Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
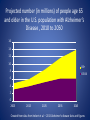
Palliative care, hospice and dementia: Are we providing the right care at the right time? Jean Jaoude, MD, MHA, CMD Medical director UnityPoint Hospice and Palliative care [email protected] Participants will be able to: • Describe the differences and similarities of hospice and palliative care • Identify the aging changes effect on end-of-life geriatric care • List the Do's and Don'ts in advanced dementia and end-of-life care Case 1 84 y.o. patient with metastatic lung cancer decides to forgo further treatment after failing several chemotherapy trials. He reports he is weak and unable to enjoy his hobbies of fishing and traveling anymore. He spends most of his time in his recliner. His wife helps him with dressing which is every 3 days now . Bathing is limited to once a week. With assistance of his wife and his walker, he takes couple of steps only and needs to sit down due to shortness of breath and fatigue. He reports no appetite and a weight loss of 40 pounds over the past 2 months. Case 1(cont’d) He wishes to focus on his quality of life and have his pain and dyspnea under better control. He asks for your opinion in regards to hospice referral. you should: 1- Refer to palliative care since this is a must step prior to hospice referral 2- Disagree with him and encourage enrollment in a new research chemotherapy trial 3- Counsel him about hospice care and proceed with the referral 4- Explain to him that once he chooses to enroll, he cannot revoke hospice care Case 2 91 y.o. patient with Alzheimer’s dementia lives at home with his daughter. She has been taking care of him for the past 5 years. Over the past 6 months she noticed he has been spending most of his time in bed. He has been unable to bear any weight and is non-ambulatory. He is dependent on his daughter for bathing, dressing, and feeding. He is incontinent of urine. He does not interact with family or surrounding. Over the past 2 months, he has been taking only bites of his meals and sips of his fluids with occasional cough episodes. Case 2(Cont’d) Daughter is concerned about weight loss and dehydration. she asks for your opinion. you counsel her and recommend to: 1- Admit patient to the hospital and start IV fluids 2- Insert PEG tube and start feeding 3- Offer oral assisted feedings 4- Place PICC line and start TPN indefinitely Aging Population Aging Population millions 90 80 70 60 50 85+ 40 75-84 65-74 30 20 10 0 2010 2020 2030 Source : Us census Bureau 2008 2040 Aging Population • • • • • Higher comorbidities Complex medical problems Increased Rate of dementia Stress on the healthcare system Questionable model of care(i.e. acute care model) Baby Boomers Aging and physiologic changes Renal: • Renal mass decreases 25-30% • Number of nephrons decreases(kidney adapts to loss of nephrons by compensatory hyperfiltration and/or increasing solute and water reabsorption in the remaining nephrons) • Serum creatinine is unchanged • Creatinine clearance decreases Aging and physiologic changes Renal(continued): Age CrCl Aging and physiologic changes Cardiovascular: • Maximum heart rate declines(220-age in males) • Maximum cardiac output declines(At rest, cardiac output tends to be normal. It declines with stress) • Increase in systolic BP(not age-related only) Aging and physiologic changes Nervous system: • Decrease in brain volume(20%) • Asymmetric loss of neurons Vision: • Decrease in light adaptation(when walking in dark room) • Lacrimal gland function decreases • More sensitive to glare because of light dispersion in the lens Aging and physiologic changes Hearing: • High frequency hearing loss Respiratory: • Lung elasticity and elastic recoil decreased • Decreased FEV1 Musculoskeletal: • Muscle mass decreases • Bone mass/density decreases Aging and physiological changes Hematopoietic: • Hct and WCC are unchanged (WCC may not be elevated during an infection) • T-cell function is decreased (immunological response to vaccine is reduced) Digestive: • Decreased function of the GE junction(thus more reflux prone) • Decreased bowel transit time (thus more constipation prone) Aging and physiological changes Liver: • Liver mass decreases by 25-35% and blood flow by as much as 40% by age 90. Thus: • Diminished first-pass metabolism Increased drug serum concentration(i.e. nitrates, Bblockers, CCB etc.) • Diminished metabolic pathways(Cytochrome P450-Phase 1 reaction) Decreased oxidation, hydroxylation, demethylation Increase in drug half-life(i.e. diazepam, alprazolam, NOT Lorazepam-Phase 2) Impact on caring for the elderly • Adjust medication dose(Renal and liver changes) • Greater degree of illness and debility like dehydration and quicker acute renal failure(renal and cardiac changes) • Less physiologic reserve thus myocardial infarction and congestive heart failure prone( cardiac changes) • Patients more prone to confusion(Brain changes) • More prone to reflux thus prone to aspiration even if PEG use(GI changes) Dementia Projected number (in millions) of people age 65 and older in the U.S. population with Alzheimer’s Disease , 2010 to 2050 16 14 12 10 85+ 8 65-84 6 4 2 0 2005 2015 2025 2035 2045 Created from data from hebert et al. – 2013 Alzheimer’s disease facts and figures Average annual per-person payments for health care services provided to Medicare beneficiaries age 65 and older Beneficiaries with Alzheimer’s and other dementias Beneficiaries without Alzheimer’s and other dementias Inpatient hospital $ 10,293 $ 4,138 Medical provider $ 6,095 $ 4,041 Skilled nursing facility $ 3,955 $ 466 Hospice $ 1,821 $ 178 Home health $ 1,460 $ 471 Prescriptions medications $ 2,787 $ 2,840 Created from data from the Medicare current beneficiary survey for 2008 Percentage changes in selected causes of death (all ages) between 2000-2010 100% 80% 68% 60% 40% 20% 0% Alzheimer Stroke Heart disease Breast cancer -20% -40% Data from the National Center for health statistics -2% -16% -23% What is palliative care? • Palliative care is specialized medical care for people of any age with serious illnesses. It is focused on providing patients with relief from the symptoms, pain and stress of a serious illness, whatever the diagnosis. • The goal is to improve quality of life for both the patient and the family. Who is palliative care appropriate for? • Palliative Medicine is appropriate at any age and at any stage in a serious illness, and can be provided together with curative treatment. • Life limiting disease like(not limited): – COPD – CHF – Cancer – Dementia – Parkinson Palliative Care Services • • • • Goal clarification IPOST development Symptom management Education/ chronic disease management • Coordination of care • Medical director • Nurse practitioners/Physicians • Social workers • Nurses • Bereavement/chaplain you may be mistaken for … Communication • Communication with patients, families, providers, multidisciplinary team • Family conferences • Tips for communication “Family wants everything done” Goal clarification • Considering the patient’s disease process, what is the patient’s goal? • Goal clarification is key • End of life wishes • Advanced directives • IPOST – Iowa Physician Orders for Scope of Treatment Coordinate • Coordinate care of patients among various agencies • Coordinate and share plans of care • Access resources • IDT Support • • • • • Facilitation of family conferences Community Resources Financial Assessment Transfer to new setting Advance Directives Symptom management • Collaborating with others to provide symptom relief • Physical symptoms • Emotional symptoms • Spiritual symptoms Hospice • Care designed to give supportive care to people in the final phase of a terminal illness and focus on comfort and quality of life, rather than cure. • The goal is to improve quality of life for both the patient and the family. END-of-Life care Services • Case Management • Symptoms management • Social and emotional support • Spiritual care • Assistance with ADL’s • Volunteers • Medications • Supplies/equipment • • • • • • • Medical director Nurses Social Workers Chaplain Volunteers Certified Nursing Aides Music, pet and massage therapy Medicare Hospice Benefit • • • • Professional services Medical equipment/ supplies Medications 4 Levels of care – Routine home care – Continuous care – Short term inpatient care – Respite care End-of-Life • • • • Hospitals major site for end-of-life care Rate of hospital death is 30% * Setting goals at the end of life Discussing values, preferences and goals with patients • CMS approved reimbursement for providers discussing advance care planning * JAMA, January 2016 End-of-life Guidelines for discussions 1. Begin conversations early in the illness 2. Ask about their understanding of current medical condition 3. Assess patient’s and family’s information-sharing preferences 4. Answer clearly with jargon’s-free information about patient’s condition, prognosis and options 5. Ask about unacceptable states 6. Inquire about patient’s concerns 7. Recommend a plan for end-of-life care Comfort care for patients dying in the hospital Craig D Blinderman, MD and J. Andrew Billings, MD N Engl J Med, December 24, 2015 The conversation Do’s and Don’ts in advanced dementia and end-of-life care (Choosing Wisely) Do • Screen for dementia in your clinic(USPSTF- Evidence Insufficient to assess the balance of benefits and harms of screening for cognitive impairment) • Start the conversation early(NEJM). Don’t • Don’t delay palliative care for a patient with serious illness who has physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment(HPM). • Don’t delay engaging available palliative and hospice care services in the emergency department for patients likely to benefit(ER). Do’s and Don’ts in advanced dementia and end-of-life care (Choosing Wisely) Do • Avoid prescribing appetite stimulants and high calorie nutritional supplements in elderly with anorexia and cachexia(AGS). • Discontinue medications that may interfere with eating. Provide appealing food, feeding assistance, measures for optimizing social supports, and means to clarify patient goals and expectations(AGS). Don’t • Don’t recommend percutaneous feeding tubes in patients with advanced dementia; instead, offer oral assisted feeding(HPM, AGS, AMDA). Do’s and Don’ts in advanced dementia and end-of-life care (Choosing Wisely) • Don’t leave an implantable cardioverterdefibrillator (ICD) activated when it is inconsistent with the patient/family goals of care (HPM). • Don’t routinely prescribe lipid-lowering medications in individuals with a limited life expectancy (AMDA). • Don’t recommend aggressive or hospital-level care for a frail elder without a clear understanding of the individual’s goals of care and the possible benefits and burdens (AMDA). Thank you