Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
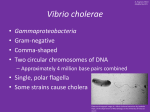
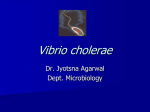
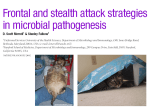
MICROBIOLOGY LEC | VIBRIOS, CAMPYLOBACTERS, HELICOBACTER and ASSOCIATED BACTERIA Tutor: DR. ZARA | Lecture Date: DEC 8, 2020 | 1ST SEM TOPIC OUTLINE I. VIBRIOS i. V. cholerae Morphology and Identification Antigenic structure and Biologic function Pathogenesis and Pathology Signs and Symptoms Diagnostic Laboratory Tests Immunology Treatment Prevention, and Control ii. V. parahemolyticus Very Actively motile by means of a polar flagellum Non-acid fast, non-spore, non-encapsulated Pleomorphic iii. V. vulnificus II. AEROMONAS i. A. hydrophila III. PLEISOMONAS IV. CAMPYLOBACTER i. Campylobacter jejuni ii. Campylobacter coli V. Helicobacter pylori Vibrio, Aeromonas, Campylobacter, and Helicobacter are Gram-negative rods that are all widely distributed in nature. Vibrio cholerae produces an enterotoxin that causes cholera, a profuse watery diarrhea that can rapidly lead to dehydration and death. Campylobacter jejuni is a common cause of enteritis in humans. Helicobacter pylori is associated with gastritis and duodenal ulcer disease. I. VIBRIOS Vibrios are among the most common bacteria in marine and estuarine waters, worldwide. Comma-shaped, curved and sometimes facultatively anaerobic, fermentive rods Catalase and oxidase positive Motile: monotrichous or multitrichous polar flagella Can grow at 14 to 40 degree centigrade All species require sodium chloride for growth (Halophilic: “salt loving”) i. VIBRIO CHOLERAE MORPHOLOGY AND IDENTIFICATION A. Typical Organisms Comma-shaped, curved rod 2-4 um long Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO B. Culture Produces convex, smooth, round colonies that are opaque and granular (very small) in transmitted light. Grow well at 37°c on many kinds of media (like EMB, MAC) Grows well on thiosulfate-citrate-bilesucrose (TCBS) agar (very selective media) produces yellow colonies (sucrose fermented) that are readily visible against the dark-green background of the agar. Unlike Enterobacteriaciae (E.coli and Klebsiella) that ferments lactose: in TSI it turns yellow and in MAC agar turns pink Non-sucrose-fermenting vibrios (e.g., most strains of V. parahaemolyticus and V. vulnificus) produce green colonies on TCBS agar. Oxidase positive, which differentiates them from enteric gram-negative bacteria. (This will automatically rule out E.coli or Klebsiella) Oxidase Test Positive – when the paper turns violet : meaning they are Aerobic ALKALOPHILES - Grow at a very high pH (8.5– 9.5 average of 9) and are rapidly killed by acid. P a g e 1 | 16 To ensure optimal recovery of vibrios, stool specimens should be collected early on the course of the diarrheal illness. If processing is delayed- mixed specimen in a Cary-Blair transport medium and refrigerate. When ingesting contaminated water, the concentration of the inoculum should be high for it to elicit diarrhea (10 2 does not cause diarrhea; should be higher in concentration) **In areas where cholera is endemic, direct cultures of stool on selective media, such as TCBS, and enrichment cultures in alkaline peptone water are appropriate. However, routine stool cultures on special media such as TCBS generally are not necessary or cost effective in areas where cholera is rare. C. Growth Characteristics Susceptible to the compound O/129 (2, 4diamino-6,7-disopropylpteridine phosphate) which differentiates them from Aeromonas species, which are resistant to O/129. Halotolerant (Salt-loving organisms)and NaCl (<0.5 to 4.5%) often stimulates their growth. Another difference between vibrios and aeromonads is that vibrios grow on media containing 6% NaCl, but Aeromonas does not. Another difference between vibrios and aeromonads is that vibrios grow on media containing 6% NaCl, but Aeromonas does not. Ferments sucrose (turn it to yellow with green background) and mannose but not arabinose. Facultative anaerobe Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO Halotolerance is the adaptation of living organisms to conditions of high salinity. Halotolerant species tend to live in areas such as hypersaline lakes, coastal ... Colonies of V. cholerae growing on thiosulfate, citrate, bile salts, and sucrose agar. The glistening yellow colonies are 2–3 mm in diameter and are surrounded by a diffuse yellowing of the indicator in the agar up to 1 cm in diameter. The plate is 10 cm in diameter. ANTIGENIC STRUCTURE AND BIOLOGIC CLASSIFICATION Share a single heat-labile flagellar H antigen. Antibodies to the H antigen are probably not involved in the protection of susceptible hosts. (It means even if you develop antibody against H antigen it doesn’t mean you are Immune to vibrio cholera) Has O LPS Confer serologic specificity. V. Cholerae strains sero groups 01 and O139 (Bengal strain) cause (epidemic and pandemic) cholera in humans while other vibrio may cause sepsis or enteritis. Antibodies to the O antigens tend to protect laboratory animals against infections with V cholerae. Occasionally, non-O1/non-O139 V cholerae causes cholera-like disease. P a g e 2 | 16 Activation of subunit A1 yields increased levels of cAMP and results in prolonged hypersecretion of water and electrolytes. There is increased sodium-dependent chloride secretion, and absorption of sodium and chloride by the microvilli is inhibited. Electrolyte-rich diarrhea occurs with as much as 20-30L/day, resulting in dehydration, shock, acidosis and death. Two biotypes of epidemic have been defined Classic El Tor. El Tor biotype: - produces a hemolysin - gives positive results on the VogesProskauer test and sensitive to Polymixin B – – – – – V cholerae O139 is very similar to V cholerae O1 El Tor biotype. V cholerae O139 does not produce the O1 LPS and does not have all the genes necessary to make this antigen. V cholerae O139 makes a PS capsule like other non-O1 V cholerae strains, but V cholerae O1 does not make a capsule. The V. cholerae Serogroup O1 antigen has determinants that make possible further subtyping; these serotypes are Ogawa, Inaba and Hikojima. Furthermore, two biotypes of epidemic V. cholerae have been defined, classic and El Tor. The El Tor biotype produces a hemolysin, gives positive results on the VogesProskauer test and is resistant to polymyxin B. Typing is used for epidemiologic studies. Vibrio cholera enterotoxin Produce a heat-labile enterotoxin, consisting of subunits A. Ganglioside GM1 (receptors located in the GIT) serves as the mucosal receptor for subunit B, which promotes entry of subunit A into the cell. Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO - - When you ingest a contaminated water, the cholera toxin which is made up of Subunit A and B, the Subunit B will be the one to bind to the GM1 Ganglioside receptor. Once the subunit B binds to the GM1 receptor, the subunit A detaches ( yung color BLUE mahihiway kay GREEN- Subunit B) hence the Subunit A will enter the Cytoplasm where it binds to G protein that will then activate binding to Adenylate cyclase. This adenylate cyclase will stimulate the increased production of cAMP now opening the Cystic Fibrosis Transmembrane receptor so mag o-open, mabubutas yung epithelial tissue: THE GATE IS OPEN hence you will excrete a lot of Na then water, and a lot of electrolytes as well. How much can you lose? – you can have a diarrhea that is 20 – 30 L a day which is di mo mapigilan P a g e 3 | 16 The genes for V cholerae enterotoxin are on the bacterial chromosome. Cholera enterotoxin is antigenically related to LT of Escherichia coli and can stimulate the production of neutralizing antibodies. However, the precise role of antitoxic and antibacterial antibodies in protection against cholera is not clear. PATHOGENESIS AND PATHOLOGY Pathogenic only for humans. Infectivity: A person with normal gastric acidity may have to ingest as many as 1010 or more V. cholerae Vehicle is water When the vehicle is food, as few as 10 2–104 This is also the infectious does in a person with achlorhydria or hypochlorhydria. Organisms are necessary because of the buffering capacity of food. V. cholerae is a noninvasive mucosal pathogen, therefore, they do not reach the bloodstream (does not cause bacteremia) but remain within the intestinal tract. Virulent V. cholerae organisms attach to the microvilli of the brush border of epithelial cells. There they multiply and liberate cholera toxin and perhaps mucinases and endotoxin. Any medication or condition that decreases stomach acidity makes a person more susceptible to infection with V cholera. SIGNS AND SYMPTOMS The spectrum of disease due to V. cholerae ranges from asymptomatic intestinal colonization to mild, moderate, or severe diarrhea. About 50% of infections with classic V. cholerae are asymptomatic, as are about 75% of infections with the El Tor biotype. The incubation period after ingestion of a sufficiently high infectious dose of V. cholerae is 12 hours to 3 days for persons who develop symptoms, depending largely on the size of the inoculum ingested. Profuse diarrhea sometimes called “rice water stools” - contain mucus, epithelial cells, and large numbers of vibrios. (Commonly asked in board exams: Rice Water Stool is Very typical of V. cholerae) Sudden onset of nausea and vomiting Abdominal pain Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO Leg cramps (because you lose a lot of electrolyte particularly your Potassium) Sunken eyes ( because of severe dehydration) SHOCK – because of severe fluid losses Hypovolemic Shock - Low blood pressure DIAGNOSTIC LABORATORY TESTS A. Specimens Mucus flecks from stools - Collected early in the course of the diarrheal illnessand inoculated within 2-4 hours of collection B. Smears Not distinctive Dark-field or phase contrast microscopy Show the rapidly motile vibrios (because of their polar flagella) C. Culture TCBS agar pH near 9 - Alkalophile 18 hours P a g e 4 | 16 Growth is rapid in alkaline peptone broth or water, containing NaCl with a ph of 8.5 or on TCBS. D. Specific Tests Slide agglutination tests using anti-O group 1 or group 139 antisera (results in Agglutination – Positive result) Immunochromatographic dipstick test IMMUNITY Gastric acid An attack of cholera is followed by immunity to reinfection, but the duration and degree of immunity are not known TREATMENT Fluids and electrolytes-most important part of treating cholera patients to correct the severe dehydration and salt depletion (because what kills the px is not the toxin but severe dehydration) Antimicrobial agents are effective against V. cholerae, but these play a secondary role in px management. Appropriate antimicrobial therapy can also reduce the duration and amount of shedding og Vibrio organism in the stool. Oral tetracycline and doxycycline Resistance: carried by transmissible plasmids. In children and pregnant women, alternatives to the tetracycline (cannot give to children; also causes yellow discoloration of teeth) include erythromycin (because we cannot give Doxycycline to pregnant women because of its teratogenic effect) and furazolidine Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO EPIDEMIOLOGY, PREVENTION AND CONTROL Most likely by V. cholerae O1 of the classic biotype and largely originating in Asia, usually the Indian subcontinent. Cholera is endemic in India and Southeast Asia. Vibrios survive in water for up to 3 weeks Cholera is a disease that is spread by contact involving individuals with mild or early illness by water, food, and flies. V. cholerae lives in aquatic environments. Lives attached to algae, copepods, and crustacean shells. It can survive for years and grow, but when conditions are not suitable for growth, it can become dormant (they’re still present but they don’t replicate) Control rests on education and on improvement of sanitation, particularly of food and water. Patients should be isolated, their excreta disinfected, and contacts followed up. Chemoprophylaxis with antimicrobial drugs may have a place. Repeated injection of a vaccine containing either lipopolysaccharides extracted from vibrios or dense Vibrio suspensions can confer limited protection to heavily exposed persons (eg, family contacts) but is not effective as an epidemic control measure. ii. VIBRIO PARAHEMOLYTICUS Halophilic Causes acute gastroenteritis after ingestion of Contaminated seafood such as raw fish or shellfish. IP: 12–24 hours, nausea and vomiting, abdominal cramps, fever, and watery to bloody diarrhea occur (due to its characteristic invasiveness) - Fecal leukocytes No enterotoxin Facultative anaerobe Does not grow well on some of the differential media used to grow Salmonellae and Shigellae, but it does grow well on blood agar. Grows well on TCBS, where it yields green colonies (does not ferment sucrose). The final organism identification is achieved by the use of various standard biochemical tests. Usually no specific treatment other than rehydration is required since the gastroenteritis P a g e 5 | 16 is self-limited. However, antimicrobial therapy could be considered for patients in whom the diarrheal illness does not resolve within 5 days; doxycycline and/or fluoroquinolones are appropriate choice for antibiotic therapy and would shorten the duration of the illness. V. Parahaemolyticus is usually oxidase-positive Spontaneously resolved in 1–4 days with no treatment other than restoration of water and electrolyte balance. iii. Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO VIBRIO VULNIFICUS Severe wound infections, bacteremia, and probably gastroenteritis. is a free-living bacterium and part of the normal marine microbiota in association with bivalves and crustaceans Oysters (commonly asked in board exams) and shellfish Alcoholism or liver disease. Wounds may become infected in normal or ICH Bullous skin lesions, cellulitis, and myositis with necrosis. TCBS Teracycline; Ciprofloxacin Wound infections may be mild but often proceed rapidly (over a few hours), with development of bullous skin lesions, cellulitis, and myositis with necrosis The two most common clinical presentations of V. vulnificus infection are rapidly progressive wound infections due to skin/soft tissue injuries following exposure to contaminated seawater and primary bacteremia/sepsis following the consumption of contaminated raw oysters. V. vulnificus can invade the bloodstream without causing gastrointestinal symptoms P a g e 6 | 16 Vibrio spp. ( Family Vibrionaceae) Associated with Human Disease i. Aeromonas hydrophila II. AEROMONAS Ubiquitous inhabitants of fresh and brackish water Aeromonads are Gram-negative, facultative anaerobic rods that ferment carbohydrates and may resemble morphologically members of the family of Enterobacteriaceae 1–4 μm long and are motile. Colony morphology large zones of hemolysis (bhemolytic) on blood agar. Cultured from stool (+) oxidase reaction Aeromonas species are differentiated from vibrios by showing resistance to the compound O/129 and lack of growth on media containing 6% NaCl. (Most differentiating characteristics – please remember) Most common spp of Aeromonas Predominantly Not associated with diarrhea Contaminated Fresh water Swelling of Lower Extremities (yung dinaanan ng tubig – Exposed Extremities) Releases cytotoxin (in the cytoplasm) and Hemolysins that hemolyzes RBC Wound infections from trauma that occurs in a water environment and are caused primarily by a hydrophila. Most commonly associated with human infection: A. hydrophila, A. caviae, A. veronii. Tetracyclines, aminoglycosides, and thirdgeneration cephalosporins (Ceftriaxone). Aeromonas species are also associated with extraintestinal infections such as bacteremia and wound infections Most commonly, uncomplicated cellulitis develops within 48 hours of the injury, but systemic symptoms may also develop. In addition to antimicrobial therapy, the suppurative necrosis surrounding the wound may require surgical debridement Produce hemolysins. Cytotoxins Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO P a g e 7 | 16 III. Plesiomonas shigelloides is an oxidase (+) It is a water and soil organism and has been isolated from freshwater fish and many animals. Plesiomonas grows on the differential media used to isolate Salmonella and Shigella from stool specimens Cross-reactions with Shigella antisera occur. Plesiomonas can be distinguished from shigellae in diarrheal stools by the oxidase test: o Plesiomonas is oxidase positive, and shigellae are not. Positive for dnase Most isolates from humans have been from stool cultures of patients with diarrhea IV. PLESIOMONAS CAMPYLOBACTER JEJUNI & CAMPYLOBACTER COLI C. jejuni and C. coli have emerged as common human pathogens Causes: o Enteritis o Occasionally systemic infection i. CAMPYLOBACTER Cause both diarrheal and systemic diseases H. pylori – Causes gastric infection C. jejuni – Prototype organism in the group and is a very common cause of diarrhea in humans. Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO MORPHOLOGY AND IDENTIFICATION A. Typical Organisms C. jejuni and the other campylobacters are gram (-) rods with comma, S, or “gull wing” shapes. Motile, with a single polar flagellum, and do not form spores B. Culture Selective media – blood free, charcoal-based selective medium agar (CSM) for isolation of C. jejuni Incubation must be in an atmosphere with reduced O2 (5% O2) with added CO2 (10% CO2) Incubation at 42°C Although C. jejuni grows well at 36 to 37°C, incubation at 42°C prevents growth of most of the other bacteria present in feces, thus simplifying the identification of C. jejuni. Skirrow’s medium contains: o Vancomycin o Polymyxin o Trimethoprim to inhibit growth of other bacteria o Colonies tend to be colorless or gray, watery and spreading or round and convex and bot colony types may appear on one agar plate. o May be less sensitive than other commercial products that contain charcoal, other inhibitory compounds and cephalosporin antibiotics. P a g e 8 | 16 a. No change with alpha-napthylamine and sulfanilic acid means nitrite absent. b. Turns red with alpha-napthylamine and sulfanilic acid means nitrite present, positive nitrate reduction test c. No change with zinc means positive nitrate reduction test d. Turns red with zinc means negative nitrate reduction test C. Characteristics C. jejuni and the other campylobacters pathogenic for humans are oxidase and catalase (+). Do NOT ferment carbohydrates. Nitrate reduction, hydrogen sulfide production, hippurate tests, and antimicrobial susceptibilities can be used for further identification of species. NITRATE REDUCTION Inoculate with loop Incubate Additional solutions o Sulfanilic acid (A) o Naphthylamine (B) (+) = Red o Nitrate to nitrite No color, add Zinc o (+) = Not red o (-) = Red Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO ANTIGENIC STRUCTURE and TOXINS When you ingested contaminated poultry products o LPS with endotoxic activity. o Cytopathic extracellular toxins and enterotoxins PATHOGENESIS and PATHOLOGY Oral route Poultry products C. jejuni is susceptible to gastric acid 104 Infection Multiply in the small intestine Invade the epithelium and produce inflammation Appearance of red and white blood cells in the stools. Bloodstream is invaded and a clinical picture of enteric fever develops. Localized tissue invasion coupled with the toxic activity appears to be responsible for the enteritis. P a g e 9 | 16 Campylobacter fetus subspecies venerealis is a rare cause of human disease. CLINICAL FINDINGS Most affected are immunocompromised host especially HIV positive patients. Acute onset of crampy abdominal pain because of toxins, profuse diarrhea that may be grossly bloody since it is invasive, headache, malaise and fever. Self-limited means not necessary to treat with antibiotics to a period of 5 to 8 days if you are immunocompetent means no DM and kidney disease just ingested contaminated poultry products. But if you are immunocompromised treat with antibiotics, you can give your tetracycline or ciprofloxacin. Erythromycin and therapy shortens the duration of fecal shedding of bacteria. Certain serotypes of C. jejuni have been associated with postdiarrheal Guillain-Barré syndrome - is an ascending muscle paralysis, paralyzes first your lower extremities and ascends to your diaphragm, which leads to difficulty in breathing. Then the patient is place in ICU with mechanical ventilator. Reactive arthritis - joint pain and Reiter’s syndrome may also follow acute campylobacter diarrhea. ii. Campylobacter fetus Opportunistic pathogen that causes systemic infections in immunocompromised patients. Oral route (POE) Causes bacteremia and systemic infection. Capsule-like structure on the surface of the organism. V. Helicobacter pylori This bacterium is a common question in revalida! MORPHOLOGY and IDENTIFICATION A. Typical Organisms Has multiple flagella at one pole and is actively motile. (unlike Vibrio in which there is only one flagella on its pole) B. Culture Grows well in 3–6 days when incubated at 37°C in a microaerophilic environment, as for C jejuni. (Most of them are incubated at 37 to 42°C) The media for primary isolation include Skirrow’s medium (same with Campylobacter) with vancomycin polymyxin B, and trimethoprim (these are the antibiotics contained in the Skirrow’s, which inhibit the growth of gram-positive organisms), chocolate medium, and other selective media with antibiotics (e.g., vancomycin, nalidixic acid, amphotericin). The colonies are translucent and 1–2 mm in diameter. (Larger colonies (mm) than Vibrio which are micrometer in size) C. Growth Characteristics Oxidase positive and catalase positive. Motile, and is a strong producer of urease (an enzyme that converts Urea into Ammonia and CO2 creating a positive color PINK). (Urease positive is a very typical characteristic of Helicobacter; and this is the one commonly asked in the revalida) PATHOGENESIS and PATHOLOGY Compared with the polysaccharide capsules of pathogens such as Neisseria meningitidis and Streptococcus pneumoniae). In a mouse model of C. fetus infection, the presence of the S protein as a surface capsule correlated with the ability of the bacteria to cause bacteremia after oral challenge and cause death in a high percentage of the animals. Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO H. pylori is the most common organism that causes duodenal ulcer & gastric ulcer. H. pylori also produces a protease that modifies the gastric mucus and further reduces the ability of acid to diffuse through the mucus. H. pylori produces potent urease activity, which yields production of ammonia and further buffering of acid. P a g e 10 | 16 H. pylori is quite motile, even in mucus, and is able to find its way to the epithelial surface. H. pylori overlies gastric-type but not intestinal-type epithelial cells. Toxins and lipopolysaccharide may damage the mucosal cells, and the ammonia produced by the urease activity may directly damage the cells. In Acute H. pylori infection, the patient will experience abdominal pain if left untreated; it will lead to chronic H. pylori infection Chronic H. pylori infection will lead to three complications (1) Antral predominant gastritis, (2) Nonatrophic pangastritis, (3) Corpus-Predominant Atrophic Gastritis (CPAG) Once H. pylori enters the host it will invade the GIT it will release urease (survival) Ammonia production which further buffer the acid pH becomes less acidic which in turn signal your parietal cells to secrete more acid ulcer In CPAG, corpus part of the stomach will undergo atrophy then it will lead to Intestinal metaplasia (change of lining epithelium) then Dysplasia Gastric cancer The Chronic H. pylori complication that leads to duodenal ulcer is the Antral Predominant Gastritis. CLINICAL FINDINGS It also has flagella (motility) travels to intestinal epithelial cells it will adhere to the cells from where it attaches it releases also toxins (damage the host) they go to epithelial cell cytoplasm intracellular replication while undergoing replication they will try to destroy the mucosa and they create crater/ ulcer Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO Acute infection: Upper gastrointestinal illness with nausea and pain, vomiting and fever may also be present. The acute symptoms may last for less than 1 week or as long as 2 weeks. After colonization, the H pylori infection persists for years and perhaps decades or even a lifetime. About 90% of patients with duodenal ulcers and 50– 80% of those with gastric ulcers have H pylori infection. P a g e 11 | 16 [So if you are asked which one is more common ulcer (by H. pylori) the answer is DUODENAL ULCER (90%)] Before you get to be diagnosed with Ulcer, you have to undergo Endoscopy Endoscope inserted to your mouth going down to your GIT and they will try to visualize (through video) if there’s ulcer in your stomach or duodenum (Endoscopy or gastroscopy) if there’s ulcer, the Doctor will take a tissue sample from that ulcer Tissue sample will be examined by the Pathologist (biopsy) and if there’s dysplastic or malignant changes seen you will be diagnosed with gastric cancer. G. Diagnosis urea breath tests DIAGNOSTIC LABORATORY TESTS A. Specimens Gastric Biopsy o Stool samples may be collected for H. pylori antigen detection. B. Smears o A gastroscopy procedure with biopsy is required. o Spiral-shaped organisms. C. Culture D. Antibodies o The serum antibodies persist even if the H. pylori infection is eradicated, and the role of antibody tests in diagnosing active infection or after therapy is therefore limited. The presence of H. pylori will result in an increase in the ratio of 13CO2 to 12CO2 in expired breath. (Breath smells like urine). E. Rapid tests to detect urease activity. F. Gastric biopsy with a color indicator. o If H pylori is present, the urease rapidly splits the urea (1–2 hours), and the resulting shift in pH yields a color change in the medium. In vivo tests for urease activity can be done also. CLOtest (Positive= RED by Urease) Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO P a g e 12 | 16 SAMPLEX Identification: 1. Responsible for the motility of V. cholerae. 2. It is the adaptation of living organisms to conditions of high salinity. 3. 2 strains of V. cholerae that causes cholera in humans. 4. Toxins released by A. hydrophila. 5. Identify the shape of C. jejuni in gram staining. 6. Identify the selective medium for C. jejuni. 7. Identification. What is the motility of Campylobacter jejuni? 8. Identification. Best specimen for H. pylori 9. What is the appearance of Vibrio on TBCS media? True or False 1. Antibodies to the H antigen are highly involved in the protection of susceptible hosts against V. cholerae toxin. 2. V. paraheolyticus grows well on TCBS, where it yields yellow colonies. 3. Even a 102 concentration of V. cholerae can induce diarrhea. 4. Plesiomonas can be distinguished from shigellae in diarrheal stools by the oxidase test with a positive result. 5. Campylobacter jejuni atmosphere and temp is, microaerophilic and 42°C 6. Campylobacters can form spores as part of their virulence factor. 7. Gastric ulcer is the most common ulcer found in patients with H. pylori infection. 8. Serum antibodies do not persist if the H. pylori infection is eradicated. Multiple choice 1. Among the three complications of Chronic H. pylori infection, which one will lead to duodenal ulcer? a. Corpus-predominant atrophic gastritis b. Nonatrophic pangastritis c. Antral predominant gastritis 2. Which of the following means positive in H. pylori? (Choose the correct answer/s) Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO a. Color yellow in CLOtest b. Increase in the ratio of 13CO2 to 12CO2 in expired breath c. Dysplastic cells seen during biopsy d. Pink reaction in Urease Test 3. An enzyme produced by the H. pylori, which modifies the gastric mucus and further reduces the ability of acid to diffuse through mucus. a. Urease b. Nuclease c. Protease d. Pepsin 4. What antibiotics are used in the primary isolation of H. pylori, which inhibit the growth of gram-positive organisms? a. Vancomycin polymyxin B b. Trimethoprim c. Clarithromycin d. A and B e. A and C 5. Which of the following/s is/are true about H. pylori? a. It has flagellum at one pole and is actively motile b. Grows well in 3-6days when incubated at 39°C in microaerophilic environment c. Oxidase positive and catalase negative d. Colonies are translucent and 1-2mm in diameter e. All of the above are true 6. Which of the following statement/s is/are true about the clinical findings of H. pylori infection? a. Acute illness includes nonspecific symptoms such as nausea and vomiting, abdominal pain and sometimes fever b. Acute symptoms may last for less than 1 week or as long as 4 weeks. c. About 90% of the patient with gastric ulcers have H. pylori infection d. H. pylori is not considered as a risk factor for the development of gastric carcinoma e. None of the above are true P a g e 13 | 16 7. A stool specimen from 5 years old child is cultured in selective media having high pH concentration. After the incubation, colonies appear smooth and round and identified as a comma-shaped, gram-negative, motile bacteria. Name the bacteria isolated? a. Aeromonas spp b. Pseudomonas aeruginosa c. Streptococcus pyogenes d. Vibrio cholerae 8. Vibrio cholerae causes Cholera and mostly occurs in developing countries, symptoms include diarrhea and vomiting within 2-3 days after the ingestion of contaminated water or food. Name the type of diarrhea caused by V. cholerae? a. Acute watery diarrhea with blood b. Acute watery diarrhea resembling rice water c. Mild watery diarrhea resembling rice water d. Acute watery diarrhea with no blood 9. What is the most common food that causes foodborne gastro-enteritis by Vibrio parahaemolyticus? a. Chicken b. Fish c. Oysters d. Rice 10. Which of the following statements is/are not correct about Aeromonas spp and Plesiomonas spp? a. Both are oxidase positive b. They can be found in freshwater and soil c. They are gram-negative rods d. Grow well on TCBS. 11. Campylobacter jejuni is one of the most common causes of food poisoning, which also has been associated with post diarrheal syndrome, the syndrome is called ________? a. Toxic shock syndrome b. Guillain-Barre syndrome c. Short bowel syndrome Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO d. Rett syndrome 12. Campylobacter jejuni is a microaerophilic bacterium, which of the following statement is true for the culture of this bacterium. a. An atmosphere increased O2 (10%) with added CO2 (5%) b. An atmosphere of reduced O2 (5%) with added CO2 (10%) c. An atmosphere of reduced CO2 (5%) with added CO2 (10%) d. An atmosphere of increased CO2 (10%) with added O2 (5%) 13. What is/are not the growth characteristics of Campylobacter spp? Select from all the options given below. a. Oxidase and catalase positive b. Produce H2S c. Ferment carbohydrates d. Have darting motility 14. Helicobacter pylori is associated with all of the following, EXCEPT? a. Malt lymphoma b. Gastric carcinoma c. Peptic ulcer d. Burkitt’s lymphoma 15. Which one of the following virulence factors may be associated with the pathogenesis of infection caused by Helicobacter pylori? a. Flagella b. Lipopolysaccharide c. Exotoxins d. Endotoxins 16. Which one of these is not the common laboratory tests for the identification of Helicobacter pylori? a. Biopsy test b. Urease breath test c. Stool antigen test d. Urine test 17. Which of the following biotypes of Vibrio cholerae is prevalent in developing countries? a. EL Tor P a g e 14 | 16 b. Classic c. Biotype O139 d. Biotype O1 18. Aeromonas hydrophila mostly causes infections to fish and amphibians and less pathogenic to humans, one of the most common infection in human is gastroenteritis. What is the other common human disease caused by bacteria? a. Peptic ulcer b. Cellulitis c. Asthma d. Gastritis 19. Helicobacter pylori infection is most prevalent in developing countries, in what age people the chances of infection is the highest? a. 10 to 30 b. 30 to 50 c. 60 and above d. Infant 20. Vibrio vulnificus and V. parahaemolyticus both gram-negative, motile bacteria are mostly found in warm coastal areas. What is/are the common source through which these bacteria can be transferred to human and cause infections? a. Water b. Oysters c. Shellfish d. All of the above 21. ________ is less likely to cause gastroenteritis or diarrheal disease in humans. a. Vibrio spp b. Salmonella spp c. Plesiomonas spp d. Campylobacter spp b. A medium containing vancomycin, polymyxin B, and trimethoprim incubated at 42°C. c. MacConkey agar medium incubated at 37°C. d. Thiosulfate-citrate-bile-sucrose medium incubated at 42°C. 23. The V. cholerae factor responsible for diarrhea is a toxin that a. Blocks EF-2 b. Yields increased intracellular levels of cAMP c. Cleaves SNARE d. Blocks EF-1-dependent binding of amino-acyl-tRNA to ribosomes 24. A patient presents to the emergency department with non-bloody diarrhea for 12 hours. The patient lives in Washington, DC, and has not recently traveled out of the area. Which one of the following is unlikely to be the cause of your patient’s diarrhea? a. Aeromonas spp b. C. jejuni c. H. pylori d. V. cholera 25. This BIOTYPE that produces a hemolysin gives positive results on the Voges-Proskauer test and sensitive to Polymixin B a. El Tor b. Classic c. Inaba d. Ogawa 22. A 45-year-old man develops a gastric ulcer that can be visualized on a contrast mediumenhanced radiograph of his stomach. A biopsy specimen is taken from the gastric mucosa at the site of the ulcer. A presumptive diagnosis can be reached most rapidly by inoculating part of the specimen on which of the following? a. A medium used to detect urease incubated at 37°C. Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO P a g e 15 | 16 Answers: Identification 1. Polar flagella 2. Halotolerance 3. V. Cholerae strains sero groups 01 and O139 (Bengal strain) 4. Cytotoxin and hemolysin 5. Comma/ S/ Gull Wing shape, Small curved rods 6. Skirrow’s Medium 7. Darting motility 8. Breath and stool 9. V. cholerae appears yellow (ferment sucrose), other spp are blue-green (non-sucrose fermenters) 21. 22. 23. 24. C A B D True or false 1. 2. 3. 4. 5. 6. 7. 8. False – not really involved False – green colonies False – needs large concentration True True False False False Multiple choice 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. C B, C, D C D D A D B C D B B C D D D A B C D Trans 10| GALISTE | GAOYEN | IBARRA | LAMORIN | LAYDA|LESCAIN |MANZANO | NGALNGALO P a g e 16 | 16