is played
arrangements, they are crucial.
DEVICE, EQUIPMENT AND ORGANIZATION of the surdical departments.
Keeping of rules of an asepsis are the fundamental principle at the
organization of a surgical hospital. It is necessary to create a maximum of
conditions for safe realization of operations, carrying out inspection and
postoperative patient care. The basis of the surgical departments is one of the
basic principles of asepsis - the division into "clean" and "purulent" patients.
Any modern methods of prevention and control of infection will be ineffective
if there in the same room will be clean postoperative patient and the patient
with septic disease. The rule of division of patients into "clear" and "purulent"
is applied both at arrival of the patient in a hospital, and during treatment,
when determining a sequence of operations, bandagings or other
manipulations.
Depending on a type of medical institution this question is solved in the
different ways, but division of these categories of patients is fundamental
maximal.
If in hospital only one surgical department, then in it chambers for purulent
patients are expressly allocated. Will surely organize two dressing rooms: clear
and purulent, and purulent have in the same wing where there are chambers
for purulent patients. For work with this category of patients must allocate
express personnel, will organize a separate sisterly post. In case in hospital
several surgical department, then surely allocate purulent department.
Respectively more narrow at hospitalization, there is a division of patients that
interferes with the relative becoming infected among them. Division of
patients into "clear" and "purulent" happens also in office. First of all more
clear operative measures are carried out, bandagings are carried out taking
into account of patients.
The main structural divisions of any surgical hospital are medical and
diagnostic offices and a surgery block. In large medical institutions the
separate operational office can be created.
Device medical-diagnostic departments
The surgical Department needs to be on the ground floor. This is to some
extent creates isolation. In departments expansion of chambers which number
depends on its power is provided. Except chambers there have to be
administrative (sisterly, a staffroom, an office of the manager of the
department and an office of elder sister), medical and diagnostic (dressing,
handling,gypsum ), subsidiary (laundry, the dining room, a still-room, pantry , a
bathroom, bathrooms for personnel and patients) rooms. Sisters post is
allocate at 20-30 patients. It is known that at receipt in a hospital only at 5%
of clean surgical patients pathogenic microbes are detected . In a month later
– at 70%, and 1,5 months later is more narrow at 100% of patients. Therefore
it is expedient to place patients in chambers, grouping them taking into
account receipt time.
The area of chambers of all-surgical office is defined at the rate of 6, 5-7, 5
sq.m on one bed with a room height not to exchange of 3 m and width not less
than 2,2 m. Small chambers on 2-4 beds (the insulator – on 1-2 beds) equipped
with a separate bathroom are most convenient. Orientation of windows of
chambers and medical and diagnostic offices has no keyest value, but the ratio
of windows and a floor has to be 1:6, 1:7. For a facilitation of carrying out
cleaning floors have to be covered with a linoleum, a tile or to be aspics. Walls
are painted by oil color or become covered by a tile. In dressing rooms also
ceilings become covered with oil color. Temperature has to be maintained 1820•C, humidity of 50-55%. The furniture for all premises of office has to meet
the requirements: 1) to be convenient for the patient, 2) to facilitate to
personnel patient care, 3) easy to move, 4) to be convenient for contents it in
purity, 5) not to spoil from washing and the wet disinfection. The quantity of
furniture has to be sufficient, but not excessive.
Cleaning of the surgical Department
The device and the equipment of surgical office has to be such that it was
possible to make multiple cleaning easily. The wet cleaning is made twice a
day, in the morning and in the evening.When carrying out wet cleaning can be
applied to various antiseptics (hydrogen peroxide, chloramine, anolyte).
Obligatory element of sanitary and hygienic actions- is the wet cleaning of
furniture, processing of objects of patient care. An important measure of
prophylaxis of a droplet infection is airing of rooms. It has to be carried out
according to the schedule. Only airing lowers an air obsemenennost by 30%.
Besides, all chambers and medical and diagnostic rooms are equipped with
germicidal lamps.
The mode of operation of the surgical Department
In surgical office the high sanitary and hygienic security has to be kept. Access
for visitors or other strangers has to be limited.
It is necessary to remember that the medical personnel of surgical offices can
also become an infection source. It can be caused by two circumstances:
violation by medics of rules of hygiene and existence of carriers of bacilli
among them. Therefore special requirements are imposed to the staff of
surgical offices.
Every employee arriving for work in the Department of surgery, undergoes a
complete medical examination (including dental examination and
consultation, a bacteriological swab from the nasopharynx mucosa for the
presence of pathogenic Staphylococcus),instructing on the main sanitaryepidemiological activities. The medical personnel must be put on a dispensary
upkeep and once a quarter have careful examination. Carriers of bacilli
(persons almost healthy, but allocating in a surrounding medium a pathogenic
microflora most often from a nose, a pharynx) are discharged of work and
carry out the corresponding treatment. Only after bacteriological monitoring
they are allowed to work.
In case of the outbreak of an intrahospital infection extraordinary surveys of
medical personnel will be organized.
Hygiene of medical personnel. Hygiene of medical staff is based on first of all
on exercise of increased requirements to personal hygiene. A primal problem
of personal hygiene of medical personnel is maintaining of a hygienic condition
of a body. The periodic of hair clippers and nails. Daily toothbrushing and
rinsing of a mouth. In a cut-in the hygienic douche, change of clothes and linen
is desirable. In operating time in deprtment, it is necessary to use overalls. All
workers have to have removable footwear, dressing gowns, or the express
suits from light fabric which are regularly undergoing washing. An obligatory
element of clothes is the cap. The medical cap has to close head indumentum
completely since in hair settles dust and hit of microorganisms in a wound, on
tools, a dressing material is possible. An exit in overalls out of limits of
department is not allowed. Health workers in department have to pay an
attention to keeping of rules of hygiene and rules of an asepsis during the
immediate work with patients. It is necessary not only not to promote a
transmission of infection from the patient to the patient, but also to avoid
infection.
After survey of the patient, a research of wounds or change of bandages,
disinfection of rooms, and also hygienic procedures the personnel wash hands
with warm running water with soap within 2 minutes. For washing of hands
use a toilet soap in shallow packaging on one procedure. Frequent washing of
hands of medical staff in surgery – the most important principle of hospital
hygiene of a surgical hospital. After contact with infectious contents, the
medical workers disinfect hands solutions of germicides.
As a means for disinfecting hands is used 76% ethyl alcohol, 0.5% solution of
chlorhexidine of digluconate in 70% alcohol or 0.5 % (0.125% of active
chlorine) chloramine solution. During the disinfection of the hands with ethyl
alcohol or chlorhexidine the drug is applied on the Palmar surface of the brush
in the amount of 5-8 ml (one teaspoon) and RUB the skin for 2 minutes.
Hygiene patients. A required element for proper sanitary conditions in the
Department is the personal hygiene of patients. Medical personnel must
monitor this and, if necessary, to assist patients who are unable to perform
hygienic procedures themselves.
THE DEVICE AND ORGANIZATION OF WORK
THE OPERATING UNIT
The operating unit is a complex of special areas of the surgical Department
intended for performance of operations and activities for their welfare.
Operating unit is a "Holy" place surgical hospital, this is the main stage of
treatment for surgical patients (op) and the quality of its performance largely
depends on the result of the treatment. Therefore, this unit of the surgical
Department special requirements. In the organization of the operating unit,
remember that its main purpose is to create the most favorable environment
for operations at a maximum reduction of the risk of entry of exogenous
infection in the operating wound. Therefore, the main requirement for the
device is maximum isolation from other units of the hospital.
The location of the operating unit
The operating unit must be located on a separate floor or in a separate wing,
connected by a corridor with the surgical Department. The best option, if it is
placed in the isolated Annex or separate building connected with the main
body passage. To avoid the influence of adverse environmental factors (noise,
air pollution, etc.) to position the operating unit on the upper floors above the
second. The best orientation of the Windows in our latitude is the North or
North-West. This avoids, first, the direct sun rays that are reflected from shiny
walls, floor and tools that make the job of surgeons, and secondly, overheating
of premises in summer months.
Operating units for “clean” and “purulent” operations should be placed
separately. If in the hospital one operating unit, select the operating to
perform a clean and contaminated operations, the most dividing and deleting
them. They must work with different staff and used different equipment,
surgical tools, linen. Despite the fact that in purulent operating operations are
performed in patients with already developed purulent-septic diseases, the
requirements for their layout, facilities and mode are the same as clean.
Despite the desire for maximum isolation of the operating unit should ensure
good communication with the Department of resuscitation and intensive care,
specialized diagnostic and treatment departments.
The layout of the operating unit
For the normal functioning of the operating unit required the following groups
of premises:
1. Operating room (operating rooms, anesthesia, hardware, preoperative,
chamber of awakening);
2. Staff quarters (sanitary inspection room surgeons, nurses, anesthesiologists,
operating older sisters, Protocol);
3. Utility rooms (Laundry, material);
4. Production facilities (premises procurement of dressing material, tooling,
autoclave, sterilization, Central sterilising Department).
Sterile in the operating mode is provided primarily by preventing the entry of
microorganisms into the operating room from other spaces and their
distribution in the operating room. To ensure aseptic conditions when
performing surgery, prevention of air pollution and areas in the vicinity of the
wound when planning the operating unit abide by the principle of zoning. It
involves dividing areas into special functional areas. In the operating unit
providing 4 zones of sterility:
1. Zone of sterile regime.
2. Zone of strict regime.
Z. restricted Area mode.
4. Area mode took place (not sterile).
To the area of the sterile mode (1 zone) are areas in which operations are
performed is the sterilization of surgical instruments: surgical, sterilization. In
rooms of this zone, most stringent requirements of aseptic.
To the high security zone (2 zone) includes facilities directly associated with
the door operating, preoperative, anesthetic. With the premises of the third
zone, they are linked by an internal corridor.
To the area limited regime (zone 3) includes all other areas within the clean
area of the sanitary inspection (instrumental, material, laboratory for urgent
tests, the hall of awakening patients, facilities, nurses, surgeons, Protocol, etc.)
Took place to the zone mode (zone 4) – includes premises located outside the
sanitary inspection or a special platform (gateway)- office head, office head
nurse, space for dirty Laundry.
The purpose of the basic premises of the operational unit
Operating. Designed to perform operations. In the operating room, the
operating team is getting dressed in sterile clothing. Also operating in isolated
areas. In the most remote from the entrance of the room is the working area
of the operating nurses. Here is the “big” operating table for sterile
instruments and dressings, tables for fluids and suture material, stands for slut
with sterile linen and material. In this zone during surgery staff not dressed in
sterile clothes are not allowed. In the working area sisters operating team
before surgery wears sterile gowns, gloves, operating room nurse completes a
small tool table.
In the Central zone is the operating table which is set so that access was
provided to the patient from all sides. In the area adjacent to the exit is
anesthetic equipment. On the wall where the door liner is centralized medical
gases (oxygen, nitrous oxide).
Sterilization. In sterilizing cabinets are hot-to sterilize tools. Sterilization
communicates with the transmission via operating the window.
Preoperative. Designed to prepare the operating team for surgery. Here is
washing hands, putting on aprons, goggles. In the preoperative removed after
the operation, sterile clothing, gloves, masks.
Anesthetic. It is designed to prepare anaesthetists for work in the operating
room, the introduction of patient to anesthesia. Operating units of the old
layout anesthetic is not provided, therefore, the introduction of the patient in
anesthesia is carried out directly in the operating room.
Protocol. In the Protocol the doctors write the protocols of surgical
interventions, fill out the required medical documentation.
Sanitary inspection staff. Here operating team passes sanitary processing. The
sanitary inspection there are "dirty" and "clean" areas. In the “dirty” zone a
staff undresses and leaves her clothes in the individual lockers. In the “clean”
zone a staff can only be accessed through the shower. Taking a shower, the
staff wear clean linen, special clothes and shoes. In operating the old layout of
the sanitary systems do not exist. The separation is the function of the
vestibule.
The decoration of the operational unit
The walls and floors of the operating unit must be free of cracks, smooth, have
a water resistant finish to be impervious to dust, insects and rodents. In
operating the joints of the walls, floor and ceiling should be rounded and
covered with materials to make multiple washing and disinfection. The most
often used tiles, but the best material is marble. Best colors are green-blue,
gray-green, as less tiring on the eyes. Their surface should be matte. A
mandatory requirement for all finishing materials, to prevent possible
explosions of gas mixtures is that they are static.
Equipment
In the operating room should not be unnecessary furniture and appliances.
The less furniture, the better to ensure its purity. The furniture should be
lightweight, simple in design, portable, with a good washable surface.
Mode of operation operating
The fundamental principle of the organization of work in operating is strict
adherence to aseptic technique. Adherence starts with the planning of the
operating day. In accordance with the degree of contamination of the
operation determine operational, where it will be operated and the position.
Operations are carried out, observing the order of from less contaminated to
more contaminated.
The mode of operation of the operating unit provides for the restriction of
visits to it. During off hours in the operating room no one should be. In
permitted operating workers operating, operating room teams, anesthesia
teams. To log in to the operating room without the need of prohibited. The
staff before the surgery is performed sanitary inspection, dressing up in special
clothes, different color from the clothes of staff from other branches, wears
Shoe covers or special shoes, hats, masks. Currently, instead of the masks
there are special plastic caps on the face, out of which exhaled air is drawn off
by a special system. Also, patients preparing for surgery, they are washing ,
change clothes, shaving of the hair in the area of operating field, on the head is
worn hat.
The access of unauthorized persons (students, observers) is minimized. To
monitor the operation in modern operating TV is used . During the operation
, movement of personnel should be limited, and mast to limit conversations.
Person 1 hour at rest while breathing emit 10-100 thousands of microbial
bodies, and in conversation - up to 1 million.
In operating it is necessary to maintain a certain microclimate (temperature,
humidity, clean air). Violations of the temperature regime and air exchange
may adversely affect the patient and lead to complications. The optimum
temperature in the operating room is considered to be 22-25C with a humidity
of 50%. Higher temperature causes increased sweating surgeons and the
patient, low temperature can cause cooling of the patient.
An important element of maintaining an appropriate microclimate and
prevention of air infection is proper ventilation of the operating room.
According to the requirements of ventilation must ensure air exchange 3-4
times per hour. To ensure sufficient ventilation operating are equipped with
air conditioning. In the operating room is equipped with supply ventilation, but
not exhaust. During its operation the air takes from the street and pumped
through filters into the room. Along with Academy the dust filters are
removed, fixed on her micro-organisms. Air is exhausted out through the
operating doors, Windows. The use of ventilation avoids the penetration of
contaminated air from adjacent spaces.
However, only ventilation to provide air purification in the operating room is
impossible. Therefore, to disinfect the air used ultraviolet germicidal lamp.
Operating can be equipped with ceiling, wall, floor lamps. Germicidal
lampcreates a "sterile zone" around themselves with a diameter of 2-3 m.
They are placed during the movement of convection currents of air. Be sure to
set the lamp over the entrance, to entering the operating room air was
subjected to germicidal irradiation. Do not place lamp bulb closer than 2 m
from the operating table. Disinfection of air by germicidal lamps is carried out
in between work, during the night or at a designated time. Be sure the lamp
should illuminate during cleaning and for at least one hour after its
completion, as it goes up into the air together with the dust a large number of
microorganisms. Work of germicidal lamps allowed in the presence of
people, only when using aluminum reflective screens. Germicidal lamp for 2
hours sterilizes 30 m3 of air, at the same time to destroy the microorganisms
on the exposed surfaces. The irradiated air for one hour reduces the amount
of micro flora in the air of 75-90%.
When you are running around hot bodies (equipment, fixtures, etc.) arise from
turbulent air streams, which may contribute to the ingress of microorganisms
into the operating area of the wound. Therefore, for the production of a series
of operations (transplantation of organs, implantation of prostheses, etc.) are
operating with ultra clean laminar flow sterile air-conditioned air. In them the
air passing through the bacterial filter is supplied to the operating pressure of
0.2 - 0.3 ATM. through the ceiling and out through holes in the floor. Thus, a
straight-line (laminar) movement of sterile air. A constant vertical flow from
operating kills the microorganisms trapped in the air from the patient or from
medical personnel. The air exchange in such operating up to 500 times in 1
hour.
The content of the operating and care for them.
It is necessary to keep purity and order in the operating room constantly.
For this purpose, the execution of several types of cleaning: preliminary,
current, postoperative, final, general.
Preliminary. In the morning before beginning operations wipe with a damp
cloth horizontal surfaces (floors, tables, window sills to remove the dust which
accumulated in a night from air.
The current cleaning. Produced during operations. During the operation wipes
clean fallen balls tools carried out of the operating room and eliminates
contamination.
The postoperative. Between operations take out waste materials from the
operating room, wipe an operating table with antiseptic solution, change linen.
General. Made under the plan once a week, the day operations are performed.
When performing General cleaning the ceiling, Windows, walls and floors
washed with hot water, soap and antiseptic substances. Is removed from
operating all mobile equipment, its processing is done in another room.
General cleaning is unscheduled in case of strong contamination of the
operating room, for example, after surgery in patients with anaerobic
infections and gas gangrene.
Control of a condition of the operating room is imposed on the elder nurse
sister . She carries out daily overseeing by a state and work of a surgery block,
behind its well-timed cleaning and the exact contents, organizes carrying out
bacteriological researches in the operating room. Control of the mode of
sterility is exercised by carrying out bacteriological researches of air of the
operating room, washouts from walls, a ceiling, devices and devices. Such
researches are carried out once a month.
Adhere to the similar principles at the organization of work of dressing rooms.
All rules accepted for a surgery block extend also to dressing rooms.
PREVENTION OF CONTACT INFECTION
The prevention of contact infection is achieved by compliance with one of the
basic principles of asepsis: “Everything that comes in contact with the wound
must be sterile”. During the operation, the wound into contact:
• the surgeon's hands;
• the surgical field (skin of the patient);
• surgical instruments;
• bandages and surgical linen.
To have been sterile all of the above, the treatment of the surgeon's hands
and surgical field, sterilization of instruments, gloves, surgical linen, dressing
and suture material.
PRINCIPLES AND METHODS OF STERILIZATION
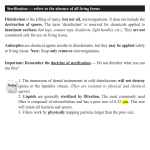
STERILIZATION - a word of Latin origin (sterilis - barren), means the full release
of items from micro-organisms by exposure to physical or chemical factors.
Sterilization is one of the key elements of asepsis. It is achieved through
sterilization of all items in contact with the wound. All methods of sterilization
based on the use of physical or chemical factors. Depending on which items
are processed, shall be elected by one method or another exposure. There are
many sterilization methods, but they must all meet certain requirements. The
methods and means of sterilization should possess the following qualities:
• to have an effective bactericidal action.
• do not cause tissue damage to be safe for patients and medical personal.
• do not destroy the tools and equipment.
Any applicable method of sterilization should, first and foremost to ensure the
destruction of all as pathogenic and not pathogenic microorganisms, it needs
to be harmless to patients and medical workers, not to have a devastating
effect on the tools and devices.
Existing sterilization methods are divided into physical and chemical.
Physical methods: heat treatment - annealing and boiling, sterilization dry heat
sterilization steam under pressure (autoclaving), radiation-induced
sterilization.
Chemical methods: sterilisation by solutions of chemical substances,
sterilization of the gaseous substances.
The choice of sterilization method depends primarily on the type and
properties of sterilizable object.
PHYSICAL METHODS OF STERILIZATION
Thermal methods
Burning. Currently not used, but it can be used, if necessary, sterilization of
metal instruments in the field. Burn tools open flame. Into a metal container
placed tools, pour a small amount of ethyl alcohol and set him on fire.
Boiling. Sterilization by boiling lately is rarely used. This is because in this
method it is impossible to achieve the destruction of spore-bearing
microorganisms, because of the inability to reach temperatures above 100
degrees. Sterilization is performed in an electric steriliser. On a special grid
placed tools in the expanded form (syringes in a disassembled state) and is
dipped in the sterilizer filled with distilled water with addition of sodium
bicarbonate (20 g of sodium bicarbonate in 1 liter of water - 2 % solution). The
sterilization time is 30 minutes after boiling.
Currently thermal sterilisation by either steam autoclave at a temperature of
120-132С or dry heat in hot-sterilising (Cabinet) at a temperature of 170-200C.
When heat sterilization is necessary to allocate the following working phases:
Heating phase – from start of heating until reaching the prescribed
temperature on the thermometer in the chamber;
Time trim – from the moment of reaching the temperature of sterilization in
the working chamber until the moment of clearing her sterilizable material;
While the destruction of germs, the duration of which is prescribed in the
regulations;
Cooling time from the moment of termination of heating to reduce the
temperature up to 80C during sterilization with dry heat and up to 60C during
sterilization in the autoclave.
An sterilization time in usable space consists of time balance, time of
destruction and time extra security, ensuring the reliability of sterilization (50
% of the time).
Sterilization by dry heat. Sterilization is carried out in hot-cupboards-sterilizers,
the applicable factor is the air heated up to 170-200C. If dry heat sterilization
process is heating of sterilizable objects. As the hot air in contrast to water
vapor serves only as a carrier of heat, the temperature of the sterilized objects
needs to reach 170-200C. Heating is provided by hot air proceeds through a
special valve at the bottom of the air sterilizer and its exit through the upper
valve.
By dry heat sterilization process can handle all thermally stable, nonflammable
materials made of glass, metal or porcelain. Hot-sterilization unsuitable for
dressings, rubber, catheters, paper products and plastics.
Sterilization is carried out as follows:
- put the tools on the shelves of the Cabin-sterilizer
- at an open door at a temperature of 80 °C dry up tools within 30 minutes.
-having closed a case door, will sterilize within 1 hour at a temperature of 180
°C.
- after cooling of the autoclave to 50°to 70 ° With the door slightly open, and
the final cooling of the tools taken.
Adding new materials and items for sterilization is unacceptable.
Steam sterilisation. Acting factor in this method is a hot vapor. There are two
methods of sterilization: sterilization by flowing steam and sterilization under
pressure. First method is currently abandoned, so the temperature reached
100C, but not enough to kill certain types of microorganisms. During
sterilization under pressure, the water is heated at elevated pressure,
increases the boiling point of water and accordingly the temperature of the
steam (at a pressure of 2 atmospheres to 132,9°C).
Hot water vapor serves as a carrier of heat. He works harder than hot air,
because the high heat capacity of steam during condensation is transferred to
the sterilizable object. At the same time the steam acts as the immediate
sterilizer is a sterilizing agent acts by hydration operations, coagulation and
hydrolysis of proteins.
The sterilization is performed in autoclaves. Apparatus for sterilization under
pressure (autoclave) consists of two metal cylinders with different diameters,
inserted one into the other so that between them remains a space that's filled
with water. In the inner chamber of the autoclave sterilization put the box
with the filter, the slut with bandages or packages of tools in a two-layer pack
of calico or greaseproof paper. Tightly screw the side door of the steam
sterilizer and begins the sterilization in the specified mode. A steam sterilizer is
equipped with a thermometer, a pressure gauge (indicating the pressure of
steam inside the Cabinet) and the safety valve which is triggered by the
buildup of excess pressure.
All the items that can not withstand high temperature flame sterilization and
for which the temperature of the steam is not damaging, should be sterilized
by autoclaving (dressings, rubber and synthetic items, paper filters, closed vials
and jars with the water-containing preparations, etc.).
Dressings, linen, instruments are placed in a metal box (Bix shimmelbush),
close the lid and leaving open the side holes, slut load in the autoclave.
Sterilization can be in 3 modes - at a pressure of 1.1 atmosphere for 1 hour,
and 1.5 atmosphere for 45 minutes, 2 atmosphere for 30 minutes. Gloves are
sterilized at 1.1 ATM. within 45 minutes or at 1.5 ATM. - 15-20 minutes.
Surgical instruments and syringes at 2 ATM' 20 min.
After the end of sterilization, the time for wiretapping in an autoclave whith
the lid open . Side openings are closed right after extraction of a drum from
the autoclave. on the sterile bix, attach a label indicating the date of
sterilization. Indoor Bix remains sterile for 72 hours. In case of the opening
24 hours.
The main methods of sterilization are now dry heat sterilization, and
sterilization by steam under pressure. In hospitals for the sterilization created
Central sterilization departments (CSSD), where it is performed sterilization of
instruments (syringes, needles, simple surgical sets, probes, catheters, etc.) for
all departments of the hospital. Surgical instruments, sterilized in the
operating units.
Radiation sterilization
For sterilization can be applied ionizing radiation (Gamma rays), ultraviolet
rays, and ultrasound. The most commonly use 1 .
Sterilization by ionizing radiation is used for sterilization of syringes, suture
material, catheters, probes systems for transfusion, etc. Instruments and
materials are sterilized in sealed packages in factory conditions in special
facilities. Shelf life in this method of sterilization is 5 years. The advantage of
this type of sterilization is that its application is not lost properties of
sterilizable (sterill) objects.
CHEMICAL METHODS OF STERILIZATION
Gas sterilization
At current gas sterilization agent is gaseous preservatives (formalin vapors,
ethylene oxide). It is done in special sealed chambers, at the bottom lay
formaldehyde tablets. Instruments placed on a grid above the chemical drug .
Dates sterilization 6-8 hours. The advantage of this method is the minimum
adverse impact on the sterilized objects. Therefore, gas sterilization is used for
sterilizing optical, fine and expensive tools.
Sterilization antiseptic solutions
As antiseptics sterilization solutions used in the ternary solution, 96% ethanol,
6% hydrogen peroxide, chlorhexidine alcohol. This method is used for the
sterilization of cutting tools, so it does not lead to a blunting.
Sterilization is carried out as follows, the tools disclosed or in unassembled
immersed in the solution. Sterilization time is dependent on the type of
antiseptic or alcohol using a ternary solution of 2-3 hours, hydrogen peroxide 6 hours.
TECHNOLOGY OF STERILIZATION
Sterilize is not just to expose the sterilizable object to physical or chemical
factors. Modern sterilization is a process involving several stages.
Stages of sterilization:
Stage I— pre-sterilization preparation
Stage II — laying and preparation for sterilization;
Stage III — sterilization;
Stage IV — storage of sterile material.
Regardless of the form of a sterilizable object, and sterilization method, stages
of implementation it is always preserved.
STERILIZATION OF SURGICAL INSTRUMENTS
Stage 1 - pre-sterilization preparation. The purpose of pre-sterilization
preparation is mechanical cleaning of instruments, removal of pyrogenic
substances, the destruction of the hepatitis b virus. Until recently, the volume
of pre-sterilization preparation was determined by the degree of
contamination of tools, handling tools after clean operations (casts), purulent
surgeries, operations in patients with hepatitis and at risk for AIDS was
significantly different. Now the rules of pre-sterilization preparation tightened.
Given the high risk of the spread of AIDS, the treatment must guarantee the
destruction of the human immunodeficiency virus. Tools of purulent after
operations, patients who have had within last 5 years hepatitis and at risk of
AIDS are processed separately from the others.
Pre-sterilization preparation consists of the following steps:
• disinfection
• washing
• drying
The disinfection
Tools that are used are placed in the tank with disinfectant. As disinfectants
can be applied with 3% solution of chloramine (exposure 40-60 minutes), 6 %
solution of hydrogen peroxide (exposure 90 minutes), anolyte (exposure 30
min). Polides– 1 % - 45’; 0,5 % - 60; combined disinfectant instrumentation – 1
% - 15’; intracept – 1 % - 30’, denavit – 1 % - 20’. After disinfection, the
instruments are washed under running water.
Washing
Wash the tools is carried out in specially prepared detergent solution, which
includes the detergent (washing powder), hydrogen peroxide and water. The
tools are immersed in a solution heated to 50-60°C. After 20 minute exposure
tools thoroughly wash sponge in the same solution and then in running
water.
Drying
After washing, instruments should be dried. Can be dried naturally, but most
often drying is carried out in a hot-cupboard at 80°C for 30 minutes.
After pre-sterilization cleaning is subject to check its quality. It is considered
effective if the products subjected to processing, is not detected residual
quantities of blood, or detergents, the presence of which is determined by
special tests. These samples based on the color change of the reagent in the
presence of the relevant substances (blood, alkaline detergents).
Currently used a Asupernova Proba
Asupernova Proba – azapirone solution mixed with 3 % hydrogen peroxide in
equal parts, drip 2-3 whith the presence of traces of blood, immediately or
not later than 1’ appears first purple, then turning into a pink-purple
coloration, in the presence of rust or chlorine – containing oxidizing agentsbrownish staining.
Instruments the presence of residues of blood are then re-pre-sterilization
cleaning.
The choice of method of sterilization
Fenolftaleina test - conducted to assess the quality of the laundering with the
surface of the instrument detergent.
To prepare: 1% alcohol solution of phenolphthalein.
Steps:
1. Apply 2-3 drops of the solution on the tool at the point of contact with the
wound surface, and compound of the moving parts of the tool.
2. To evaluate the staining. Appearance of pink colouration indicates the
presence of unwashed surfactants. In this case, the entire batch again washed
with tap and then with distilled water. The instrument that carried out the
sample, washed under running water and placed in a container with cleaning
solution to perform a second pre-sterilization processing.
The quality of cleaning of catheters or other hollow products checked by
introducing the reagent inside the product with a syringe or pipette. The
reagent is left inside the product by 0.5-1 min after it is poured on the gauze.
Sterilization method is elected depending on the form of tools. It must be
remembered that any method must, first, to ensure complete destruction of
microorganisms, and secondly, does not lead to rapid destruction of
sterilizable instruments and devices.
Surgical instruments are divided into three groups:
• metal (cutting and no cutting),
• rubber and plastic,
• optical.
For sterilization of metal cutting tools can be used in hot air sterilization hot-in
Cabinet or in an autoclave.
For sterilization of metal cutting tools, the use of chemical sterilization, in
antiseptic solutions, but the best method is gas sterilization. The application of
thermal methods leads to a rapid blunting.
Sterilization of rubber and plastic instruments is autoclaving. Various catheters
and probes are exposed to radiation sterilization, often they are used once.
Sterilization of gloves is also carried out by autoclaving.
Sterilization of optical instruments
Any optical instruments used in surgery differ in complexity and cost. So their
sterilization is carried out most carefully. The best method is gas sterilization.
Sterilization fibrogastroscope, colonoscopes, bronchoscopes may be carried
out by a method of cold sterilization using a chemical antiseptic (ethyl alcohol,
chlorhexidine, "Sidex", etc., 40 % formalin with chlorine bleach at a ratio of 1:
8-their pairs 40').
Stage 2 - installation and preparation for sterilization.
Depending on the selected method, is the preparation and laying of sterilizable
items.
In preparation for sterilization in hot-sterilising, tools are placed in metal boxes
or stack them on a metal grid in a single layer. The syringes dismantled and
wrapped in two layers of heavy paper.
In preparation for sterilization in an autoclave instruments wrapped in cotton
fabric in the form of a package and placed in a metal box.
In the case of sterilization of syringes in an autoclave, dismantle them
separately in gauze wrapped cylinder and piston. They are then wrapped in
cotton cloth and placed in Bix.
Rubber gloves pour talcum powder, filling him inside, wrapped in gauze and
placed in a separate box.
Step 3 - sterilization. Carry out the sterilization method chosen, the standard
observing modes.
Stage 4 - storage of sterile material. Sterile slut stored in a special room.
Sterility is maintained for 48 hours, if the slut has not been opened.
STERILIZATION OF DRESSINGS,
OPERATING CLOTHES
Stage 1 —preparation of the material.
Bandaging material should be easily sterilized and does not lose its properties.
It is made of gauze and wool, and less frequently from viscose and lignin. From
them prepare the balloons, napkins, tampons, turundy, bandages. Gauze
should be folded so that no free edge, which can flake off the fabric. Material
harvested for future use, adding to it as you use it. Before sterilization it is
placed as follows: the balls in gauze bags for 50-100 pieces, napkins tie 10
pieces.
As operating clothes use surgical gowns, sheets, diapers, towels, hats, Shoe
covers. They are made of cotton fabric. Bathrobes, sheets, diapers, towels for
sterilization are formed into rolls, it makes it easy to deploy them when using.
Dressing material after its use is burned. Linen reuse erased, but separately
from other types of underwear.
Step 2 - laying material.
Bandaging material and operational linen are sterilized in the slut. Used three
types of stacking Bix:
• versatile styling
• purposeful styling
• specific styling
Universal - laid material and linen for a small, typical operation. This type of
stacking used in dressing and for small operations. Styling produced by sector.
Bix is divided into sectors, which are filled with a certain kind of material or
linen: in one sector to put a napkin in the other - balls in the third - tampons,
etc.
Targeted - laid material and linen for the specific operation. For example,
appendectomy, gastrectomy. Bix is placed in the set dressings and linen
necessary for the implementation of the operation.
Species - stack a certain type of material or linen.
This type of presentation is used in the operating, running large number of
different operations. Laying out in the following manner – one Bix surgical
gowns, other sheets in the third – wipes, etc.
Laying Bix is as follows.
Checks the condition of the beaks. Wipe the base, wall, lid inside beaks first,
then outside of 0.5% ammonia. On the side of the beaks of the circular plate
(belt tightness), move to open side holes. Beaks lined with double-folded
sheets, with the ends thereof pointing outward. At the bottom of the beaks
put the indicator sterility control. Dressings and linen are placed in the beaks
loose, vertically, across sectors or in layers. Every object is placed so that it was
easy to get without breaking the styling. In the middle of the Bix put another
indicator of sterility control. The edges of the sheets lining the beaks are
wrapped on one another. The top closer to the castle Bix put one control
indicator. Close the lid of the beaks of the castle. To the handle of the bix
attach the tag to the passport.
Step 3 - sterilization. Bandaging material and linen is sterilized by autoclaving
under standard modes.
Stage 4 - storage of sterile material. Side openings bix which sterilised must
be closed. A bix whith sterill material is kept separate from non steril object
After sterilization, store the unopened Bix is possible 3 days after opening 1
day. Unused bix subjected to repeated sterilization.
QUALITY ASSURANCE STERILIZATION
Control of sterility can be carried out which direct and indirect ways. Direct
method - bacteriological, conduct the inoculation with sterile items. It is
produced in the following manner: in the operating room, opened bix , small
pieces of gauze moistened with isotonic sodium chloride solution several times
spend on underwear, and then put in a test tube. Taken this way, the material
is sent for bacteriological examination. Bacteriological monitoring is carried
out once in 10 days. It is the most reliable method of sterility control.
For direct control of sterility of the material used indirect ways. They can be
used to assess the quality of sterilization each Bix. Indirect methods are based
on laying in a sterile bix of thermoindicators if the sterilizable material has a
certain temperature. For indicators use a substance with a particular melting
point with benzoic acid (120°C), urea (132°C), and thiourea (180°C). They are
placed in the vials. Indicators lay with sterilizable items. The melting of the
powder and turning it into a solid mass indicates that the sterilization
temperature was equal to the melting point test substance or exceeded it.
PROCESSING HAND
The aim of surgical hand disinfection is a reliable exemption from the
microorganisms for a long time. Preparation of hands of surgeon and his
assistants for the operation fraught with great difficulties, due to the inability
to use high temperatures and high concentrated solutions of antiseptics. A
special difficulty causes the disinfection of the hands from the germs that
accumulates in the excretory ducts of the sebaceous, sweat glands and hair
bags. In this regard, along with the flushing of the bacteria and destroying
them on the surface of the skin with antiseptics all methods include as a
mandatory component of the tanning of the skin to tighten pores and prevent
the penetration of microbes on its surface during operation.
The principle of surgical hand disinfection is first mechanically cleaned and
then disinfected. Hands and forearms pre-treated in 2-5 minutes with soap
and brush. Particular attention is paid to the treatment of the nail beds and
skin folds, interdigital spaces. Then the hands rinsed and wiped with sterile
wipes. At the final stage use disinfectants. Which should meet the following
requirements:
• quickly kill pathogens.
• safely kill germs in the glove juice hands to remain decontaminated during
the entire operation.
• have a cumulative action to the surgeon's hands remained depleted by
microorganisms and between procedures, disinfection.
• do not render irritating action on the skin.
Treatment of the hands with a solution of hydrogen peroxide and formic acid.
Formulation C-4 prepared on the day of the operation of the required number
of 30-33 % hydrogen peroxide (perhydrol) and 85-100% of formic acid, which
are mixed in a sterile vessel in a ratio of 1:2.4 and store no more than days in a
container with a sealed tube in a cool place. For the treatment of hand use the
2.4 % solution of the formulation “S-4”.
Before treatment of the hands with a solution of the formulation “S-4” wash
them with soap and water (no brush) for 1 minute, wipe dry with sterile towel
and then the hands are usually processed within 1 minute recipe “-4” in the
enameled basin. Wipe with a sterile towel and wear sterile gloves.
Wash hands surgical decontamination is performed first wash with soap,
better liquid. Brushes for modern disinfectants are not required to use. After
washing your hands with soap and water they should be dried with a sterile
napkin and treated with antiseptic. Handling hand hold to the upper third of
the forearm in several stages: the first stage treatment is carried out to the
upper third of the forearm, the second to the middle third, then treatment is
carried out only brushes to prevent contact with the raw surface with
antiseptic hands .
For disinfection of hands today used mainly the following medications: group
detergents - evroseti (sterilium, cutasept F, AHD 2000) and alcohol 0,5-1,0 %
solution of chlorhexidine digluconate; derivatives miramistina - drug Piramides
(0,1 % alcohol solution miramistina).
When using chlorhexidine hands after washing with warm water and soap and
wiped with a cotton or gauze swab moistened with 0,5-1,0 % alcoholic solution
of chlorhexidine for 3 minutes.
When using Euroatom solution in portions of 5.0 ml twice rubbed into the skin
for 5 minutes.
When using muramidase hands treated with the solution for 1 minute.
Rules of processing of hands of modern antiseptics.
PUTTING ON OPERATING CLOTHES
Medical staff (surgeon, assistants, surgical nurses) after surgical disinfection of
hands wearing sterile (free from microorganisms), bathrobe. Operating coats
do not fit loose textile material, repeatedly used, because it becomes
permeable to sweat and bacteria on the skin of members of the operating
team (appear on the robe within 30 minutes of work). It is best to use linen
and bathrobes integrirovannoi of thick cotton material. Cuffs and drawstring
are needs to be flexible and do not squeeze the wrist and hand. The mask
must have a tightly closed the mouth and nose.
After surgical disinfection of hands microorganisms on the skin are absent.
However, soon, from the ducts of sweat glands, hair follicles, microcracks on
the surface of the skin appear again the microorganisms, therefore, with the
goal of aseptic surgery must be isolated hands with sterile rubber gloves.
When putting on gloves not to touch the outside of the bare hand.
While working in her gloved hands are wet, there is accumulated the so-called
glove juice, which contains a concentrate of a virulent microflora, and
therefore before the operation and during it you need to pay close attention
to the integrity of the gloves. A damaged glove should immediately be
changed. If the operation takes a long time , while working every 45-60
minutes gloves treated with 2,4 % pervomur and wipe with 96 % ethyl alcohol.
Handling gloves should also be performed after each phase of the operation
involving the opening of a hollow organ.
PROCESSING OF THE SURGICAL FIELD
Preparing the operation field starts in the preoperative period (hygiene bath,
cleaning impurities with ether or gasoline, skin treatment green or potassium
soap, shaving hair in the area of operational fields). Before the operation the
patient takes a bath, he changed underwear. In the morning, on the day of
surgery, hair in the region of the surgical field carefully shave. Shaving you
should apply the razor without causing irritation. After shaving the skin is
rubbed with alcohol. The hair in the area of the upcoming surgery can also be
removed using a special cream-depilatory. It provides convenience in the
processing of skin folds and reduces the risk of microdamage that was
observed in the processing of razor blade.
The classical method of treatment of the surgical field by the method GrassiaPhilonchikova coating 5% alcoholic solution of iodine is now not applicable. For
skin treatment the operating field is currently most often used yodonat,
yodopiron, 0.5% alcohol solution of chlorhexidine digluconate
The basic rules of treatment of the surgical field:
1. Produce the processing widely.
2. Processing should be done from the centre to the periphery.
3. More contaminated sites process in the least.
4. Processing is performed repeatedly.
First time lubricate the operating field before applying sterile linen, the second –
after the imposition of linen, and the third before sewing the skin and the fourth
time – after sutures on the skin. As shown by numerous studies, iodine tightens
the skin and penetrating the depth of wrinkles and pores, disinfects it.
To handle surgical field using other antiseptic agents (1 % solution germicida 1%
solution of roccal or ketamine A-B, 2.4% of the pervomura). For disinfection of
mucous of their cuticles 1% solution of brilliant green, 3% solution of hydrogen
peroxide, 1% solution yodonat or yodopiron, as well as a 0.5 % alcoholic solution
gibitana. At this point in time, use Betadine, 200 of the ANDES and other
evroseptic.
To isolate the skin of the surgical field, you can use a special sterile film
(protector).
PREVENTION IMPLANTATION NFECTION
Prevention of implant infection is possible by maintaining strict sterility of all
items introduced in the body of the patient.
The feature of the implant way is that in 100% of cases infection leads to the
development of purulent-inflammatory process. Foreign bodies left in the tissues
during this long support the inflammatory process. In some cases, it may be the
encapsulation of infected implants, the micro-organisms die and can cause
outbreaks of a purulent process in the late postoperative period. Formed the
source of a dormant infection.
Sources implant infection.
• suture material
• implants
• metal brackets suturing devices, screws, spokes, screws and plates for
osteosynthesis),
• special devices (cavability, coils, stents, etc.)
• transplanted organs and tissues.
STERILIZATION OF SUTURE MATERIAL
Surgical suture material must be sterile, durable and well tolerated by tissue, and
after performing the locking function to disappear. Currently, there are many
types of suture material. It is divided into the material of natural and artificial
origin. Suture of natural origin: silk, cotton thread and catgut. Artificial suture
material made of synthetic chemicals: nylon, polyester, Perlon, polyester, Dacron,
etc.
Sterilization of suture material is achieved in different ways: thermal, chemical,
gamma irradiation. Typically now use disposable steriline package with suture
material, computed in a single operation.
STERILIZATION STRUCTURES, PROSTHESES,GRAFTS
The method of sterilization of different designs and prostheses depends on the
type of materials from which they are made. Metal structures are sterilized in an
autoclave, hot-closet, or by boiling. Tissue prostheses are sterilized by boiling or in
a gas sterilizer. Dentures complex structures can be sterilized by chemical
methods in gas sterilizer, or chemical preservatives. Currently, most prostheses
available sterilised in the factory by gamma-irradiation. To produce the
sterilization of biological grafts is impossible, therefore, guarantee the prevention
of infection is the observance of rules of asepsis at the fence of organs or tissues.
PREVENTION OF ENDOGENOUS INFECTION
The most dangerous endogenous source of contamination during surgery and the
early postoperative period. Prevention of contamination provides the following
measures:
• examination and rehabilitation of patients before surgery.
• preparing airway for anesthesia and surgery.
• preparation of gastrointestinal tract for surgery.
• delimitation at the opening of hollow organs.
• treatment of the lumen of a hollow organ before and after opening.
Examination of the patient enables the diagnosis of comorbidities, which may
contribute to the weakening of protective forces of an organism (diabetes,
chronic pneumonia, tuberculosis, etc.), and to identify foci of chronic infection
(tonsillitis, caries, periodontitis, suppurative lesions, etc.). The detection of these
pathological processes is directed to rehabilitation or correction of the relevant
disorders of hemostasis.
Preparation of the airway is especially important during inhalation anesthesia and
pulmonary pathology. Patients, especially the elderly, should be trained in
breathing exercises before surgery. On the day of surgery it is important to
reduce the secretion of bronchial glands: enter n/a skin/muscle,/V 0,1% solution
of atropine 0.3 to 1.0 ml. in patients with purulent diseases of the lungs produces
lavage of the bronchial tree with the help of the bronchoscope or trachea by
antiseptic inhalations, bronchoscope or puncture of the trachea.
Preparing the gastrointestinal tract for surgery is done by mechanical cleaning
and the introduction of antibacterial drugs.
For surgery on the stomach mechanical cleaning is required only when the
presence of delayed emptying (pyloric stenosis), or operations on other
abdominal organs if it is performed on an emergency basis under anesthesia
(bowel obstruction, trauma, peritonitis as a result of damage or perforation of the
walls of the stomach and 12 duodenal ulcer). Under normal conditions it is
sufficient to limit food intake in the evening and in the morning stomach is empty.
Preparation of the intestine is carried out through the appointment of laxatives
24 hours before surgery, and the presence of narrowing of the intestine 48 hours.
24 hours is assigned the administration of antibacterial drugs by mouth, which
inhibit the intestinal microflora (chloramphenicol, Biseptol, trihopol). The evening
and morning before surgery made the cleansing and siphon enemas.
Before opening of the hollow abdominal organs is an additional delimitation in
the area of the intended incision body using large napkins soaked in antiseptic
solutions (furacillin 1:5000 chlorhexidine or 1:1000). Possible delimitation with
oil-cloth, polyethylene film.
After further myocardial cooling and opening the treatment with antiseptics
cavity of a hollow organ (internal surface) to be autopsy. Resection of the
stomach, pressed the stump thoroughly washed through a nasogastric tube with
a solution of furatsilina (1:5000), before opening of the intestine (especially the
colon or rectum) clearance in the alleged autopsy, introduced antibiotics,
antiseptics or a combination of them (kanamycin, metronidazole, gentamicin,
dioxidine, chloramphenicol).
After opening of the hollow body lumen it dried gauze (electric pumps), and then
mucosa is processed by a 1% aqueous solution gibitana or Odonata.
After further myocardial cooling and opening the treatment with antiseptics
cavity of a hollow organ (internal surface) to be autopsy. Resection of the
stomach, pressed the stump thoroughly washed through a nasogastric tube with
a solution of furatsilina (1:5000), before opening of the intestine (especially the
colon or rectum) clearance in the alleged autopsy, introduced antibiotics,
antiseptics or a combination of them (kanamycin, metronidazole, gentamicin,
dioxidine, chloramphenicol).
After opening of the hollow body lumen it dried gauze (electric pumps), and then
mucosa is processed by a 1% aqueous solution gibitana or Odonata.
THE PROBLEM OF AIDS AND HEPATITIS VIRUSNYKH IN SURGERY
Twentieth century plague called AIDS (acquired immunodeficiency syndrome). As
in centuries past, plague was brought great disasters to humanity, and AIDS is
currently a real threat to people. Every year a growing number of patients
infected. The spread of AIDS has put before the surgeons a number of serious
problems. The surgeon is connected with the constant contact with blood, other
liquids of the body. Therefore an actual problem of modern asepsis is the
prevention of penetration in the process of treatment in the patient's body and
medical staff of the human immunodeficiency virus.
Prevention of AIDS in surgery includes a range of activities. There are four types of
events:
• identification of virus carriers
• identification of AIDS patients
• compliance with safety regulations for medical staff
• change the rules of sterilization of instruments
The identification of virus carriers.
Should be carried out at the prehospital stage of the planned patients emergency
during inpatient treatment. Patients at risk should be screened for HIV. It should
be remembered that HIV testing Barcelona performed only after written consent
of the patient.
Identification of AIDS patients. Any doctor should know the characteristic
manifestations of the disease, constantly remember them and to be active in
conducting diagnostic activities. For a long time, the doctors zeroed in on the
manifestation of malignancies, i.e., the desire for early and active detection of
malignant tumors. Currently, the same alertness should be developed against
AIDS.
Compliance with safety regulations.
Currently, the developed complex of preventive measures, which must comply
with any medical professional. They can be divided into two groups. The first
involves measures to prevent blood discharge the patient on the mucous
membranes and skin of staff. According to these requirements all manipulations
with blood should be performed in gloves, the doctors and nurses must wear
protective goggles, aprons.
Clearly, measures in case of skin or mucous got any fluid from the patient. In such
cases, the health care provider must carry out the treatment with antiseptics
according to the instructions. Also provides for mandatory measures for the
treatment of the surrounding objects and equipment after contact with blood or
fluid discharge.
Changing the rules of sterilization.
Currently there is a trend towards the use of disposable instrumentation.
Instrumentation reusable now more stringent rules for pre-sterilization
preparation, the treatment must guarantee the destruction of the human
immunodeficiency virus.
Identification of AIDS patients. Any doctor should know the characteristic
manifestations of the disease, constantly remember them and to be active in
conducting diagnostic activities. For a long time, the doctors zeroed in on the
manifestation of malignancies, i.e., the desire for early and active detection of
malignant tumors. Currently, the same alertness should be developed against
AIDS.
Compliance with safety regulations.
Currently, the developed complex of preventive measures, which must comply
with any medical professional. They can be divided into two groups. The first
involves measures to prevent blood discharge the patient on the mucous
membranes and skin of staff. According to these requirements all manipulations
with blood should be performed in gloves, the doctors and nurses must wear
protective goggles, aprons.
Clearly, measures in case of skin or mucous got any fluid from the patient. In such
cases, the health care provider must carry out the treatment with antiseptics
according to the instructions. Also provides for mandatory measures for the
treatment of the surrounding objects and equipment after contact with blood or
fluid discharge.
Changing the rules of sterilization.
Currently there is a trend towards the use of disposable instrumentation.
Instrumentation reusable now more stringent rules for pre-sterilization
preparation, the treatment must guarantee the destruction of the human
immunodeficiency virus.
The risk of infection of various viral infections through contact with infected blood
are not the same. It is believed that the probability of infection With hepatitis C
virus is lower than with hepatitis B. This is because for infection with hepatitis C
need ingested a larger quantity of infected blood. The risk of infection of health
care workers receiving accidental injuries from needles for injections, the
hepatitis C virus is 5 to 10%. One known case of transmission of hepatitis C virus
with drops of blood falling on the conjunctiva. According to the Center for control
and prevention of diseases (CDC) in 1989, the rate of transmission of hepatitis b
virus to health care workers after contact of damaged skin with HBEAg-positive
patient's blood is equal to approximately 30%, and when such contact with HIVinfected blood is 0.3%.
The highest incidence of hepatitis b occurred among emergency physicians and
surgeons. They have two times more often than employees from other
departments, detect HBsAg and antibodies to hepatitis C. the highest risk groups
also include staff of institutions of blood service, the departments of
hemodialysis, renal transplantation and cardiovascular surgery.
Factors that affect the risk of infection of medical staff with HIV-infection:
• the degree of violation of the integrity tissues;
• degree of contamination of the tool;
• stage of HIV infection in the patient;
• patients receiving antiretroviral therapy;
• there is a patient resistant strains of HIV.
Prevention of nosocomial and occupational infection with HIV and hepatitis C
Preventive measures should be aimed at prevention of intra-hospital infection
and occupational infection of medical workers.
In the beginning of the pandemic of HIV infection has come to understand that
the condition of the patients and blood samples facing in operation, the medical
staff, presumably unknown. Is forced to recommend the promotion of the
concept of "mind the blood and fluids of the body" in relation to all patients. The
concept is known as universal precaution (CDC, 1987). Its use eliminates the need
for obligatory identification of patients with infections, blood-borne, and provides
attention to each patient as a potential source of infection. Universal precaution
include hand washing, use of protective barriers when possible contact with
blood, caution when using needles and other sharp instruments all health
facilities. Instruments and other reusable equipment used in invasive procedures
should be appropriately disinfected or sterilized. Further, recommendations were
developed for the prevention of transmission of HIV and viral hepatitis with
professional contacts, including provision of vaccination against hepatitis b,
prevention of infection in dentistry and ambulances, the use of post-exposure
chemoprophylaxis for suspected exposure to HIV and for the prevention of HIV
transmission from healthcare workers to patients during invasive procedures
(CDC, 1990,1991,1993).
Ways to reduce the risk of infection of medical personnel
To reduce the risk of infection of medical personnel in medical institutions is
recommended:
• regularly informing and training health workers in methods of preventing
contact with potentially infected material;
• avoiding to work with patients of any profile, biomaterials and contaminated
items, medical and technical workers with skin lesions (wounds, cracks, weeping
dermatitis);
• ensuring all jobs with disinfectant and a standard first aid kit for emergency
prevention;
• correct sampling and handling of infected material, including various biological
fluids, used instruments and dirty linen;
• use of individual protection means: gloves, glasses, masks, aprons and other
protective clothing;
• vaccination against hepatitis b of all health workers, primarily related to the
group of professional risk;
• regular screening of all personnel for hepatitis viruses and HIV (before and
during);
• strict administrative control over the implementation of prevention programs.
Actions to prevent contamination of medical personnel from viral hepatitis and
HIV:
• to attend classes on the prevention of infections, transmitted by parenteral and
implement the relevant recommendations;
• pre-plan their actions before any work with hazardous tools, including their
neutralization;
• do not use dangerous medical tools, if they can be replaced by safe;
• do not put a cap on a used needle;
• promptly dispose of used needles in special, Neprikasaemye, refuse collection
container;
immediately report all cases of injury when working with needles and other sharp
objects and infected substrates, to get timely medical care and to carry out
prophylaxis of infection;
• to inform about all the factors that increase the risk of injury in the workplace;
• to give preference to devices with protective devices;
• to prepare health workers at all levels: managers, doctors, nurses, social
workers, counsellors and other professionals;
• provide complete and accurate information about transmission and risk factors;
• to teach methods of struggle against discrimination and stigma;
• to observe confidentiality.
Vaccination of workers against hepatitis B. For vaccination using one of the
following two schemes:
• 0, 1, 6 months (the introduction of the second and third doses, respectively,
after 1 and 6 months after first dose);
• 0, 1, 2, and 6 months (the introduction of the second, third, and fourth doses,
respectively, after 1, 2 and 6 months after the first dose).
The second scheme is recommended, if due to a high degree of risk need to
quickly provide protection from possible infection. In such cases, prevention is
based on the ability of vaccines to quickly launch a mechanism of development of
specific immunity and thereby prevent development of the disease if the vaccine
administrated early after infection . When emergency required on the first day
(but not later than 48 hours) to be injected intramuscularly specific
immunoglobulin (HBsIg) containing antibodies to HBsAg (anti-НВ5) in high
concentration, 0.12 ml (not less than 5 ME) per 1 kg of body weight.
Simultaneously administered a first dose of the vaccine. In the future continue
vaccination in the second scheme. Complete course of vaccinations carried out, if
the study of blood taken before the vaccine, discovered the absence of markers
of viral hepatitis in the victim. It is believed that it is advisable to start vaccination
of physicians against hepatitis b before the beginning of their independent work
(in the first year of medical school and colleges). Vaccination protects the health
of the worker and eliminates the possibility of transmission of infection to the
patient.
Currently, for the prevention of viral hepatitis In an officially registered scheme
accelerated immunization vaccine Engerix V. Scheme: 0-7-21 day, it is used in
some hospitals for patients with upcoming planned surgery and other patients
with a planned invasive procedures. The vaccine according to this scheme, 81% of
people vaccinated leads to the formation of anti-NV3 protective concentration,
but after 12 months you need additional vaccine.
The titer of anti-НВ5 equal to 10 Miu/ml, is an indication of formation of
protective immunity, which develops more than 95% of vaccinated individuals
and protects you from contamination not only hepatitis b and Delta hepatitis
(hepatitis D virus requires for its replication, the presence of hepatitis b virus, as it
infects a person only in conjunction with hepatitis B. It may increase the severity
of liver damage).
If the antibody titer less than 10 Miu/ml, the person is left unprotected from
infection and necessary re-vaccination. Some people even re-vaccination is
ineffective. Health workers lack protective levels of anti-НВ5 must comply with
the safety regulations in the workplace.
To prevent infection with the hepatitis C virus needs to adhere to universal
precautions and to prevent skin damage, because while there is no specific
vaccine.
Post-exposure prophylaxis for HIV infection
The main way to protect the health of medical workers in an emergency situation
with risk of HIV infection - prevention measures, including the appointment of
antiretroviral drugs. In the event of an emergency is recommended:
• If skin damage (cut, prick) and the occurrence of bleeding from the damaged
surface does not need to stop for a few seconds. If no bleeding, it is necessary to
squeeze out the blood, the skin to handle 70% alcohol solution, and then 5%
solution of iodine.
• In contact with infected material on the face and other exposed areas of the
body:
thoroughly wash the skin with soap and water, then wipe with a 70% alcohol
solution;
eyes, rinse with water or 0.01% solution of potassium permanganate;
o in contact with the infected material in the oral cavity, rinse your mouth with
70% alcohol solution (not drink!).
• In contact with infected or suspect material on clothing:
this piece of clothing immediately treated with one of solutions of
disinfectants;
to decontaminate gloves;
remove the robe and to soak in one of the solutions;
clothes folded in boxes for sterilization autoclaving;
The skin and the hands and other parts of the body under contaminated
clothing wipe with 70% alcohol solution;
shoes twice, wipe with a cloth dipped in a solution of one disinfectants.
• In contact with infected material on the floor, walls, furniture, equipment and
other surrounding objects:
pour the contaminated area with any disinfectant;
30 minutes to wipe.
Chemoprophylaxis of parenteral transmission of HIV. With the threat of
parenteral infection - damage to the skin tool, the infected HIV, in contact with
the material containing HIV, mucous membranes or damaged skin recommended
antiretroviral prophylaxis. Proven effectiveness of following schemes of
chemoprophylaxis (risk of infection is reduced by 79%): zidovudine - ingestion, 0.2
g 3 times a day for 4 weeks.
Currently use other schemes depending on the availability of health facilities,
anti-retroviral drugs. Efavirenz - 0.6 g per day plus zidovudine - 0.3 g 2 times daily
+ lamivudine 0.15 g 2 times a day. With the development of intolerance to one of
the drugs it is replaced in accordance with the General rules described in the
guidelines for antiretroviral therapy in HIV-infected patients. In addition, you can
use any scheme of highly active antiretroviral therapy, depending on the specific
provision of antiretroviral drugs by medical institutions, with the exception of
schemes with use of nevirapine, as its use increases the risk of side effects that
threaten the lives of people with a normal immune system. A single dose of
nevirapine followed by a transition to a different scheme is valid in the absence of
other drugs.
It is important to start prophylaxis as early as possible, preferably in the first two
hours after a possible infection. If it cannot be started immediately according to
the scheme of high-intensity therapy, how early should begin receiving the
available antiretroviral drugs. 72 hours after possible infection to start
chemoprophylaxis or extend its schema is meaningless.
Recommendations for chemoprophylaxis can be obtained from the specialist of
the AIDS Center at the phone. At night, weekends and holidays, the decision to
start antiretroviral therapy responsible for the hospital doctor.
Design of emergency situations is carried out in accordance with the laws and
regulations adopted by the Federal government and the regions. When you
register the accident in a special register to record the date and time of the
incident, name of health care provider, his position; point manipulation, during
which the accident occurred and the measures taken to protect the health care
worker. Separately indicate name, age, address, patient assistance which the
accident occurred; details make information about HIV infection (HIV status, stage
of the disease, received antiretroviral therapy, HIV RNA (viral load), CD4 count
and СD8-lymphocytes) and the presence of viral hepatitis b and C. If the patient is
the source or HIV status unknown, decide on the beginning of post-exposure
prophylaxis based on the probable risk of infection.
The fact of the injury should be reported immediately to the head of Department
or his Deputy, as well as in the AIDS Center and the Center for state sanitary and
epidemiological supervision. In each health care setting should be the
consideration of injuries to paramedics and registered as an accident in the
workplace.
Surveillance affected employees
A medical worker after the emergency contact with the source of infection should
undergo observation for at least 12 months. Laboratory examination of the HIV
antibody is performed at the detection of the emergency situation, after 3, 6 and
12 months after. The victim should be warned that he needs throughout the
period of observation to observe precautions to prevent possible transmission of
HIV to another person.
ANTISEPSIS- is a complex of the actions directed on destruction of
microorganisms in a wound, pathological focus in the organs and tissues and the
organism as a whole, by using chemicals, mechanical, physical and biological
factors.
THE TYPES OF ANTISEPTICS
Depending on what factors are used to influence the microorganisms, antiseptic
subdivided into types. Distinguish mechanical, physical, chemical and biological
antisepticis. In practice, very rarely limited to the isolated application of only one
type of antiseptic. To fight infection once in the body in most cases use and
chemical, physical, mechanical and biological factors simultaneously or in various
combinations. Therefore, allocate more mixed antiseptics.
MECHANICAL ANTISEPTIC
Mechanical antisepsis is a set of mechanical techniques that are used to fight
infection. These techniques are based on mechanical removal of microorganisms
from wounds. Of course, it is impossible mechanically to destroy the
microorganisms in the wound. The use of mechanical methods can partially
remove the microorganisms trapped in the wound along with the infected
devitalized tissue, blood clots, foreign bodies, exudate, etc., i.e. everything that
can become a breeding ground for further bacterial growth. It should be noted
that the mechanical method in most cases is the main, since the use of other
types of antiseptics is not effective, if it is not deleted infectious focus.
The main methods of mechanical antisepsis
• toilet of the wound
• primary surgical processing of wounds
• secondary debridement
• puncture of cavities.
• the opening of purulent cavities.
• removal or resection of organs.
TOILET OF THE WOUND SURFACE
Toilet of the wound is a mandatory element of surgical treatment for accidental
damages, as well as perfomed at any bandaging.
Toilet of the wound includes the following activities - removal of previously
imposed bandages, treatment of the skin around the wound, removing trapped
on the skin wound exudate, the residues of collodion or cleola, exfoliated
epidermis. Directly from the wound removes exudate, blood clots, loose
necrotizing tissue, foreign bodies.
PRIMARY SURGICAL TREATMENT
Primary surgical treatment (PST) gives an opportunity to convert the infected
wound into aseptic. Execute it in the nearest time after the receipt of trauma,
prior to the development of an infectious process in a wound. The essence of
primary surgical treatment is to prevent the development of the infectious
process removed tissue in contact with the external environment , which
exposed to bacterial contamination. To do this, cut the wound, remove foreign
bodies, blood clots, excised, edges, walls and bottom of the wound along with
areas of necrosis, doubtful - viable and infected tissue is carried out to stop
bleeding and stitch up the wound so that the left cavities. Processing is performed
in the operating room under sterile conditions. Effect of antiseptic primary
surgical treatment consists of removing the pathological substrate, which is a
favorable environment for reproduction of microorganisms; the reduction of
bacterial contamination of tissues to a level at which they do not have a clinically
noticeable damaging effect, activation of factors of local immunity. It is
established that infectious inflammatory process develops, if bacterial
contamination is 105 to 106 microorganisms per 1 g tissue. When properly carried
out surgical treatment of fresh wounds it is possible to reduce the number of
microorganisms in the tissues by 2 - 3 orders of magnitude. Suturing is an
important element in the prevention of development of purulent-inflammatory
process, as it reduces the risk of secondary infections. Currently, primary surgical
treatment is the leading method of prevention of wound infection.
SECONDARY SURGICAL TREATMENT
The secondary surgical treatment is made in case in a wound already developed is
purulent - septic process. At a secondary surgical treatment removed necrotic
fabrics, a purulent exsudate, liquidate the isolated cavities filled with purulent
contents. Excising within healthy fabrics is not made as it on the contrary can
promote distribution of infectious process. Antiseptic action of a secondary
surgical treatment consists is to remove the substratum which is the favorable
environment for their life activity
Puncture of cavities. For removal of inflammatory exudate from the natural body
cavities (pleuritis, arthritis, etc.), as well as from the cavities resulting from the
pathological process (hematoma, abscess) are used they puncture. Currently
undertaking a puncture not only superficial cavities, but also localized in the
depth of the body. In such cases, the manipulation produced under the control of
ultrasound. More often than not limited only to the removal of fluid, but also
injected into the cavity of various antiseptics or provide constant lavage .
The opening of purulent cavities. Unfortunately, in severe purulent-inflammatory
process is not confined to the possible puncture of purulent cavity. Removal of
the pathological substrate (purulent content, necrotic tissue) is necessary to
perform surgical intervention. Most often produce the opening of abscesses. Such
operations are not limited only to skin dissection and removal of purulent
content. Always perform the audit of purulent cavities for the detection of
pockets or streaks, of which hampered the flow of fluid. The creation of an
adequate outflow of the contents of a mandatory element of such interventions.
When purulent-inflammatory diseases of the natural body cavities (pleural
empyema, peritonitis, arthritis), also resorted to opening them.
PHYSICAL ANTISEPSIS
Physical antiseptic is a combination of the methods of infection control based on
the use of physical factors. Methods of physical antisepsis is aimed at creating
unfavorable conditions for vital activity of the microflora, reduction of absorption
of bacterial toxins and products of disintegration of its own tissues. Factor
physical antiseptics are physical phenomena - heat, light, sound waves, all kinds
of radiation, in addition to the physical antiseptics are different therapeutic
methods based on the use of physical laws (hygroscopicity, capillarity, diffusion,
osmosis, etc.)
One of the key elements of infection control is to ensure timely removal of
bacterial toxins and tissue breakdown products from purulent focus. We need to
ensure adequate outflow of fluid. Among the methods of physical antiseptics
used for this purpose, should be highlighted: the use of absorbent dressings,
hypertonic solutions, sorbents, drainage of wounds and cavities.
HYGROSCOPIC OF DRESSING MATERIAL
For treatment of infected wounds has long been used in various dressings.
Bandages are used to protect wounds from the environment and local application
of drugs, at the same time used dressing material itself has a therapeutic effect.
Due to its hygroscopicity of the wound removes blood, fluid, pus, which helps to
eliminate a nutrient medium for microorganisms. As a dressing material use of
cotton, viscose, synthetic fabric, canvas, ribbon, fibrous structures, yarns, other
coatings. Of them made dressings (gauze, cotton wool, bandages, etc.)
The most commonly used cotton-gauze bandage. For superficial wounds gauze or
cotton-gauze tampon applied on the wound surface. If there are deep cavities,
introduce gauze pads or turundy. The duration of the operation of gauze about 8
hours later it loses its hygroscopic properties and impregnated with exudate
begins to prevent the outflow of wound. In order not to produce dressings 3 to 4
times a day swab is introduced loosely. In this case, after the loss of
hygroscopicity, it will not play the role of "plugs", because the outflow will be
carried out by the tampon. For a long time used a tampon of Mikulich. The
wound is placed a large gauze pad with sewn to the middle of the thread, lined
the bottom and sides. The resulting "bag" filled gauze balls. After the balls are
impregnated with a wound, they produce a replacement, while leaving the gauze
in the cavity. Change bulbs produce several times a day. The tampon is removed
after the termination of outflow of fluid, a tissue extract pulling on the thread.
HYPERTONIC SOLUTIONS
To enhance the absorbent properties of gauze and swabs IS moistened with
hypertonic solutions. The most commonly is used 10% solution of NaCI (officinal
hypertonic solution). The osmotic pressure of the hypertonic solution is higher
than in blood plasma. Due to the difference in osmotic pressure the pressure of
the liquid is carried out more actively.
Removal or resection of the body. In some pathological conditions is necessary to
fully remove or resect part of the body affected by infectious process. Such
operations running in the case that came irreversible tissue changes. When
performing such interventions the aim is to remove the purulent focus, which
contributes to a more extensive dissemination of the infectious process.
It should be noted that methods of mechanical antisepsis are essential in the
treatment of surgical infections. The use of any other factors (physical, chemical,
biological) will be ineffective if not eliminated by mechanical means the source
(focus) of infection.
DRAINAGE
An effective method of combating wound infection is drainage of wounds and
cavities. Drains provide the outflow of fluid from the interior of natural or
pathological cavities in the environment, reducing the absorption of bacterial
toxins, products of tissue destruction. Currently, several types of DRAINAGES.
They are all based on the use of various physical factors (capillarity, surface
tension, pressure difference, etc.).
There are three types of drainage:
1. passive of drainage
2. active of drainage
3. fluidly - washing drainage
Passive of drainage
In passive drainage as a drainage used rubber strips, silicone and PVC pipes. The
drainage is conducted is down to the lowest point of the cavity and through the
wound separate or cut output. If you use a tube, and on the side surfaces make a
few holes. The outer end of the leave the bandage (rubber strips) or dipped into
the vial with an antiseptic, you can use special sealed plastic bags. The receiving
container should be placed below the level of the body. Drainages, introduced
into the cavity should fix the skin seams, this measure allows to avoid migration of
drainage as the outside and inside. For the effective functioning of drainages is
necessary to monitor them. The lumen of the tube can be overlapped necrotic
tissues, respectively, stop the outflow of exudate.
If necessary, drainage of the chest cavity, apply drainage for Belau,.. It should be
attributed to passive drainage , so for work not included forces of body. A
drainage tube is introduced into the pleural cavity, at the outer end it is fixed with
flap valve of rubber fingertip, which is immersed in an antiseptic solution. When
breathing movements change the pressure in the thoracic cavity. When exhaling,
the pressure increases, the fluid in the tube flows into the bottle (valve open)
during inspiration the valve closes, preventing the flow of solution.
Active drainage
Active drainage involves the application of an external force, providing the
outflow of wound. The functioning of the drainages of this type is based on
creating a pressure difference in the wound and on the outside. Currently, many
models of active drainages, but the principle is the same. On the outer end of the
drainage creates negative pressure, through the suction effect of the wound
exudate is removed. Active drainage is applied if the drains sealed cavity (sewn
wound abscess cavity, thoracic cavity, the cavity of joints). Not this kind of
drainage to use in interventions on the abdominal cavity, as the omentum or
intestines may be prisoin to the holes of the drainage tube. In the best case it will
cease to function but may develop necrosis of the bowel wall.
Active drainage involves the application of an external force, providing the
outflow of wound. The functioning of the drainages of this type is based on
creating a pressure difference in the wound and on the outside. Currently, many
models of active drainages, but the principle is the same. On the outer end of the
drainage creates negative pressure, through the suction effect of the wound
exudate is removed. Active drainage is applied if the drains sealed cavity (sewn
wound abscess cavity, thoracic cavity, the cavity of joints). Not this kind of
drainage to use in interventions on the abdominal cavity, as the omentum or
intestines may be prisoin to the holes of the drainage tube. In the best case it will
cease to function but may develop necrosis of the bowel wall.
Drainage is as follows. In drained cavity introduce one or two of silicone and PVC
tubing with holes on the walls. Their conduct should not through the wound but
through a separate small incision. If necessary, for better sealing, you can put a
few skin sutures. The outer end of the drainage attached to the tank, which
creates a negative pressure. For this purpose, use a plastic harmonica, a special
plastic cans or various types of suction, water jet, electric).
The most simple vacuum drainage is by Redon. The method consists in the
following. Heated to 100°C in the water bottle closed hermetically with a rubber
stopper. On cooling the vessel gradually creates vacuum up to 75 - 100 mm of
mercury. article the Connection of such system to the drainage provides for the
removal of her to 180 ml of fluid.
A highly original system for vacuum drainage with pleural empyema has been
proposed M. S. Subbotin. A vacuum on the end of the tube introduced into the
pleural cavity, is created by movement of the fluid in the two banks according to
the law of communicating vessels. The liquid from the upper banks along the tube
flows into one of the lower, while in the upper Bank (closed tightly) the pressure
is reduced. The pressure reduction in the upper Bank leads to the suction of air
from the second lower banks, which is hermetically connected with a tube
inserted in the pleural cavity.
In the absence of special devices, you can use a simple sealed vial. The vacuum it
creates by suction of air using a syringe Janet.
This type of drainage is also called the closed or vacuum. To apply it is only
possible when sealing the cavity. It is believed that the active drainage is the most
effective method. In addition to removing the content it contributes to the rapid
reduction of the wound cavity.
Flow-drainage.
In the treatment of purulent wounds and inflammatory diseases of the cavities
arises the need to remove from the wound not only the exudate, but the decay
products of tissues. Passive and vacuum tubes for this purpose can be ineffective,
as it cannot support the removal of thick pus, necrotic tissue. In such instances, a
flow-washing drainage. Drainage is as follows. Into the wound or cavity enter the
drainage tube as well as during passive or active drainage. Additionally, usually on
the opposite side from the outlet of the drain tube, introducing the tube of
smaller diameter. Using it constantly is the introduction (or drip struino)
antiseptic solutions that flow through the drain tube. Antiseptic constantly
washes the cavity, while it is removed from the fluid, disintegrated,
nekrotizirovannye tissue. You need to follow to avoid the delay of the solution. To
take account of the amount and the flowing liquid. It should not be different. You
can use two translucent tubes, a thin channel which is used for introduction of
the antiseptic, broad – removal of fluid from the cavity. Method a flow-wash
drainage is very effective. When it is used in some cases sewn up tightly even
infected wounds. Flow-drainage. can be used for drainage of the abdominal cavity
(peritoneal dialysis). In addition of antiseptics to the wound can be administered
proteolytic enzymes that contribute to the melting of devitalized tissue
(enzymatic dialysis). A flow-wash drainage may be applied simultaneously with
the vacuum aspiration. This type of drainage should rather be attributed to the
methods of the mixed antiseptics, because in addition to the physical factors used
chemical and biological.
The choice of drainage method depends on a number of factors, but the
preference should be given not passive. Active and flowing-. drainage allows to
quickly arrest the inflammatory process.
Sorbents
In recent years increasingly used sorption method for the treatment of wounds,
providing for the introduction into the wound of substances adsorbing on itself
toxins and microorganisms. This is usually carbonaceous matter in the form of
powder or fibers. The most commonly used polifepan and various coals intended
for hemosorption and hemodialysis, such as a SMOOTH 1.
The development and use of sorbents is one of the most important medical
advances of the second half of the twentieth century. At the beginning of the
widespread hemosorption, enterosorption and then finally, most recently, the
application or wound sorption, although historically initially sorbents have been
used to treat wounds and poisonings.
When wound sorption in the wound introduce a substance capable of adsorbing
toxins and the microflora. As the application of sorbents used coal, activated in
the form of granules or fibrous materials, polifepan, algipore, eleven, helical,
debrisan, genetical, liposorb, tigerr, cellosorb etc.
Included in dressings or directly introduced into the wound sorbents have a
therapeutic effect in all phases of wound healing.
Bacteriological investigations showed that the introduction of sorbents into the
wound leads to a reduction in the number of microbes by several orders of
magnitude.
The efficiency of the sorbents will be reliable when they are used antiseptics or
when the sorbent will change as the loss of its sorption properties.
Physical factors
Drying. The treatment of wounds can be probuditi without the use of bandages.
This method is used for extensive wounds, burns. Patients are placed in a special
chamber where it is maintained at low humidity and elevated temperature.
Wound surface gradually dries and forms a scab, which is a biological bandage,
creating unfavorable conditions for microorganisms. Even better, when applied
method of treatment in abacterial environment. The patient or the limb placed in
a special chamber, which create abacterial environment using special installation.
Washing.
In addition to a flow-wash drainage for the treatment of wounds used pulsating
jet lavage. Pulsating stream of fluid is formed using special apparatus that creates
alternating phases of high and normal pressure. In the phase “pressure” water-jet
due to turbulent movement washes all parts of the wound and captures the flow
of a liquid tissue detritus. Germs, blood clots, small foreign particles that are left
in the wound after surgical treatment. In the “decompression” phase of the fluid
flow carries away all the contents into the tank. The treatment of the wound
pulsating jet was carried out as before surgery, and during it, but the biggest
effect it gives after surgical treatment.
As a result of processing of the wound pulsating jet, the number of microbes in
the wound is reduced by 1 - 2 orders of magnitude, and the combination of
surgical treatment and pulsed jets by 3 - 5 orders of magnitude compared to the
original quantity.
Treatment of vaccum.
The vacuum created by vacuum suction. In the wound serves an antiseptic
solution or antibiotic and nozzle of the vacuum device sucked into the sump from
the side , pockets of tissue detritus, debris, blood clots, microorganisms. The
procedure lasts 5 - 10 minutes prior to the appearance of diffuse capillary
bleeding.
The low ultrasound frequency has a bactericidal action. In liquid medium the
ultrasonic waves cause cavitation pronounced effect - will have shock waves in
the form of short pulses with the formation of cavitation bubbles. Fluctuations of
the solution contribute to the improvement of microcirculation in tissues, and
rejection of necrotic tissue. In addition, under the action of ultrasound ionization
of water with the release of her molecules ions H+ and Oh-, which cause the
violation of redox processes in the microbial cells. Treatment of wounds with
ultrasound is called ultrasonic cavitation of wounds.
Ultrasonic treatment is performed as follows. The cavity of the wound is filled
with solutions of antiseptics (antibiotics). Then the solution exposed for 3 to 10
minutes of low-frequency or medium-frequency ultrasound. In the result of
combined surgical, antimicrobial and ultrasonic treatment is rapid and complete
wound cleansing from necrotic tissues, accelerates reparative processes.
Laser.
For the treatment of purulent wounds used radiation of low power. It has a
bactericidal effect, without the damaging effect on the fabric. Used with this
purpose, lasers with low-intensity radiation, in particular, a helium-neon laser
which emits monochromatic polarized light with a penetration depth into the skin
to 0.61 mm in the muscle - to 2.04 mm. the Laser can be applied in the form of a
“laser scalpel”. In this case, use a carbon dioxide laser with high power focused
beam. Debridement of suppurative focus or bloodless. The laser beam has a
volatile effect on nekrotizirovannye tissue and microorganisms, which leads to a
rapid and complete removal of damaged tissues. On the walls of the wound forms
a thin coagulation film that prevents the penetration of microorganisms and their
toxins in the tissue. In addition, the CO2 laser beam has a direct bactericidal
action. So the wound is almost completely released from microorganisms.
Laser radiation is used for irradiation of blood as ekstrakorporalna and inside
vessels. But these methods should be attributed to the biological antiseptic, as is
used in this case is not bactericidal activity, and the ability of stimulation of
protective forces of an organism.
Radiotherapy.
X-rays has anti-inflammatory actions. To radiation therapy is resorted to if
necessary to suppress the infection in a small, deeply located lesions.
Cryosurgery.
Low-temperature effects on the wound leads to a decrease in the number of
microbes to a level below the critical, reduces acidosis wound content, increases
the phagocytic activity of leukocytes. As a result, accelerates the cleansing of
wounds and regeneration, reduces the treatment time.
Ultraviolet irradiation (UVI).
Ultraviolet radiation has bactericidal, anti-inflammatory and desensitizing effect.
To prevent the spread of the infection and resorption of inflammatory infiltration
used ultraviolet irradiation in erythema doses.
Electric field of ultrahigh frequency (APUWJ). It causes dilation of blood vessels,
accelerate blood circulation, enhancing immunological processes, especially the
phagocytic activity of leukocytes.
Medicinal electrophoresis. During electrophoresis the pH change that activates
the activity of the enzymes, its action creates a persistent depot of drug ions.
CHEMICAL ANTISEPTIC
Chemical antiseptics is a set of methods of combating infection in a wound,
pathological focus or the body of the patient based on the use of various
chemicals. This type of preservatives widely used in the treatment of surgical
diseases. Currently offered a huge number of drugs with bactericidal and
bacteriostatic activity.
THE MECHANISM OF ACTION OF ANTISEPTICS
The activity of microorganisms is possible under optimal conditions, the change of
such constants as temperature, osmotic pressure, ionic balance, etc. creates a
hostile environment for the development of infection. The effect of antiseptics is
based on the change of these constants. When they act violated the metabolic
processes in the microbial cell that leads to slowing down the reproduction of
microorganisms. In these cases, talking about the bacteriostatic action of an
antiseptic.
The antiseptic substance may penetrate into the protoplasm of the microbial cells
and lead to the coagulation of proteins and of her death. It is a bactericidal effect.
The best are antiseptics that destroy microbial cell.
It should be remembered that in addition to the effects on the microflora, these
chemicals in most cases possess the biological tissue in the application area (in
the wound) and the body as a whole (when suction from a wound or in their
General application). Therefore, not all chemicals can be applied in medical
practice.
Chemical antiseptics must meet the following requirements:
1. in low concentrations, to kill or retard the growth of pathogenic
microorganisms;
2. no adverse effects on tissues;
3. not have General toxic action;
4. should not inaktivirovanie exudate or other body fluids.
5. be persistent during long-term storage;
6. have a dosage form suitable for its application;
7. to have a simple manufacture and low cost.
CLASSIFICATION OF ANTISEPTICS
Chemical ANTISEPTICS are divided into groups according to several
characteristics.
On the purpose and method of application are divided into:
• disinfectants
• antiseptic substances outdoor use
• chemotherapeutic agents.
Disinfectants are used for instrument processing, washing walls, floors, treatment
and care items . etc.
Antiseptic substances for external use are used for skin treatment, hand surgeon,
surgical field, washing wounds, mucous membranes, the local treatment of
wounds.
Chemotherapeutic agents are injected into and provide resorptive effect in the
patient by reducing the infection in various pathological lesions.
On chemical structure.
Produce 17 groups of chemical antiseptics:
1. The group of Halogens
2. Salts of heavy metals
3. Alcohols:
• aldehydes
• phenols
• dyes
• acid
4. Alkali
5. Oxidants
6. Detergents (surface active agent)
7. Nitrofuran derivatives of
8. Derivatives of 8 - hydroxyquinoline
9. Derivatives chinoxalin
10. Derivatives of nitroimidazole
11. The tars, resins
12. Antiseptic of plant origin
13. The sulfonamides.
THE MAJOR GROUPS OF CHEMICAL ANTISEPTICS
1. The group of Halogens.
Chloramine B - 1 - 3 % aqueous solution. Used for disinfection of objects of care,
rubber tools, premises. Used for disinfecting hands, 0.5% solution for disinfection
of premises 2 %.
Iodine - 1 - 5 - 10 % alcohol tincture. Is used for external application (for
processing the skin around the wound ligation, for the treatment of abrasions,
scratches, superficial wounds). Has a pronounced tanning effect.
Iodinol - 1% solution, "blue iodine". Used for throat gargling, washing wounds,
purulent cavities, trophic ulcers. .
Yodonat - 1% solution. Used for the treatment of the surgical field.
Yodopiron - 1% solution. Used for skin disinfection of the surgical field and at the
primary surgical treatment of wounds.
Lugol's iodine - aqueous and alcohol solution of iodine and potassium iodide. The
preparation of combined action. Used for the sterilization of catgut as a
disinfectant. As a chemotherapeutic tool is used in the treatment of thyroid
diseases.
Povidone-iodin - organic iodine compound (0,1 - 1 % of free iodine). Used for
treatment of the skin with dressings and operations, as well as the treatment of
wounds (aerosol).
2. Salts of heavy metals.
Corrosive sublimate (mercury dichloride) is a strong poison. Solution 1:1000 or
1:2000 can be used for disinfection of gloves, care items, sterilization of silk. Has
toxicity, so currently the application is limited.
Oxycyanide mercury disinfectant. Used for sterilization of optical instruments in
the form of a solution in a concentration of 1: 10000,1: 50000.
Silver nitrate (lapis) - an antiseptic external use, has anti-inflammatory action. 5 20 % solutions have a pronounced cauterizing effect. Used in the treatment of
erosions, ulcers, cracks, excessive granulation tissue. For washing of the
conjunctiva, mucous membranes, bladder, purulent wounds and cavities are used
of 0.1—0.2 % solution. 1 - 2 % solution 1-2 % ointment is used to ablate excess
granulation in the treatment of fistula.
Protargol, collargol - salts of silver. Antiseptic external application. Have
astringent effect. Apply 1 - 3 % solutions for disinfection of the bladder, the upper
respiratory tract and eye drops for conjunctivitis, blepharitis.
Zinc oxide - an antiseptic for external use. Has anti-inflammatory effect, prevents
the development of maceration. Part of many powders and pastes.
3. Alcohols.
Ethyl alcohol - is used in 70 - 95% water solution as a disinfectant (processing
instruments, sterilization of suture material) and as an antiseptic external
application (processing hands of the surgeon and the surgical field, the edges of
the wound with dressings, compresses, etc.). 70% alcohol has an antiseptic effect,
96 % - and even tanning. Currently widely used combination medications
containing ethyl alcohol - a AHD - 2000 (active agents ethanol and ether polyalloy
fatty acids), and AHD - 2000 special (includes chlorhexidine).
4. Aldehydes.
Formalin - 37 % solution of formaldehyde. Has a strong disinfectant action. 0,5 5% solution used to disinfect gloves, drains, tools. In dry form is used in
pereformuliruem chambers for sterilization of optical instruments, artificial
prostheses, etc. Good quality material for pathological research.
The Lysol is a strong disinfectant. 2% solution can be used for disinfection of
premises, care items, tools. Currently almost never used.
5. Phenols.
Carbolic acid - a potent disinfectant. Before for disinfection of gloves, care items
was used 2 - 3% solution. Currently, carbolic acid is used in combination with
other substances.
Triple the solution is a combination drug that includes preservatives from the
group of aldehydes and phenols. Contains 20 g of formalin, 10 g of carbolic acid,
30 g of soda dissolved in water (liter). Can be applied to treatment tools, care
items, sterilization of cutting tools.
6. Dyes.
Organic compounds, dyeing fabric and is bactericidal.
Diamond green - 1 - 2% alcohol (or aqueous) solution Antiseptic for use external .
Used for treatment of superficial wounds, abrasions, oral mucosa, skin, treatment
of pustular skin diseases.
Methylene blue - 1 - 2% alcohol (or aqueous) solution. Antiseptic for use external.
Used for the treatment of superficial wounds, burns, abrasions, oral mucosa, skin.
A 0.02% aqueous solution may be used for washing purulent wounds and cavities,
the bladder.
Ethacridine lactate (rivanol) is a yellow crystalline powder. Used in the form of
freshly prepared 0,05 - 0,2 % aqueous solutions. Used for washing to fresh and
infected wounds, purulent cavities.
7. Acid.
Boric acid powder, 2 - 4 % aqueous solution. Antiseptic for external use. Used in
the form of powders, solution, rinsing and treatment of purulent wounds, chronic
fistulas. Particularly effective against Pseudomonas aeruginosa. 5 - 10 % ointment
is used for pustular diseases
Salicylic acid – an antiseptic for external use. It has antibacterial and keratolytic
effect (lysis of necrotic tissue). Used in the form of powders ointments, 1% and
2% alcohol solutions for the treatment of wounds containing necrotic tissue.
Included in the paste of lassara (2 % salicylic - zinc pasta)
Nagarajuna acid disinfectant. Used for processing of surgeon's hands, surgical
instruments, rubber gloves.
8. Alkali.
Ammonia – antiseptic for external use. 0.5% solution was used for processing of
surgeon's hands at the method of Spasokukotskogo - Kochergina.
9. The oxidizing agents.
This group includes potassium permanganate, hydrogen peroxide and products
containing it. Oxidants in contact with the tissues, enter into compounds with
organic substances it releases atomic oxygen having a strong oxidizing action. This
creates unfavorable conditions for microbial growth. Especially effective oxidizing
agents under anaerobic and putrefactive infections.
Permangant potassium is an antiseptic for external use, has a coagulating and
deodorant effects. Used aqueous solutions. For washing of wounds and cavities of
0.02 - 0.1% solution; 0.01% in rinse of the mouth and throat, gastric lavage, 2 - 5
% solution for the treatment of burns and bedsores.
Hydrogen peroxide - antiseptic for external use. Used in the form of solutions. Has
antiseptic, haemostatic (helps stop bleeding), deodorizing properties. When
injected into the wound with H2O2 decomposes to release O2,it forms abundant
foam. Antiseptic action of H2O2 is due to both a strong oxidizing effect and
mechanical cleaning of the wound from pus and foreign bodies Produced
abundant foam helps to remove from the wound of pus, fibrin, necrotic tissue.
For washing of purulent wounds, infected cavities, fistulas used 3% solution. 3 - 6
% solution of hydrogen peroxide in combination with 0.5% solution of detergents
used for disinfection of operating and surgical departments, surgical instruments.
Perhydrol - contains about 30 % hydrogen peroxide, used for the preparation of
pervomura used for the treatment of hands.
Gidroperit— complex compound of hydrogen peroxide and urea. Available in
tablets weighing 1.5 g. Used for washing wounds as a 1 % solution. To prepare the
solution dissolve two tablets in 100 ml of water.
10. Detergents.
It is a potent surface - active compounds belonging to the group of Quaternary
ammonium bases.
Chlorhexidine digluconate and 20% aqueous solution. Antiseptic for external use.
For washing wounds using a solution of 1:400,for irrigation of body cavities with
purulent inflammation of 1:1000. Prepare solutions as follows - 1 ml of a 20%
solution of chlorhexidine digluconate, respectively, diluted in 400 and 1000 ml of
distilled water. Sterilize the solutions by autoclaving at a temperature of 115S for
30 min, 0.5% alcohol solution is used for the treatment of hand surgery and
surgical field. Chlorhexidine digluconate is part of the solutions for the treatment
of hands and operating field ("Plivasept", AHD - special).
Carigali - antiseptic for external use. Used for the treatment of hands. When
applied to the skin, polyvinyl butyral, part of zeregelja, forms a protective film
which is removed with ethanol.
Degen, degmesin - antiseptic for external use. Used for the treatment of hands
and operating field.
Rokkal 10% and 1 % aqueous solution. Low-toxic antiseptic with deodorizing
effect. It has a bactericidal action. Used for treatment of hands, operating margins
(0.01% solution) disinfection of objects of care (1 % solution), treat wounds
(0,0025 % solution)
11. Nitrofuran derivatives of.
Nitrofurazone drugs are derivatives of 5 - nitrofuran. They are similar in their
action to broad-spectrum antibiotics, but in some cases are very active.
Nitrofuran derivatives of possess broad spectrum of activity, effective against
most gram-positive and gram-negative bacteria, spirochaetes, protozoa and large
viruses. Have low toxicity.
Furatsilin - antiseptic for external use. Aqueous solution 1: 5000. Used for the
treatment of purulent wounds, burns, pressure ulcers, irrigation of cavities and
mucous membranes.
Furagin is a chemotherapeutic agent. Apply with heavy purulent-septic diseases
caused by staphylococci, streptococci, E. coli and other sensitive to the drug
pathogens. Enter intravenous drip method in a daily dose for adults is 300 - 500
ml of 0.1 % solution (0.3 - 0.5 g of the drug), or every 1 - 2 for only on course 3 to
7 infusions.
Furadonin, furazolidone is a chemotherapeutic agent effective against urinary
tract infection ("uroantiseptiki"). Can be used in the treatment of intestinal
infections.
Lifuzol – antiseptic for external use, containing furatsilin, linetol, tar, acetone.
Available in aerosol form. It is used to treat superficial wounds, burns. When
applied on the wound forms a protective surface with antimicrobial action film,
which is held for 5-7 days.
12. Derivatives of 8 – hydroxyquinoline.
The nitroxoline (5 - NOK) - antiseptic chemotherapeutic agent used for the
treatment of infectious diseases of the urinary tract ("uroantiseptik”).
Enteroseptol, intestate - antiseptic chemotherapeutic agent used in the
treatment of intestinal infections.
13. Derivatives chinoxalin.
Hinoksidin – chemotherapy antiseptic. Has broad spectrum antibacterial action.
Effective against Escherichia coli, Pseudomonas aeruginosa, Proteus vulgaris, the
causative agents of gas gangrene. Administered orally at 0.25 g 3 times a day.
Dioxidine - antibacterial broad-spectrum drugs. 0,1— 1 % aqueous solution
applied for treatment of purulent wounds, irrigation of the bladder, cavities,
purulent fistula, the mucous membranes, especially the ineffectiveness of
antibiotics and other antiseptics. In severe infections may be administered
parenterally. Intravenously administered up to 60-90 ml (2-3 reception (30 ml of
solution is diluted in 500 ml of 5 % rastvorilis). Contraindicated in violation of
renal excretory function.
14. Derivatives of 5 – nitroimidazole.
Metronidazol (metrogel, glaygl, klion, trihopol) – antiseptic chemotherapeutic
agent broad-spectrum, effective against protozoa, Bacteroides and non-clostridial
anaerobic bacteria. It is used to treat amebiasis, leishmaniasis, trichomoniasis,
peritonitis, purulent diseases of the pleura, osteomyelitis, severe anaerobic
abscesses. Assign drug inside of 0.25 g 2 - 3 times a day for 7 - 10 days and
intravenous (metrogyl for injection). When intravenous use is administered to
adults and children over 12 years: 0.5 g in 100 ml solution at 5 ml per 1 minute.
Can be applied rectally in the form suppositories 0,5 g 2-3 times a day.
Tinidazole (fasigyn) - Indications and spectrum of action are the same as
metronidazole. Available in tablets of 0.5 g administered orally.
15. The tars, resins.
Birch tar is an antiseptic for external use, is a member of Vishnevsky ointment.
The ihtiola, Naftalan - has anti-inflammatory properties. Used in the form of
ointments.
16. Antiseptic of plant origin.
Volatile, chlorophyllin, Valerian root, baliz, calendula - antiseptic for external use.
Have antibacterial activity and anti-inflammatory effect, stimulates reparative
processes in wounds, promote sloughing. Used to lavage of superficial wounds,
mucous membranes, skin treatment.
17. Sulfonamide.
Sulfa drugs are chemotherapeutic antimicrobials. They have a bacteriostatic
effect. sulfanilamides susceptible by streptococcus , gonococci, meningococci,
and others. They are used to suppress a variety of foci of infection in the body.
The mechanism of action is based on infringement of synthesis necessary for their
folic acid and dihydrofolate activity. In surgical practice often used short-acting
sulfonamides (streptocid, etazol, sulfadimezin et al.), At least - long and extremely
long action (sulfapiridazin, sulfadimetoksin). Tableting applied as drugs may be
formulated as ointments, dusting powders.
Short-acting sulfonamides.
Streptocide - one of the main drugs of sulfonamides. It is used to treat angina,
erysipelas, cystitis pielita for the prevention and treatment of wound infections
and other infectious diseases. It affects streptococci, meningococci, gonococci,
pneumococci, E. coli and some other bacteria. Assign inside tablets 4 - 6 g daily,
topically applied powder, ointment, liniment and streptotsida.
Etazol, sulfadimezin, sulfatsil - sodium, urosulfan. Unlike streptotsida cause fewer
side effects. Most often used in the form of tablets. The therapeutic dose of 0.5-1
g preparations 4-6 times a day inside. Etazol - Sodium and can be administered
intravenously in a 10% and 20% solutions of 5-10 ml. For wound treatment
preparations are used in powder form (powder).
Sulfonamide long and extremely long action.
These include - sulfapiridazin sulfadimetoksin, sulfalen, Biseptol (Bactrim). Is
administered orally in tablets of 0.5 g, the daily dose of 1 - 4 g
Due to the poor solubility of sulfonamides can precipitate as crystals (crystalluria)
and clog the glomeruli. To prevent these complications, patients when taking
sulfa drugs should receive plenty of alkaline water.
BASIC METHODS OF antiseptics
when applying a chemical antiseptic, it should be remembered that it, like any
therapeutic measures should be carried out according to strict rules. Mode of
application largely determined by the shape of its production, or mechanism of
action.
Topical administration of chemotherapeutic agents:
1. antiseptics may be used as dressings in the treatment of wounds and burns. In
such cases, solutions are used, which are washed during wound dressings, and
swabs moistened wipes. Application in the form of ointments and powders.
2. antiseptics can be administered as solutions in a closed cavity through
aspiration followed by drainage - washing, flow drainage.
General use of chemotherapeutic agents.
1. Enteral application. Antibiotics taken orally in pill form.
2. Parenteral administration. The most frequently used intravenous
antimicrobials.
Biological antiseptics
Biological antiseptic - a set of methods for combating infection in the wound, the
pathological focus or the patient's body based on the use of various biological
factors.
Unlike other kinds of antiseptics, biological antiseptic - it is not just the biological
methods for destruction of microorganisms. Biological antiseptic is divided into
two types:
• Biological antiseptic direct action. Applied biological factors directly affecting
the microorganisms.
• Biological mediated antiseptic action. Applied biological factors affecting the
patient's body to stimulate its ability to destroy microorganisms.
Thus, the biological antiseptic involves the use of biological origin, which influence
both on the microorganisms and the macroorganism. The impact on the macroorganism is enhanced immunity and increased protective properties. On the
microorganisms is an overwhelming effect.
MAJOR DRUGS AND METHODS OF BIOLOGICAL
ANTISEPTICS
Methods of direct action on microorganisms
- Antibiotics.
- The use of proteolytic enzymes.
- Carrying out specific passive immunization (therapeutic serum antitoxin, Yglobulin, bacteriophages, hyperimmune plasma)
Methods of indirect actions on microorganisms
- Methods of stimulating non-specific resistance (UVR blood kvartsevanie, laser
irradiation of blood, use of perfusate and ksenoselezenki cells, transfusion of
blood and blood components)
- Introduction of substances that stimulate innate immunity (vitamins, thymus
preparations (timalin, T - activin), prodigiozan, lysozyme, levamisole, interferons,
interleukins)
- The introduction of products for active stimulation of specific immunity
(vaccines, toxoids)
Antibiotics
Antibiotics are the most important group of biological antiseptic agents used for
the treatment and prevention of surgical infection. These are substances that are
formed during the life radiant and fungi, and certain bacteria that inhibit the
growth and development of certain groups of microorganisms.
Antibiotics inhibit the growth and proliferation of microbial cells than create
favorable conditions for effective control of the body of the patient with an
infection. With the discovery of antibiotics began a new era in the prevention and
treatment of wound infection. Antibiotics were discovered in the 20th century.
More in 1871 professor of St. Petersburg Military Medical Academy, VA
Monassein revealed the ability of fungi to inhibit the development of certain
bacteria. AG Polotebnov mold applied for the treatment of festering wounds,
having a positive effect. In fact, the world's first antibiotic was in 1896, Italian
physician B. Gozio, which was isolated from Penicillium cultures mycophenolic
acid has a bacteriostatic effect on the causative agent of anthrax. Unfortunately,
this drug is not widely used. One of the first antibiotic in the early 20th century
have been obtained from a culture of Pseudomonas aeruginosa. However, the
drugs were unstable with a non-effect.
Black Americans Alsberg and in 1913 allocated penicillin acid having antimicrobial
activity. The First World War prevented its implementation in the clinic. Father of
antibiotics is considered to be an English scientist Fleming, who in 1929 raised the
fungus Penicillium notatum. It turned out that he is able to destroy streptococci
and staphylococci. Howard Florey in 1940 isolated from this fungus in a substance
called penicillin. He first used it in clinical practice. The resulting therapeutic effect
was so convincing that the Americans in the shortest possible time (in 1943)
establishing its industrial production. In Russia, the first Russian penicillin received
in 1942 academician Z. Yermolyeva.
In the following decades, there was intensive work on the allocation of new
antibiotics: in 1944 released streptomycin in 1947 - chloramphenicol, in 1952 erythromycin, in 1957 - kanamycin, in 1959 - rifampicin. In 50-ies. Cephalosporum
of the fungus was obtained from the first antibiotic cephalosporin group.
Currently available synthetic and semi-synthetic antibiotics.
Now a large amount of antibiotics used, but we can say with certainty that the
known drugs make up only a small part of this group. There are more than 2,000
substances having antibiotic activity, but only 200 are used in clinical practice.
Antibiotics are divided into the following groups.
1. Group of penicillin.
Biosynthetic penicillins: penicillin (sodium or potassium salt of benzylpenicillin),
Prolonged,: bitsillin, bicillin 3, bicillin 5,
Semisynthetic oxacillin, methicillin, ampicillin, amoxicillin.
Combined: ampiox (ampicillin+oxacillin),
Augmentin (amoxicillin+potassium salt of klavulanova acid),
Unasyn (ampicillin+sulbactam).
Clavulanate potassium and sulbactam are used as inhibitory the penicillinase
produced by the microorganisms and destroy penicillin.
Mechanism of action: inhibit cell wall synthesis of the microorganism.
Have a wide range of actions.
2. The group of streptomycin.
Streptomycin.
Mechanism of action: suppress function of the ribosome of a microorganism.
It has a wide spectrum of action.
Side effect: inhibit hematopoiesis, OTO -, and nephrotoxicity, hematotoxicity
3. The group of tetracyclines.
Tetracycline
Semi-synthetic: metacycline, doxycycline.
Mechanism of action: suppress function of the ribosome of a microorganism.
Have a wide range of actions.
4. The group of macrolides.
Erythromycin, oleandomycin, oletetrin, reporttitle, midecamycin, roxithromycin,
azithromycin, clarithromycin.
Mechanism of action: violates the synthesis of protein.
has an effect on gram-positive bacteria and weak or almost no effect on gramnegative.
Side effects: hepatotoxic, can cause dysfunction of the gastrointestinal tract
5. The group of aminoglycosides.
Kanamycin, gentamicin, tobramycin, sisomicin,
Semi-synthetic: amikacin, netromycin.
Mechanism of action: violates the synthesis of the cell wall of the microorganism
Have a wide range of actions.
Side effects: OTO - and nephrotoxic
6. Group of chloramphenicol.
Chloramphenicol, sintomitsina.
Mechanism of action: disrupt protein synthesis in the microorganism
Have a wide range of actions.
Side effect: inhibit haematopoiesis
7. A group of rifampicin.
Rifaximin (normix), rifamycin (rivoal), rifampicin (rifadin, rimactane).
Mechanism of action: disrupt protein synthesis in the microorganism
Have a wide range of actions.
Side effect: cause hypercoagulability, hepatotoxic
8. Group lincosamines.
Lincomycin, clindamycin
Mechanism of action: disrupt protein synthesis in the microorganism
9. The group of cephalosporins.
1st generation: ceporin, cephalexin, Cefazolin, cefamezin, kefzol,
2nd generation: cefamandole, cefmetazole, cefoxitin, cefaclor, cefuroxime,
cefotetan,
3rd generation: Ceftriaxone, Cefotaxime, cefixime, ceftibuten, cefpiramide,
ceftazidime,
4th generation: cefpirome (Kate).
Mechanism of action: violates the synthesis of the cell wall of the microorganism
Have a wide range of actions
Side effects: nefrotoksicski in high doses
10. Polymyxin B.
Affects gram-negative microorganisms, including Bacillus blue - green pus.
11. The group of antifungal antibiotics.
Nystatin, levorin, amphotericin b
Possess chemotherapeutic activity against pathogenic yeasts.
12. The group of fluoroquinolones.
3rd generation: ofloxacin, ciprofloxacin,
4th generation: levofloxacin, fleroxacin, tosufloxacin.
Mechanism of action: inhibit DNA girazu microorganism
Have a wide range of actions
13. Group carbapenemov.
Imipenem, Meropenem; combination drug: Tienam (imipenem+cilastatin sodium)
Mechanism of action: violates the synthesis of the cell wall of the microorganism
Have a wide range of actions
14. The glycopeptides.
Vancomycin.
The most common antibiotics are the so-called β-lactams. Such antibiotics include
penicillins and cephalosporins. Microflora coming into contact with these
antibiotics, begins to produce the enzymes splitting them (penicillinase,
cephalosporinase, β-lactamase)
On antibiotics last generations, these enzymes are not produced. So they have a
high activity and broad spectrum of action. Some antibiotics are specifically
injected lactamase inhibitors (clavulanate potassium Augmentin, sulbactam in
unatine).
Antibiotics can be divided into drugs with broad and narrow spectrum of action.
To broad-spectrum antibiotics, has a bactericidal action on gram-negative and
gram-positive flora, are semi-synthetic penicillins, cephalosporins and
aminoglycosides, semisynthetic tetracycline
Produce antibiotics of the first stage (penicillins, macrolides, aminoglycosides),
second stage (cephalosporins, semisynthetic aminoglycosides, Augmentin, etc.)
and backup (fluoroquinolones carbapenem). At the time of action of antibiotics
are divided into preparations of short and prolonged action.
In the initial period of antibiotics were intensively used in clinical practice, forcing
the Arsenal of therapeutic measures many antibacterial drugs. However, after 10
to 15 years, it has become clear that they do not fully justify imposing on them
expectations.
First, it was found that antibiotics can have harmful effects on the body. Second,
revealed that it may be antibiotic resistance of microorganisms. In many ways,
these negative aspects of antibiotic therapy due to a violation of the rules of
application of the latter.
Complications of antibiotic therapy
In conducting antibiotic therapy, you can experience the following complications.
1. allergic reactions,
2. toxic effects on the patient body .
3. dysbacteriosis.
4. the formation of resistant strains of microorganisms.
Allergic reactions. A large number of allergic complications due to the fact that
antibiotics are the drugs of biological origin, therefore, can cause sensitisation.
In clinical practice, the most common are the following allergic complications allergic rash (hives), angioedema, anaphylactic shock. Using antibiotics, you
should always remember about the possibility of allergic reactions, which in
extreme cases can lead to death of the patient. Major complications of antibiotic
therapy following:
Toxic effects on the patient. Many antibiotics have a toxic effect. Allocate OTO- ,
nefro- , haemato- , neurotoxicity, etc. are Often toxic effect is manifested in the
use of antibiotics for a long time, in large doses, without taking into account
comorbidity in the patient.
Dysbacteriosis. Observed with prolonged use of large doses of broad-spectrum
antibiotics. Often develops in children.
The formation of resistant strains of microorganisms. Resistant strains are often
formed in cases where dosage and frequency of administration of drugs.
Insufficient concentration of antibiotic in the blood to develop a mechanism of
resistance. In such cases, subsequent treatment with antibiotics may be
ineffective.
In order to avoid the negative consequences of antibiotic therapy, it is necessary
to observe strict rules of prescribing.
Principles of rational antibiotic therapy
1. Treatment with antibiotics on strict conditions.
2. The choice of antibiotic realize, based on the results of a study of the sensitivity
of microflora.
3. The avoid an allergic reaction, it is necessary to identify the allergic
predisposition of the organism (or from a history of treatment with antibiotics, or
after a tolerance test - the intradermal injection of antibiotic solution in low dose)
4. Prescribe antibiotics at optimal doses, strictly adhering to single and daily
dosage of the drug;
5. To observe the frequency of administration during the day to maintain the
desired constant concentration of the drug in the blood plasma.
6. While the use of multiple antibiotics should be consider the possibility of their
interaction (synergy, antagonism, indifference, the formation of toxic complexes).
Do not assign a treatment combination of antibiotics of the same group.
7. The use of the optimal route of administration of antibiotics.
8. Not to short or long courses of antibiotics, with no effect to produce timely
replacement of one type of antibiotic (or their combinations) on the other;
9. Keep in mind the possibility of side effects development and promptly
discontinue treatment with the appearance of their symptoms.
10. During the prolonged treatment to prophylactically prescribe antifungal drugs.
Antibiotics in surgery can be applied topically, orally, intramuscularly,
intravenously, intra-arterial, endolymphatic, enter in the internal cavity.
Algorithm for antibiotic therapy of surgical infections.
The rational is considered to be carrying out etiotropic antibacterial therapy, i.e.,
the choice of drug is determined by the results of microbiological studies. In most
cases, surgical diseases in which it is necessary to conduct antibiotic therapy treat
urgent. Therefore, surgeons are forced to treat empirically without knowing what
strain of microorganisms, resulted in the pathological process, of unknown their
sensitivity to antibiotics. In such situations, you should adhere to two principles.
1st principle - the use of an antibacterial drug maximum spectrum. In the
appointment treatment, pending the results of microbiological studies used
broad-spectrum antibiotics.
2nd principle of reasonable sufficiency. Treatment should begin with broadspectrum antibiotics first phase, in severe infections can start with a combination
of antibiotics first line or spending monotherapy antibiotic of the second stage.
Reserve antibiotics used in severe infections or ineffectiveness of other drugs.
After identification of strains of microorganisms and their sensitivity to
antibacterial drugs necessary to carry out a correction of the treatment, that is, to
go to etiotropic therapy.
Antibiotic therapy should be stepped. Having a positive effect, you can switch
from parenteral administration to oral forms of drugs of the same group, or
similar spectrum of activity.
Antibiotic prophylaxis
Until recently it was believed that the use of antibiotics prophylactically is
impossible. Now these views in the revised surgery. To prevent postoperative
complications, antibiotics are prescribed before surgery, administered during it.
Because of this, in the blood and in the area of operation at the time of its
execution creates a bactericidal concentration of the drug. For antibiotic
prophylaxis used cephalosporins 2nd and 3rd generation.
Proteolytic enzymes
The desire to accelerate the process of cleansing of infected wounds has led to
the use of proteolytic enzymes. Proteolytic enzymes do not destroy the
microorganisms, but have the ability to lyse (melt) nekrotizirovannye tissue,
fibrin, pus, have anti-edematous effect anti-inflammatory effect and enhance the
therapeutic effect of antibiotics. Isolated enzyme preparations:
1. of animal origin such as trypsin, chymotrypsin, himopsin, ribonuclease,
collagenase;
2. bacterial - turrilites, streptokinase (streptokinase), esperaza;
3. vegetable papain, bromelain.
The most widely proteolytic enzymes of animal origin (trypsin, himotripsin, the
drug containing both enzyme – himopsin). They are derived from the pancreas of
cattle.
Terrilitin - product life mold fungus Aspergillis terricola. Widespread ointment
iruksol. It is a combined preparation containing clostridiales, vydeleny from
Clostridium histolyticum and the antibiotic levomycetin.
Proteolytic products are widely used in the treatment of purulent wounds, trophic
ulcers. Thanks to them, it is possible to achieve the rapid cleansing of necrotic
tissue, essentially to produce necrectomy without a scalpel.
There are the following ways of application of enzymes:
1. intramuscular injection;
2. local application;
3. the introduction of enzymes using electrophoresis;
4. irrigation with a solution of proteolytic enzymes fistula and bone cavities;
5. intravenous injection;
6. intraosseous introduction;
7. inhalation method of administration;
8. endobronchial administration of enzymes;
Fagoterapii
The emergence of resistant to antibiotics and chemotherapeutic drugs strains of
bacteria, be forced to seek new methods of combating infection. For this purpose
you can use bacteriophages. Bacteriophage submicroscopic agent that has all of
the basic properties of viruses that can reproduce in the bacterial cell and cause
its death. They have a pronounced and typical species specificity. In surgical
practice used antistaphylococcal, antistreptococcal bacteriophages,
bacteriophage - Anticoli, as well as polyvalent bacteriophage that contains
multiple phages. Bacteriophages applied after the identification of the causative
agent, polyvalent and can be used when it is unknown.
Bacteriophages are used locally for washing and treatment of purulent wounds,
cavities,they can be administered through the drainage and mikroirrigatory, carry
out infiltration of surrounding tissues Endotrahealno introduce in purulent lung
diseases. Intravenous specific bacteriophage is used for sepsis.
Immunotherapy
Immunotherapy in patients with purulent infection gives a high clinical effect and
can be used as an independent method or in combination with antimicrobial
therapy.
There are three methods of influence on the immune system:
- passive immunization
- active immunization.
- immunomodulation.
Passive immunization is the introduction into the body ready-made antibodies to
certain pathogens of surgical infections. To do this, use preparations containing
antibodies: hyperimmune plasma, gamma globulins, serum. In Surgery is widely
used antistaphylococcal, antidiagonal, anticlimatically hyperimmune plasma.
Antistaphylococcal hyperimmune plasma is a native (liquid or frozen) blood
plasma of donors immunized with adsorbed staphylococcal toxoid. The titer of
antistaphylococcal plasma must be at least 6 ME. Plasma is used at severe
infectious diseases caused by S. aureus (sepsis, purulent peritonitis, osteomyelitis,
etc.).
The medication is administered intravenously once or repeatedly depending on
the condition of the patient, the dose is 4-6 ml/kg. is Usually used for 150 - 200 ml
a day (at the rate of 3 - 5 I/V infusions).
Antistaphylococcal gamma globulin receive from blood of donors immunized with
adsorbed staphylococcal toxoid. Available in sterile form in vials. Use of
antistaphylococcal gamma globulin for the treatment and prevention of diseases
caused by stafilokokkom. Is administered intramuscularly. One therapeutic dose
contains 100 IU of antitoxin. Produce 5 - 10 in/muscular injection of 5 ml every
other day.
Sandoglobulin— dried polyvalent human immunoglobulin. The drug is broad
spectrum and contains antibodies against bacteria, viruses and other pathogens.
Intravenously in severe bacterial infections, the dose is 0.4—1.0 g/kg daily for 1-4
days.
Tetanus gamma globulin receive from blood of donors immunized with tetanus
toxoid.
Available in sterile form in vials. 1 ml contains 150 ME anti-tetanus antibodies.
Used for prevention and treatment of tetanus. Is administered intramuscularly.
Tetanus serum - immune serum, obtained from blood of animals (horses)
immunized with tetanus toxoid. Used for prevention and treatment of tetanus.
Protivogangrenoznaya serum - immune serum containing antibodies to the major
causative agents of gas (anaerobic) gangrene.
Used for prevention and treatment of gas gangrene.
The means of passive immunization are given only short-term effect, so while it is
necessary to conduct active immunization.
Active immunization is the introduction of antigens for the produce of their
antibodies.
For this purpose, use of vaccines, toxoids.
Staphylococcal toxoid. it is administered fractional subcutaneously in the
subscapular region every 3 days in increasing doses from 0.1 to 1 ml After the
third injection, the titer of antitoxic antibodies increases 4 - 5 times or more.
Tetanus toxoid. Used for planned and emergency prevention of tetanus.
Immunomodulation.
For stimulation of immunity can be used various nonspecific stimulants: aloe,
autohaemotherapy, etc. Their drawback is that the stimulating action is
performed in the blind on the entire immune system, not the specific mechanism.
Therefore, at present, the aim should be not to immune stimulation and to
immunomodulation, that is, to act only on defective unit immunity. As
immunomodulators used drugs derived from the thymus affects T-population of
lymphocytes, various lymphokines, interleukins, interferons.
In surgery the most frequent use of prodigiozan, lysozyme, levamisole (dekaris).
Prodigiozan - bacterial polysaccharide activates T - system of immunity,
stimulates leucopoiesis and phagocytosis. Prescribed for reducing the activity of
phagocytosis and inhibition of leucopoiesis. Apply 50 mg 4 times a day at intervals
of 3-4 days.
Levamisole (decaris) stimulates the synthesis of antibodies, the formation of
phagocytes, T - lymphocytes. Prescribed for inhibition of phagocytosis.
Treatment rate (dose 150 mg). Administered 6 times a day every other day.
Lysozyme is a natural humoral factor of non-specific reactivity, bactericidal effect.
Enhances the effect of antibiotics, increases nonspecific resistance.
T I m a l n (Tamarin) - derived from the thymus gland (thymus) in cattle. Has a
stimulating effect on cellular immunity reactions, regulates the number of T - and
b-lymphocytes, enhances phagocytosis. Applied with acute and chronic purulent
processes, accompanied by a decrease in cellular immunity. Enter intramuscular
injection of 10-30 mg daily for 5-20 days
Taktivin - derived from the thymus gland of cattle.
Applied with inflammatory diseases, sepsis, when the revealed immunodeficiency
States with the defeat of the T - system. Use 1-2 µg/kg at night for 5-14 days.
In recent years began to use the interferons and interleukins. They have a more
focused and strong effects on the immune system. The most effective are new
drugs obtained by genetic engineering, Reaferon, Roferon, Ronkoleukin and
Betaleukin.
For stimulation of immunity using various in vitro methods of
immunomodulation: ultraviolet and laser irradiation of blood, hemosorption,
hyperbaric oxygenation, etc., These methods stimulate phagocytosis, the
complement system, improve the function of oxygen transport and rheological
properties of blood. They are used in the acute phase of the infectious process,
and also to prevent its recurrence. At the present time have started to apply
drugs xenoculture. Exercise perfusion using whole or fragmented spleen (the
spleen of the pig). You can cook xenophobic and suspended matter of spleen
cells. These methods involve the use of tissue contained in the spleen
lymphocytes and cytokines.
For stimulation of nonspecific resistance apply vitamin therapy, transfusion of
blood and blood products (plasma, suspended matter of lymphocytes).
MIXED ANTISEPTIC
The impact of these types of antiseptics on microbial cell and the microorganism
is not possible to reduce to a common mechanism. Their effect is in most cases
сomplex .
The surgeons in their work strive to get the maximum antiseptic effect and, as a
rule, use several types of antiseptics, and sometimes their entire Arsenal.
A classic example of the practical use of mixed antiseptic is a modern treatment
of wounds. Primary surgical wound treatment (mechanical and chemical
antiseptic), usually complemented biological antiseptical, physiotherapy, the use
of hypertonic solutions, drainages, etc., i.e. physical antiseptic. This
comprehensive use of various means of antiseptics is carried out under strict
indications and under the consideration of many factors (nature of the wound
and its contamination, the time since the emergence of the wound, the condition
of the patient, etc.).
Algorithm
sterilization of surgical instruments in the hot-cupboard
Phase I - preparatory. The goal - the preparation of tools to sterilization.
Spend soaking the instruments in the detergent solution, washing in a detergent
solution with a brush, thoroughly wash it under running water, rinsing with
distilled water, desiccation;
The SECOND main stage. The goal is sterilization.
Sterilized instrumentation in hot-cupboard at a temperature of 180°C - 60
minutes at a temperature of 160°C - 120 minutes, at a temperature of 140°C - 180
minutes;
The THIRD stage is the final. The goal is the quality control of sterilization.
Carried out by means of chemical indicators, which reflect the level required for
sterilization temperatures, which are laid in the closet along with the tool, or by
bacteriological methods - make a sowing of the tools on a nutrient medium.
Algorithm
sterilization in autoclave
Phase I - preparatory. The aim is to prepare the tools, linens, napkins and other
items for sterilization.
To do this, they are completed on appointment and placed on a napkin in Bix. The
last close tag, side vents are left open;
The SECOND stage primary. The goal is actually sterilization.
Sterilization of surgical instruments takes place in an autoclave under pressure. In
autoclave lay the bix of laying the material at the open side holes. Tightly close
the lid of the autoclave. Warming the autoclave, displace the air remaining in it,
raise the pressure to the desired level and temperature, depending on the mode
of sterilization (at 2 ATM. - 30 min., 1.5 ATM. - 45 min, 1.1 ATM. - 60 min.). After
sterilization, release the steam from the autoclave to bring the pressure up to
atmospheric, carefully open the lid of the autoclave, leave it open to cool (50°C).
After that, take out the bix , close the side openings. Make the tag a time stamp
and date of sterilization.
The THIRD stage is the final. The goal is the quality control of sterilization. For this
purpose, physical (powdered substances which have a melting point in the range
of 110-120°C), chemical ( thermotest - tape paper, impregnated with substances
which change their color at a certain temperature), technical (accounting for the
thermometer maximum temperature) and bacteriological (seeding swabs on a
nutrient medium) control methods of sterilization.
Algorithm
hand washing solution cutasept, sterilium, AHD 2000
Phase I - preparatory. Goal - hygienic hands processing.
Is clipping nails, pre-hand washing hygiene products, no brushes;
SECOND stage.- wiping hands. The goal is drying of hands. Spend wiping hands
sterile cloth;
The THIRD stage - the main. The purpose - the actual hand disinfection.
processing hands whith one of the solutions (Cutasept, sterilium, chlorhexidine)
twice in 5.0 ml of 5 minutes.
Algorithm
dressing operating underwear
I stage - dressing operating mask;
The SECOND stage of surgical processing ;
III stage - dressing the sterile operating clothes operating room nurse delivers the
gown, the surgeon pushes his hands into the sleeves, keeping them on urosemide
belt and chest
IV stage - tying a robe (sleeves tying each by itself or scrub nurse);
Stage V - sister give queue sterile gloves, holding their first finger to the middle,
turning and stretching the rubber ring, the surgeon inserts his hand in one motion
in glove.
So You can understand whether the initial level of knowledge and skills required,
it is proposed to perform a number of tasks, the correctness of the decision which
can be tested by comparison with standard answers:
1) in a patient with suppurative process, the limb used a sample of pus for
bacteriological examination. How long we will be able to obtain the results using
standard research:
a) after 1 day;
b) in 2-3 days;
C) 5-7 days;
grams) a month;
2) is it Possible to asepticize all layers of human skin without destroying it:
a) Yes, perhaps if you choose modern and effective tools;
b) is impossible because the microorganisms are located deep in the skin
appendages;
in) is possible in all cases, since microorganisms are only on the surface of the
skin;
g) is not only for spore-forming microorganisms;
3) To Elected two methods of sterilization of instruments with dry air and steam
at the same temperature and the same duration of treatment. Why the
destructive action of steam under these conditions the microorganisms will be
great:
a) because the moist environment is more unfavorable for microorganisms;
b)due to the greater heat capacity and heat transfer of steam;
C) in dry air survive spore-forming microorganisms;
4) in a patient with suspected infection from a wound taken smear-imprint. What
is the method of microbiological testing which can confirm the diagnosis in this
case:
a) microscopy;
b) bacteriological;
in) biomicroscopic.
5) nurse was treated with the hands with soap and antiseptic before washing the
urinary catheter have a heavy patient. What level of decontamination of the
hands should be attributed to such treatment before manipulation:
a) social;
b) hygienic;
b) to the surgical.
6) For preparation of a solution of s-4, for disinfection of hands, the first step,
prepare a mixture of hydrogen peroxide and formic acid. What substance is
formed during this chemical reaction:
a) water and formic acid;
b) perhydrol;
in) nagarajuna acid;
d) water and oxygen.
To control the study recommended training materials, we offer you to answer a
series of questions:
1) in a patient for 10 days after surgery there were signs of the inflammatory
process in the postoperative wound, the abscess is opened. Determine the
possible route of infection, if known, the cause of its development have become
infected thread for suturing the abdominal wall?
(a) exogenous;
b) contaction;
C) implant ;
d) endogenous;
e) criss-cross
2) the patient after the injury occurred suppurative process on foot, which it long
time was treated independently. Appealed for medical aid within the week. The
examination except purulent wounds of the dorsum of the foot revealed an
inflammatory infiltration of the upper thigh of the same limb. What is the route of
infection of the limb is most likely in this case:
(a) exogenous contact;
b) exogenous airborne;
C) exogenous implant;
d) endogenous contact;
d) endogenous nodal.
3) the nurse took a closed sterilization Bix out of the closet for use in surgery,
which was sterilized 2 days ago. What is the working life of sterile material and
linen in closed slut?
(a) up to 1 day;
b) up to 3 days;
in) up to 5 days;
d) up to 1 week;
d) up to 1 month.
4) In suhoor laid the instruments for sterilization. What are the parameters for
adequate sterilization?
a) 160°C - 30 minutes;
b) 180°C - 60 minutes;
C) 180°C - 30 minutes;
g) 200°C for 60 minutes.
5) the nurse must sterilize optical instruments. Select for this purpose the
necessary means of sterilization.
a) ahogar;
b) paraformaldehye camera;
C) a 6.0 % solution of hydrogen peroxide, the autoclave;
g) autoclave
d) radiation sterilization;
6) Before sterilization decided to hold a pre-sterilization control preparations
tools. Select from the listed favorites for this two samples:
a) benzoic acid and resorcinol;
b) benzidine and fenolftaleina;
in) antipirina and ascorbic;
d) with thiourea and succinic acid;
d) antipirina and glucose.
7) Select from listed modern antiseptic for the treatment of hands and surgical
field before surgery:
(a) pervomur, 5.0 per cent alcoholic solution of iodine, diamond green, 70.0% of
the alcohol;
b) 70.0% of the alcohol, zeigel, hlorgeksidin, furatsilina;
in) 0,5 % solution of ammonia, to 96.0 % alcohol, povidone-iodine, desmin;
g) sterilium, AHD, Piramides, cutasept;
d) to 96.0 % alcohol, 3.0 percent alcoholic iodine, poligonului solution of iodine,
chlorexidine.
8) During sterilization and after completion it used a variety of controls. Which of
the controls allows to get objective information about the quality of sterilization?
(a) bacteriological;
b) biochemical;
in) thermometric;
g) thermoinduction;
d) physical.
9) a nurse has prepared for sterilization multiple target positioning to perform
surgical procedures. Name which pilings can be sterilized in autoclave?
(a) linen, metal instrument, the cystoscope, the filament;
b) napkins, rubber catheters, metal tool, gloves;
in) napkins, gloves, sigmoidoscopy, tool;
d) linen, tampons, laparoscope, gloves.
10) When the surgeon wore a robe, he snagged a medic hand. That it is
appropriate to do in this situation?
(a) to remove clothing, repeat treatment again;
b) treating the hands with alcohol;
C) to continue dressing, and then further processed hand;
g) to change clothes without repeating the treatment of hands.
So You can understand whether the initial level of knowledge and skills required,
it is proposed to perform a number of tasks, the correctness of the decision which
can be verified by comparing with the standard answers:
1) Select the mechanism of action of an antiseptic, which displays a bactericidal
effect?
a) coagulation of the cellular membrane;
b) violation of the reproduction;
C) violation of intracellular synthesis;
2) What are vaccines?
a) bacterial, viral
b) fungal
C) physical,
g) chemical,
d) biological;
3) aided by injecting serum into the human body?
a) the development of active immunity;
b) the development of passive immunity;
C) increase non-specific reactivity of the organism
g) development of serum based on.
4) Which substrate is a immune serum? This:
a) weakened the culture of microorganisms;
b) the set of antibodies;
C) toxoid;
g) specific antigens of microorganisms
5) That represents the aggregate state of chemically pure iodine?
a) a solid substance;
b) liquid;
C) the gas;
6) What are the frequency characteristics relate to ultrasound?
a) oscillation with frequency up to 16 Hz
b) oscillation with a frequency in the range 16 - 20000 Hz;
in) oscillation with a frequency over 20,000 Hz;
7) What constituted a material property as hygroscopic?
a) suction of fluids;
b) the ability to easily give liquid;
C) the ability to pass the liquid;
8) Coagulation of the protein may occur due to the action of heat, acids, some
chemicals. What if this occurs?
a) protein breakdown;
b) protein synthesis;
C) coagulation of protein.
To control the study recommended training materials, we offer you to answer a
series of questions:
1) patients with cellulitis of the limbs underwent a complex treatment, which
includes parenteralno and local use of antiseptics. Which of the following
antiseptic agents are referred to the biological antiseptic?
a) intramuscular immunoglobulin;
b) excision of the affected tissue;
C) treatment of the wound with 3% solution of hydrogen peroxide;
g) treatment of the wound with an alcoholic solution of chlorophyllipt;
d) ultraviolet irradiation wounds.
2) to Achieve the deepening of antibacterial action for external use of antiseptics
by using physical methods (electrophoresis, ultrasound). But among antiseptics
are those that penetrate through the intact skin quite deeply. Select them:
a) chloramine and chlorhexidine;
b) 70% alcohol and dimexide;
C) 98% alcohol and potassium permanganate;
g) furatsilin and diamond green;
d) boric acid and silver nitrate.
3) Which of antiseptics possess coagulating effect?
a) chloramine;
b) phenol;
C) lysoformin;
g) Ichthyol;
d) silver nitrate.
4) the patient has osteomyelitis of the tibia. Select tools the introduction of
antiseptics, which allow you to minimally to reduce their elimination and to
achieve maximum concentration in the area of inflammation.
(a) intra-arterial, intraosseous;
b) intravenously, endolimfaticaki;
in) oral, intramuscular;
g) subcutaneous application;
d) intramuscular, intravenous.
5) The patient on the operating table be carrying out the surgical field of skin
processing with a disinfectant solution. Which of these solutions can cause burns
to the skin after treatment?
(a) yodonat;
b) yodopiron;
C) 5-10 % solution of tincture of iodine;
g) chlorexidine digluconate;
d) cutasept.
6) a surgery about injection abscess. Abscess cavity was washed with a solution of
hydrogen peroxide, chlorhexidine. For wound drainage operating sister told the
surgeon gauze drainage together with a rubber band. Than it is advisable to
handle the gauze drainage to enhance the osmotic action of the gauze?
a) hypertonic solution of sodium chloride;
b) a solution of furacilini;
C) 5-10 % solution of tincture of iodine;
g) hydrophobic ointment on the basis of;
d) Ichthyol ointment.
7) the Patient received a bruised shin injury. On the third day arose festering
wounds with necrosis of the skin of this section in the area of inflammation. What
is the antiseptic method should be used primarily for such a patient?
(a) biological - the introduction of a bacteriophage;
b) chemical washing solution furatsilina;
in manual - run necrectomy;
g) physical - the use of ultraviolet irradiation of the wound;
8) the patient has a deep wound infection of the hip after the disclosure of
phlegmon
. Which method of drainage is most effective for the early cleansing of the wound
cavity?
a) passive drainage of the latex band;
b) passive drainage with a rubber tube;
C) active flow-drainage.;
g) passive drainage with gauze tape;
d) drainage with hypertonic solution.
9) Select from listed modern antiseptic for treatment of hand surgery and surgical
field:
a) 5% alcoholic solution of iodine, 0.5% chloramine, 96 % ethanol;
b) 0.5% solution of ammonia, pervomura solution of brilliant green;
in) sterilium, cutasept, AHD 2000;
d) chlorhexidine, 0.5% ammonia solution, 70 % ethanol solution;
e) zeigel, povidone-iodine 5% alcohol solution of iodine.
Main literature:
• General hirurga / edited by S. P. Gusenka, M. D. Gelba, S. D. HMA. To: "Health",
1999
• Petrov S. V. General surgery. - Saint Petersburg: "LAN", 2002
Additional literature:
• I. P. Cherenko, J. M. Vavryk General chirurgia. To: "Health", 1999.• Surgery. Vol. 1: Textbook of General surgery / edited by J. S. Bereznikovo, M. P.
Zakharash, V. G. Mishalov, V. O. Shidlovska: DITCH "Dnipro-VAL", 2006.
• Y. V. Werewolves General surgery. Riga."Zvaygzne",1989