Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
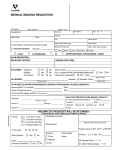
THIS DOCUMENT MUST BE COMPLETED BY A PHYSICIAN (must not be completed by patient) DIAGNOSTIC IMAGING: ULTRASOUND RADIOLOGY BONE MINERAL DENSITY Ordering Physician Name OUTPATIENT SERVICES (Please Print) Name: Ordering Physician Signature QHC-BG 265 Dundas St. E Belleville, ON K8N 5A9 QHC-TM 242 King St Trenton, ON K8V 5S6 QHC-PECM 403 Main St. E Picton, ON K0K 2T0 QHC-NH 1-H Manor Lane Bancroft, ON K0L 1C0 DOB: HCN: Phone #: Address: Copy to: Pregnant: Yes No LMP: ER patient in EMERG ER patient sent Home Routine Stat Urgent PLEASE BRING THIS REQUISITION AND YOUR HEALTHCARD PATIENTS PRESENTING UNSIGNED/INCOMPLETE REQUISITIONS WILL BE RE-BOOKED APPOINTMENTS MUST BE MADE THROUGH CENTRAL BOOKING AT 613-969-7400 EXT. 2494 OR EXT. 2949 IF CALLING FROM BANCROFT AREA CALL 613-332-2825 EXT. 2494 OR EXT. 2949 Clinical Indication/History: XRAY ULTRASOUND Appointment Date & Time: QHC Site: BG TM PECM NH Lower Extremities Chest Upper Extremities Pelvis Chest A.C. Joints L S.I. Joints R R Sternum L Clavicle L Hips R R L Shoulder Thoracic Inlet L Femur R L Ribs R R L Scapula R L Knee R L SC Joints R L Humerus L Tib & Fib R R L Elbow Appointment Date & Time: QHC Site: BG TM PECM NH Carotids (PVD) Peripheral arterial area of interest: _____________ (DVT) Peripheral venous area of interest: ____________ Chest Wall Mass Pleural Effusion Abdomen Kidney, Ureters & Bladder (KUB) Pelvis (Female) Transvaginal Pelvis (Male) TRUS BX: Must be referred by a Urologist Testes/Scrotum Thyroid Obstetrical ≤ 15 wks >16 wks Biophysical Profile Medically Warranted Musculoskeletal Shoulder Superficial Mass L Ankle R L Foot L Os Calcis Toes L 12345 G.I. Tract Ba Swallow R R Abdomen Plain film (KUB) Acute (3 Views) L Forearm R L L R R Head and Neck Skull Wrist Hand Fingers T2345 Spine Cervical Upper G.I. Series Sinuses Thoracic Small Bowel Lumbar Barium Enema Soft tissue Neck Facial bones Scoliosis Orbits R Mandible Other: ___________________________________ ___________________________________ ___________________________________ L Sacrum & Coccyx Skeletal Survey Bone Age Arthritic Metastatic BONE MINERAL DENSITY Appointment Date & Time: QHC Site: BG Routine High Risk QHC # 408 Rev: May 2011 R TM Height: Weight: Area of Interest: __________________ Other: TECHNOLOGIST NOTES: THIS DOCUMENT MUST BE COMPLETED BY A PHYSICIAN (must not be completed by patient) Bring your requisition & Health Card to your appointment. Arrive 30 minutes prior to appointment for registration. If unable to keep appointment, please give 24 hours notification. All QHC hospitals are designated as a reduced scent environment. We do not provide child care, please leave young children at home DIAGNOSTIC IMAGING INSTRUCTION SHEET DIABETICS: Please inform us at the time of booking so that an early appointment can be arranged. If having an injection of a contrast medium (x-ray dye), Metformin HCL (Glucophage) must be stopped on the day of the exam, and for an additional 48 hours after contrast injection. Normal renal function must be confirmed prior to restarting this medication. If urine output decreases, contact your doctor. FEMALE PATIENTS: If there is a possibility that you are Pregnant, please inform your doctor and the technologist. If possible, book your appointment within ten (10) days following the onset of menstruation, since the risk of pregnancy is small during this period. X-RAY UPPER GI SERIES, SMALL BOWEL STUDIES, and ESOPHAGUS: Do not eat or drink after midnight on the night before your test. Bring your morning oral medications with you and take them after your test. Do not smoke or chew gum on the day of the test. Expect small bowel studies to take a minimum of two hours. BARIUM ENEMA, IVP (INTRAVENOUS PYELOGRAM): Purchase one (1) box of Pico-Salax and four (4) Bisacodyl tablets from a pharmacy. The day before your test, remain on a clear fluid diet (clear “pulp-free” fruit juice, plain jello, clear soup such as consommé, bouillon, tea, coffee…no milk). At 1:00 p.m., take 4 Bisacodyl tablets. Drink lots of clear fluids. At about 4:00 p.m. take the first packet of Pico-Salax (prepare as the package indicates). Drink a large glass of water every hour. At about 8:00 p.m. take the second packet of Pico-Salax. Do not eat or drink after midnight. BONE MINERAL DENSITY Do not take any calcium supplements day of exam. Appointment should not be booked within 2 weeks of having any X-ray exams involving contrast agents or having had a nuclear medicine appointment. Dress comfortably, wear loose fitting clothes ULTRASOUND ABDOMINAL ULTRASOUND: Do not eat or drink anything for 6 hours prior to the examination. Do not chew gum the day of your test. ABDOMINAL/PELVIC ULTRASOUND: Do not eat for 6 hours prior to the examination. . Do not chew gum the day of your test. Finish drinking 1 Litre of fluid 1 hour before your examination time. Do not empty your bladder. PELVIC ULTRASOUND: Finish drinking 1 Litre of clear fluid 1 hour before examination time. Do not empty your bladder. A Transvaginal study may also be requested which involves the insertion of the ultrasound probe into the vagina for optimal visualization of the pelvic structures. The bladder will be emptied for this portion of the examination. OBSTETRICAL (PREGNANCY) ULTRASOUND: Before 20 weeks (4 ½ months)—follow the instructions for the Pelvic Ultrasound above. After 20 weeks (4 ½ months)—Do not drink fluids, but do not empty your bladder 1 hour before examination time. KIDNEY/BLADDER ULTRASOUND: Finish drinking 1 Litre of clear fluid 1 hour before examination time. Do not empty your bladder. TRUS BIOPSY: Stop taking aspirin 1 week prior to procedure. Discuss stopping any other blood thinners with your physician. An antibiotic must be prescribed prior to your procedure. LIVER BIOPSY: Light breakfast morning of procedure. Discontinue taking aspirin &/or arthritic antiinflammatory medications 4 to 5 days prior to the procedure (Tylenol is acceptable) Discuss stopping any other blood thinners with your physician.