Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Compounding wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical marketing wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Tablet (pharmacy) wikipedia , lookup
Prescription costs wikipedia , lookup
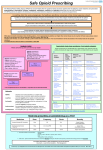
David Todd Loffert B.S., M.H.S., (Ph.D. Candidate) Addiction is a primary, chronic, neurobiologic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. Addiction is characterized by behaviors that include one or more of the following: • Impaired control over drug use • Compulsive use • Continued use despite harm • Cravings Rx Addicted Doctors Lawyers Attorneys Newscasters Housewives Businessmen Young Teenagers Athletes Politicians Celebrities 1 • Sobriety 2 • Jails / Institutions 3 • Death 2011 • 21 Million Americans using prescriptions for non-medical use (addicted) 2011 • Non-medical use of prescription drugs the #1 drug of abuse in U.S. 2011 • 30,000 overdoses in U.S. 2011 • Prescription Drug Abuse Results in One Death Every 19 Minutes in U.S. 2010 • 39 out of 50 states have a Prescription Drug Monitoring Program 2009 • Over 1 million visits to ERs for drug related complications Rates of Prescription Painkiller Sales, Deaths and Substance Abuse Treatment Admissions (1999-2010) SOURCES: National Vital Statistics System, 1999-2008; Automation of Reports and Consolidated Orders System (ARCOS) of the Drug Enforcement Administration (DEA), 1999-2010; Treatment Episode Data Set, 1999-2009 Prescription Drug Overdose Death Rates By State per 100,000 People (2008) SOURCE: National Vital Statistics System, 2008 1 • The drug or other substance has a high potential for abuse, no medical use. 2 • The drug or other substance has a high potential for abuse, medical use. 3 • The drug or other substance has a potential for abuse less than the drugs or other substances in Schedules I and II. 4 • The drug or other substance has a low potential for abuse relative to the drugs or other substances in Schedule III. 5 • The drug or other substance has a low potential for abuse relative to the drugs or other substances in Schedule IV. 1 • Prescription Drugs (2-5) 2 • Marijuana (1) 3 • Cocaine (2) 4 • Heroin (1) 5 • Methamphetamine (2) 1 • University of Northern Colorado, B.S. in Biology and Chemistry 2 • Johns Hopkins University, Master of Health Science in environmental/radiation/respiratory health 3 • Medical College of Virginia/Virginia Commonwealth Universtiy, Ph.D. in respiratory medicine 4 Peer-Reviewed Journal Articles 53 Papers Presented At Various Medical Conferences & Meetings Contributing author for the book, “Inhalation Aerosols, Physical and Biological Basis for Therapy” by Anthony J. Hickey Masters Thesis: Fundamentals of Aerosol Delivery to the Respiratory Tract with an Emphasis on the Performance of Medicinal Spacer Devices Delivery of glucocorticoids by jet nebulization: Aerosol characteristics and output Jeffrey Leflein, MD, a Eleanor Brown, MT(ASCP), a Malcolm Hill, PharmD, a H. William Kelly, PharmD, b David Todd Loffert, BS, a Harold S. Nelson, MD," and Stanley J. Szefler, MD ~ Denver, Colo., and Albuquerque, N.M. Background: Since inflammation has been identified as a critical factor in the pathogenesis of asthma, use of inhaled glucocorticoids has increased. Because young children are often unable to coordinate properly the use of metered-dose inhalers and no glucocorticoids preparations for nebulization have been approved in the United States, parenteraI and intranasal glucocorticoids preparations are occasionally administered by nebulization. Methods: We examined whether a parenteral preparation (triamcinolone acetonide [TAA]; Kenalog) could be delivered by nebulization. TAA, 1000 txg (0.1 ml), was placed in the nebulizer bowl (MB5 [MeFar, Brescia, Italy] or Pari-Jet [Dura Pharmaceuticals, San Diego, Calif.]), then diluted with 2. 9 ml normal saline solution for a total volume fill of 3 ml. Using a laser panicle analyzer, high-performance liquid chromatography, and cascade impactor, we examined the percentage of aerosol volume produced with panicles in the respirable range of 1 to 5 lazn in diameter, actual TAA output (in micrograms) and concentration of TAA contained in the panicles within the respirable range. Results: Laser particle analysis indicated that 34% +- 3% (mean +- SEM) (MB5) and 47 +3% (Pari-Jet) of the total aerosol volume produced were within the respirable range of I to 5 txm in diameter, and this remained consistent throughout nebulization. The nebulizer was stopped serially for determination of TAil output with high-performance liquid chromatography. TAA output (1000 tzg less the amount in micrograms remaining after nebulization) was essentially complete after 2 minutes with the Pari-Jet and within 4 minutes with the MB5 and totaled 352 +- 19 ixg and 367 +-- 9 Ixg, respectively. Finally, cascade impactor studies confirmed that 33.4% of the TAil aerosol generated by the MB5 nebulizer was contained in panicles in the respirable range. Conclusion: Approximately 35% (Pari-Jet) and 37% (MB5) of the initial 1000 lag of TAA was delivered with the two nebulizers tested. The panicles generated within the respirable range were limited to 34% (MB5) and 47% (Pari-Jet) of the amount delivered. TAA was equally distributed in the particles generated. The theoretic amount delivered in the respirable range was approximately 12.5% for the MB5 nebulizer on the basis of the cascade impactor and 16.5% for the Pari-Jet (assuming TAA distribution equivalence) of the TAA placed in each of the nebulizers. Additional clinical studies are needed to define efficacy and safety in view of the excipients used in preparing the parenteral preparation. (J ALLERGY CLIN IMMUNOL 1995;95:944-9.) Key words: Triamcinolone acetonide, glucocorticoids, laser panicle analyzer, high-performance liquid chromatography, cascade impactor. COMPARISON OF DISPOSABLE JET NEBULIZERS, A METHOD FOR DETERMINING WHICH BRAND TO USE. D. Todd Loffert, PARI Respiratory Equipment, 7493 Whitepine Road, Richmond, Virginia, 23237. Four commercially available nebulizers from 4 sources were studied (Misty-Neb/Baxter, PARI LCD/PARI, Updraft II/Hudson RCI, and Whisper Jet/Marquest medical). The nebulizers were operated using an PARI Master compressor and reanalyzed with an Devilbiss Pulmo-Aide compressor. Delivery rate(Ml/Min), percent Particles in the Respirable Range(PRR), Respirable Particle Delivery Rate(RPDR), and standard deviation of all parameters were compared. All nebulizers were filled with 2.5 ml of saline. PRR was measured by continuous sampling by Laser Particle Analyzer, Malvern Mastersizer X. The nebulizers were sampled at a simulated flow rate of 20 liters per minute. PARI MASTER COMPRESSOR Ml/Min varied from 0.23 to 0.56 ml/min. The Whisper Jet (0.23) had the lowest ml/min while the PARI LC-D (0.56) had the highest. PRR varied 22.74 to 59.89%. The Misty-Neb (22.74%) had the lowest PRR while the PARI LC-D (59.89%) had the highest. To combine the previous variables RPDR was calculated, = Ml/Min multiplied by PRR. The Misty-Neb (0.06) had the lowest RPDR while the PARI LC-D (0.34) had the highest RPDR (means significantly different at p<0.0001). PULMO-AIDE COMPRESSOR Ml/Min varied from 0.14 to 0.48 ml/min. The Whisper Jet (0.14) had the lowest ml/min while the PARI LC-D (0.48) had the highest. PRR varied 25.00 to 51.92%. The Misty-Neb (25.00%) had the lowest PRR while the PARI LC-D (51.92%) had the highest. To combine the previous variables RPDR was calculated, = Ml/Min multiplied by PRR. The Misty-Neb (0.04) had the lowest RPDR while the PARI LC-D (0.25) had the highest RPDR (means significantly different at p<0.0001). The Ml/Min, PRR, and RPDR of the commercially available nebulizers varies greatly with each compressor used. Consideration must be given to these efficiency parameters when deciding which nebulizer brand to use. Comparison of the bronchodilator response to albuterol administered by the OptiHaler, the AeroChamber, or by metered dose inhaler alone. Nelson HS, Loffert DT. National Jewish Center for Immunology and Respiratory Medicine, Denver, CO 80206. Eighteen subjects with moderate asthma participated in this double-blind study comparing the bronchodilator response to albuterol or placebo used in conjunction with three inhalation devices; the metered dose inhaler (MDI) actuator alone, the AeroChamber, and the OptiHaler. The principal comparison was the increase in FEV1 over 30 minutes. Also recorded were heart rate, time required to use each device, and patient acceptance of each device. There was a large bronchodilator response with albuterol with each of the devices, but there was no difference in the promptness or the magnitude of the bronchodilator response among the three devices. There was a small but statistically significant increase in heart rate which did not differ among devices. Subject ratings of acceptability were MDI alone best, followed by OptiHaler, then AeroChamber. We conclude (1) the bronchodilator response obtained with use of the MDI alone, the AeroChamber and OptiHaler were not significantly different; (2) patients, as a group, found the MDI required less time to use and they favored it over either spacer; (3) while in subjects employing good MDI technique, the addition of either an AeroChamber or an OptiHaler did not improve bronchodilator response. Spacers may have a role in those with poor inhaler technique or in conjunction with inhaled corticosteroids. “If you were stranded on a desert island, what pain medicine would you want to have with you” FDA Schedule Visit # 2 1 Prescription Demerol 100mg tubex shots (needles) #RX Ordered/Refills 5 Date Rx Written 7/30/1998 Last Filled XXX 2 1 Demerol 100mg Tablets 60 7/30/1998 XXX 2 1 Dexedrine 5mg Tablets 30 7/30/1998 XXX 2 1 Mepergan (Demerol & Phenergan) 60 7/30/1998 XXX 4 1 Valium 100 / w3 Refills 7/30/1998 XXX 2 1 Percocet 10mg Tablets 100 7/30/1998 XXX FDA Schedule Visit # 2 Called in between visit 1-2 Prescription Percocet 10mg Tablets #RX Ordered/Refills 100 Date Rx Written 8/10/1998 Last Filled 7/30/1998 2 Called in between visit 1-2 Dexedrine 5mg Tablets 60 8/11/1998 7/30/1998 2 Called in between visit 1-2 Dexedrine 5mg Tablets 60 9/15/1998 8/11/1998 2 Called in between visit 1-2 Demerol 100mg Tablets 60 10/6/1998 7/30/1998 2 Called in between visit 1-2 Demerol 100mg Tubex (needles) 20 8/28/1998 7/30/1998 FDA Schedule 2 #RX Ordered/Refills 100 Date Rx Written 10/20/1998 Visit # 2 Prescription Percocet 10mg Tablets Last Filled 8/10/1998 2 2 Dexedrine 5mg Tablets 100 10/20/1998 9/15/1998 2 Called in between Demerol 100mg visit 2-3 Tubex Shots (needles) 20 11/18/1998 8/28/1998 2 Called in between Demerol 100mg visit 2-3 Tablets 60 11/18/1998 10/6/1998 4 Called in between Valium 5mg visit 2-3 Tablets 100 / w4 Refills 11/18/1998 7/30/1998 FDA Schedule 2 Visit # 3 2 3 2 3 #RX Ordered/Refills 100 Date Rx Written 12/4/1998 Last Filled 10/20/1998 Dexedrine 5mg Tablets 120 12/4/1998 10/20/1998 Mepergan (Demerol & Phenergan) 100 12/4/1998 7/30/1998 Prescription Percocet 10mg Tablets FDA Schedule Visit # Prescription #RX Ordered/Refills Date Rx Written Last Filled 2 Called in between visit 3-4 Percocet 10mg Tablets 100 12/21/1998 12/4/1998 2 Called in between visit 3-4 Demerol 100mg Tablets 100 12/15/1998 11/18/1998 2 Called in between visit 3-4 Demerol 100mg Tubex Shots (needles) 20 12/21/1998 11/18/1998 4 Called in between visit 3-4 Valium 5mg Tablets 100 / w4 Refills 12/15/1998 11/18/1998 2 Called in between visit 3-4 Dexedrine 5mg Tablets 120 12/21/1998 12/4/1998 2 Called in between visit 3-4 Percocet 10mg Tablets 100 12/31/1998 12/21/1998 2 Called in between visit 3-4 Dexedrine 5mg Tablets 120 12/31/1998 12/21/1998 2 Called in between visit 3-4 Mepergan (Demerol & Phenergan) 100 2/15/1999 12/4/1998 2 Called in between visit 3-4 Demerol 100mg Tablets 100 2/24/1999 12/15/1998 FDA Schedule Visit # 2 4 Prescription Dexedrine 5mg Tablets #RX Ordered/Refills 100 Date Rx Written 3/10/1999 Last Filled 12/31/1998 3 4 Vicodin HP 10mg Tablets 100 / w3 Refills 3/10/1999 XXX 4 4 Valium 100 / w3 Refills 3/10/1999 12/15/1998 xx 4 Ultram 50mg 100 / w6 Refills 3/10/1999 XXX xx 4 Ultram 50mg 100 / w3 Refills 3/10/1999 XXX 4 4 Klonopin 60 / w3 Refills 3/10/1999 XXX FDA Schedule Visit # 3 Called in after visit 4 3 Prescription Vicodin HP 10mg Tablets #RX Ordered/Refills 100 / w3 Refills Date Rx Written 3/28/1999 Last Filled 3/10/1999 100 3/31/1999 3/28/1999 Called in after visit 4 Vicodin HP 10mg Tablets Total # of Visits Total Days Under Dr. Suter’s Care Total # of Pills Average Pills Per Day 4 243 (7.9 Months) 6,647 27.35 655 • FIRST VISIT 710 • DEXEDRINE 5MG 380 • DEMEROL 100MG 600 65 1800 • VALIUM 5MG 900 • VICODIN HP 10MG 260 • MEPERGAN (DEMEROL & PHENERGAN) • PERCOCET 10MG • DEMEROL SHOTS 100MG 1100 • ULTRAM 50MG (1 VISIT) 09-24-99 Cary G. Suter, M.D., 0101-011492, Richmond, VA – Acceptance of surrender of license, in lieu of further administrative proceedings, based upon inappropriate prescribing of controlled substances and inadequate documentation and monitoring of this prescribing. 1 • After months under Dr. Suter’s care, I decided to stop. 2 • On my way home from school. 3 • Started to have a horrible feeling. 4 • Ended up in the hospital that night with severe withdrawal complications/symptoms. 9 2 8 7 0 6 0 0 0 9 15 7 13 16 0 10 0 23 87 29 20 5 4 16 3 419 20 21 16 1 24 1 19 2 12 8 109 18 648 31 11 0 46 13 24 32 • GERMANY 12 • CARIBBEAN 8 • AUSTRIA 21 • MEXICO 10 • HOLLAND 4 • JAPAN 12 • PAKISTAN 5 • SPAIN 15 • CANADA 9 • BRAZIL 17 • BERMUDA 65 11 • INDIA Controlled Substance Rx Doctors Internet ER’s Walk-In Clinics Forged Insurance When Had It Rehab Facilities Foreign Countries THROUGHOUT MY 9 YEARS OF ADDICTION THE FOLLOWING EVENTS HAD A SIGNIFICANT DETRIMENTAL EFFECT IN MY LIFE 1) 67,457 controlled substance pills ingested 9) Fired from 5 prominent scientist positions 2) 45 grand mal seizures 10) 19 prescription related arrests 3) 323 narcotic related hospital visits 11) 180 forged prescriptions 4) 9 in-patient rehabilitation programs 12) 2 suicide attempts 5) Homeless 3 different times 13) 167 bad checks for prescriptions/Dr. visits 6) 35 hospitalizations from drug overdoses 14) 1,434 medical visits to obtain narcotics 7) Total medical debt over 9 years = $310,650.00 8) Dropped out of my Ph.D. due to addiction issues Lecture in Atlanta Forged Demerol Rx Arrested At Conference Taken Past Colleagues In Handcuffs Spent 2 Weeks In Atlanta Jail On Way To Conference Had Drug Seizure Hit Wall, Rolled 3 Times High On Prescription Drugs Looking For My Dog Woods Behind House 4 Masked Individuals With Guns Burglarizing Houses Walking Away Waiting To Be Shot Desperation No Way Out Continuous Physical & Emotional Pain 1 • Denver Cares 2 • PEER I (Needed at least 1 yr.) 3 • Family 4 • Acceptance/Responsibility 5 • Has Become a High Risk 1 • During Employment (1 Day) 2 • Arapahoe House (1 Week) 3 • West Pines (2.5 Weeks) 4 • Step 13 (2 Months) 5 • Denver Rescue Mission (6 Months) 6 • PEER 1 (1 Year) 1 • Publish From Hopkins to Homeless: My True Story of Prescription Drug Addiction 2 • Complete My Doctorate In Public Health Education (1 Year Before Completion) 3 • Find Full-Time Job In Public Health or In The Addiction or Addiction Related Field 4 • PRePARe (People Recovering from Prescription Addiction and Relapse) 5 • Maintain Positive Outlook 1 • CELL = 303-898-7859 2 • E-MAIL = [email protected] 3 • P.O. BOX 631344, LITTLETON, CO. 80163-1344