Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
VOL 12, NO. 3, 1986
Information-Processing
Abnormalities:
Trait- and State-Dependent
Components
by Dennis P. Saccuzzo
and David L. Braff
Abstract
Schizophrenics were compared to
schizoaffective, bipolar, and nonpsychotic depressed patients in a visual
masking paradigm in which an informational target stimulus was
followed at varying intervals by a
noninformational masking stimulus.
In limiting the availability of the
sensory signal provided by the target
stimulus, the mask was used to probe
how information from the environment enters and is processed by the
central nervous system. The use of
the masking paradigm was originally
based on the hypothesis that thought
disorder is a result of a more primary
dysfunction in the processes that
precede and result in thought. Results
confirmed previous findings of a
performance deficit in the schizophrenics when compared to nonpsychotic controls. Schizoaffective and
bipolar patients also showed evidence
of impaired processing, however.
Results were interpreted in terms of a
trait/state formulation in which
impaired information processing is
seen as a fundamental trait of schizophrenia spectrum disorders and as a
state that can covary with psychotic
illness in general. A unifying concept
centers on the effects of psychopathological conditions on an individual's
processing resources that results in
either underprovision or overprovision of information from sensory
input to complex cognitive operations dependent on the cerebral
cortex. Findings from a variety of
paradigms are consistent with those
of the masking paradigm in revealing
that the processing deficits of schizophrenics are time dependent and
occur in the 500 ms following
stimulus input.
Formal thought disorder is a chief
defining characteristic of the group of
schizophrenic disorders. In this
447
context, information-processing
approaches to schizophrenia view
thought as the product of a number
of stages or processes, such as the
selection of relevant information
from the environment, elaboration
and interpretation of input, and the
transfer of information throughout
the nervous system. Informationprocessing approaches to the schizophrenias attempt to isolate an
abnormality in the processes that
result in thought. It is this underlying
attentional or information-processing
abnormality, not thought per se, that
is viewed as the basic cognitive
dysfunction in schizophrenia.
Venables (1964, 1973, 1984), for
instance, has argued that disturbed
thinking in schizophrenia can be
traced to an "input dysfunction," in
which, due to a disturbance in the
central and peripheral mechanisms of
arousal, schizophrenics take in either
too much or too little information.
Silverman (1964) similarly proposed
that thought disorder was due to a
"narrowing" or "broadening" of
attention in which either too little or
too much information was transferred to the higher cortical centers
for analysis. Other theorists have
pointed to a breakdown in a
hypothetical filter that normally
serves to screen out irrelevent input.
The impaired filtering hypothetically
causes the higher centers to become
overwhelmed and results in distortions in abstraction and reasoning
(Weckowicz and Blewett 1959;
McGhie and Chapman 1961; Payne
1966). Still others have attributed
thought disorder to an abnormally
slow rate of information transfer,
which results in critical losses of
information and distorted interpreta-
Reprint requests should b>e sent to
Dr. D.L. Braff, UCSD Medical Center,
H620, 225 Dickinson Ave., San Diego,
CA 92103.
448
tions of events (Yates 1966). More
recently, Callaway and Naghdi
(1982) presented a model of schizophrenia as a disorder of information
processing in which schizophrenics
were seen as deficient in processing
tasks characterized as conscious,
serial, and limited in channel
capacity. Processing tasks characterized as automatic, unconscious,
parallel, and of very large capacity,
by contrast, were hypothesized to be
normal or supranormal. In this
context, new evidence indicates that
even apparently simple letterdetection tasks may fall into the
serial-processing category (Sagi and
Julesz 1985), thus accounting for the
rather global deficits seen in schizophrenic patients' informationprocessing abilities.
The information-processing
approach to the study of thought
disorder in the schizophrenias is itself
in the early stages of development
(Kietzman, Spring, and Zubin 1980).
There have been a number of
important attempts to integrate
existing findings along constructs
such as hemispheric processing (Gur
1977, 1978; Magaro 1980), the developmental course of schizophrenia
(Nuechterlein and Dawson 1984),
and perceptual organization (Knight
1984; Kietzman and Zubin, in press).
At present, however, there exists no
fully developed or widely held
model.
The current state of the information-processing approach to
schizophrenia, its promise as well as
its limitations and obstacles, is
exemplified in studies involving the
brief presentation of two or more
stimuli in rapid succession, such as
those involving visual masking. In a
visual-masking paradigm, an informational target stimulus is presented
in close temporal succession with a
noninformational masking stimulus
(Kahneman 1968). When a visual
SCHIZOPHRENIA BULLETIN
stimulus is presented for a short time
and then is terminated, visual
persistence and a host of possible
individual differences in how the
sensory signal might be stored and
analyzed make it virtually impossible
for a researcher to evaluate how the
sensory impulse is experienced by the
higher brain centers. The purpose of
the noninformation masking stimulus
is to limit the manner in which a
sensory signal might vary, thus
providing critical control of input.
As Felsten and Wasserman (1980)
state in their comprehensive review
of the masking literature:
backward masking . . . limits the
duration of the sensory signal
itself . . . . [The mask) can be used
to control the information content
of the sensory signal representing
the TS [target stimulus] . . . a
mask permits the cognitive investigator to do something important
that cannot be done by other
means, namely, to deliver a pulse
of information to the central
nervous system with precise
control on the duration of that
pulse. Without . . . masking,
visual persistence will guarantee
that the duration of the information pulse experienced by the
central nervous system will vary in
an exceedingly complex manner,
[p. 350]
To evaluate possible deficits in one
stage of information processing, it is
necessary to either control or
minimize the demands on all other
stages. Such was the goal in the first
effort to apply the visual masking
technique to schizophrenia. Saccuzzo,
Hirt, and Spencer (1974) attempted
to control for possible differences in
the initial strength of the sensory
impulse by determining the minimal
target exposure duration for criterion
accuracy for groups of paranoid and
nonparanoid schizophrenics, nonpsychotic psychiatric patients, and
normal controls. Then, to control the
duration of the signal, target presentations were followed by a noninformational mask at intervals of 50,
100, 150, 200, and 300 ms following
termination of the target. To
minimize the effects of short-term
memory and higher cognitive
processing such as organizational
strategies, the task was a simple twochoice forced discrimination of a
capital "A" or "T." Results showed
that the two control groups achieved
the no-mask condition level of
accuracy at the 150 ms interval.
Schizophrenics, by contrast, did not
approach their no-mask performance
levels until the 300 ms interval. The
findings, which revealed that schizophrenics required more time than
controls to process the target and/or
deal with the noninformational
mask, supported the notion that
there is a disturbance in the processes
that precede and lead to conscious
thought in schizophrenic patients.
The findings of Saccuzzo, Hirt,
and Spencer (1974) have subsequently been replicated and extended
under a variety of conditions, and
have been shown to be highly
reliable (Saccuzzo and Miller 1977;
Braff and Saccuzzo 1981; Saccuzzo,
Braff, and Sprock 1982; Schwartz,
Winstead, and Adinoff 1983; Green
and Walker 1984). The use of signaldetection methodology, which takes
into consideration errors as well as
correct responses, has ruled out
differences in visual sensitivity and
response strategy in the findings,
indicating that the observed schizophrenic deficit in the masking
paradigm is indeed due to impaired
information-processing capabilities
(Saccuzzo and Braff 1981; Saccuzzo
and Michael 1984). Study of the
effects of medication indicated that
antipsychotic drugs may actually
enhance the performance of schizophrenics in the masking and related
attentionally dependent paradigms
VOL. 12, NO 3, 1986
(Braff and Saccuzzo 1982). And by
demonstrating quantitative as well as
qualitative differences in the masking
performance of schizophrenics and
the elderly, who show generalized
deterioration, Brody, Saccuzzo, and
Braff (1980) have argued against
generalized deficit as the primary
factor in the poor masking performance of schizophrenics (see
Saccuzzo 1977, for a discussion of
generalized deficits in schizophrenia
and old age).
Because no single study can
reasonably be expected to cover all
of the myriad possibilities, information-processing approaches to schizophrenia have required the support of
a marshaling of evidence (Saccuzzo,
in press). A series of studies, for
example, dealt with the issue of
whether the processing disturbance,
as revealed by the masking
paradigm, is simply the result of the
disorder, or a more fundamental
problem linked to its cause. Miller,
Saccuzzo, and Braff (1979) studied
the masking performance of remitted
schizophrenics. Although free of
significant thought disorder, these
individuals exhibited the same poor
performance as actively psychotic
schizophrenics, supporting the
conclusion that impaired processing
is not dependent on the presence of
thought disorder and, indeed, may be
a more enduring feature of schizophrenia than the thinking disorder
itself. In support of such a
conclusion, Braff (1981) and
Saccuzzo and Schubert (1981)
independently demonstrated impaired
masking performance in schizotypal
personality disordered patients with a
nonpsychotic schizophrenia spectrum
disorder believed to be genetically
linked to schizophrenia (Heston 1966,
1970; Meehl 1962). An important
feature of Braff's (1981) study is that
none of the schizotypal patients were
receiving medication; yet, they were
449
as impaired as a group of schizophrenics, most of whom were
receiving antipsychotics. Such
findings parallel those that emerge
when related techniques are used to
test remitted schizophrenics
(Asarnow and MacCrimmon 1978)
and children at risk for schizophrenia
(Asarnow et al. 1978). The finding of
impaired information-processing
capabilities in schizophrenia spectrum
disorders cannot be attributed to
medication, hospitalization, or active
thought disorder, according to
Minnesota Multiphasic Personality
Inventory (MMPI) studies, which
have found poor masking performance in college students showing
MMPI patterns associated with the
schizotypic 2-7-8 code type and/or
schizophrenic linked 8/9/9-8 code
type (Steronko and Woods 1978;
Merritt and Balogh 1984; Saccuzzo et
al. 1984; Balogh and Merritt, in
press; Nakano and Saccuzzo, in
press).
That an information-processing
disturbance, as revealed in the
masking paradigm, may be a trait of
certain subtypes of schizophrenics
and only a state in others was
revealed in a study of Saccuzzo and
Braff (1981). Good prognostic schizophrenics were compared to poor
prognostic schizophrenics and psychiatric as well as normal controls in
eight experimental sessions during the
course of their hospitalization in an
acute care psychiatric hospital. The
psychiatric controls consisted of a
group of depressive neurotics and a
group of manic controls demonstrating hypomania with no evidence
of formal thought disorder. Results
showed that the poor prognosis
schizophrenics had a pronounced
impairment in their ability to evade
the effects of the mask for all eight
sessions. The good prognosis schizophrenics, by contrast, showed
improved masking performance as
their clinical state improved. It was
hypothesized that impaired information processing is a relatively
pervasive and long-lasting trait of the
poor prognosis schizophrenic
patients. In addition, impaired
processing was viewed as a more
transient state of the good prognosis
schizophrenic patients that covaries
with their active psychosis and
theoretically with their thought
disorder.
If impaired information processing
can be both a trait of the poor
prognosis schizophrenic and schizotypal patients and a state that
covaries with thought disorder, then
one might expect to find evidence of
impaired information processing in
nonschizophrenic thought-disordered
patients. Indeed, Schubert, Saccuzzo,
and Braff (1985) found evidence of a
continuum in the degree of information-processing impairment among
schizoaffective, manic, and
psychotic-depressive disorders. All
three groups showed poor masking
performance relative to nonpsychotic
psychiatric and normal controls, yet
could be distinguished among
themselves. Thus, unlike the less
impaired manics tested by Saccuzzo
and Braff (1981), the psychotically
disturbed manics tested by Schubert,
Saccuzzo, and Braff (1985) did show
evidence of a masking disorder. It
remained to be shown, however,
whether schizophrenics could be
distinguished from other psychotically disturbed persons, an issue that
is addressed in the present article.
Method
Subjects. Forty-four psychiatric
inpatients consisting of 11 schizophrenic disorders, 11 schizoaffective
disorders, 11 bipolar affective
disorders, and 11 nonpsychotic
depressed individuals were tested.
The schizophrenic, schizoaffective,
450
and bipolar affective disorders met
the Research Diagnostic Criteria
(RDC) of Spitzer, Endicott, and
Robins (1977) for their respective
groups. All diagnoses were determined by a senior psychiatrist
(D.L.B.) and a trained research
assistant. The nonpsychotic
depressed group met the RDC for a
minor depressive disorder. This
group provided a nonpsychotic
control group. The groups were
matched on age and intelligence as
evaluated by their scaled score on the
Vocabulary Subscale of the Wechsler
Adult Intelligence Scale. Single classification analysis of variance indicated
no significant differences for either of
these variables {p > .05). The groups
did differ on the Global Assessment
Scale (GAS) (Endicott, Spitzer, and
Fleiss 1976), both in lowest GAS
score (F = 6.34, df = 3/40,
p < .005) and overall GAS score
(F = 8.55, df = 3/40, p < .001).
Table 1 provides the means for age,
scaled score on Vocabulary, and
GAS scores for the four groups.
Newman-Keuls analysis of the lowest
GAS score indicated no differences in
the level of severity of impairment
between the schizophrenics and
schizoaffectives. Both of these
groups, however, were significantly
more impaired than the bipolar
disorders (p < .05), who in turn were
more impaired than the nonpsychotic
depressed group. These findings were
paralleled by those for the overall
GAS score.
Patients were screened for a
history of central nervous system
(CNS) damage, mental retardation,
electroconvulsive therapy, and severe
polydrug use. All subjects had at
least 20/30 vision.
Apparatus and Stimuli. Stimuli were
presented in a Gerbrands four-field
tachistoscope. Stimuli were
constructed by mounting black
SCHIZOPHRENIA BULLETIN
Table 1. Mean age, Vocabulary, Global Assessment Scale (GAS),
and critical stimulus duration (CSD) scores
Age
Mean
SD
Vocabulary
Mean
SD
GAS, lowest
Mean
SD
GAS, overall
Schizophrenic
Schizoaffective
Bipolar
Nonpsychotic
depressed
27.18
5.51
26.82
6.42
28.73
7.18
26.64
7.28
10.27
2.87
11.64
2.94
11.73
1.74
10.73
2.05
30.91
9.40
30.82
8.80
37.64
14.14
48.55
10.87
4.91
1.04
5.27
0.79
4.73
1.10
3.36
0.81
12.18
15.58
18.18
18.33
13.09
17.39
6.36
4.86
Mean
SD
CSD
Mean
SD
paratype (Futura bold No. F29-14)
upper case A's and T's on white
stimulus cards. With a viewing
distance of 78.7 cm, stimuli
subtended a visual angle of .20
degrees when presented in the center
of the visual field. Five T's and As
were constructed and presented in
random order in blocks of 10. The
mask consisted of overlapping X's,
completely superimposed over the
letters. Luminance of the target and
masking fields was set at 15
footlamperts. A small dot presented
just above the center in field 3,
illuminated at 1 footlampert,
provided a fixation field
Procedure. After they provided
written informed consent, subjects
were escorted to a dimly lit experimental room where they were read a
standard set of instructions
(Saccuzzo, Hirt, and Spencer 1974)
To ensure that subjects were
attending to the task, the experimenter preceded the presentation of
each stimulus card with the
statement, "Ready, look." In phase 1
of the experiment, the minimum
exposure duration for criterion
identification of the test stimulus
without a mask, which Saccuzzo et
al. (1979) called the "critical stimulus
duration" (CSD), was calculated for
each subject. The procedure for
calculating the CSD followed that
used by Saccuzzo et al. (1979) and
Braff and Saccuzzo (1981). Briefly,
the target stimulus duration was
initially set at 1.0 ms and increased
in increments of 1.0 ms for each
incorrect response until the subject
reached the criterion of seven consecutive correct identifications. The
CSD provides a suprathreshold
exposure duration (see Saccuzzo and
Schubert 1983). Targets were
presented at each subject's independently determined CSDs for the
masking experiment. There are
advantages and disadvantages to the
use of a CSD procedure (see
Saccuzzo 1981; Stanovich and
Purcell 1981; Saccuzzo and Schubert
1983; Schwartz 1983; Long 1984). In
451
VOL. 12, NO. 3, 1986
this experiment, the advantage of
ruling out possible intergroup differences in the ability to identify
unmasked targets outweighed the
possibility of influencing the masking
functions in different ways for
different subjects. It is true that in
normals longer durations shorten the
range of the masking function for
any given subject (Turvey 1973).
Such findings, however, are based on
the unlikely assumption of no
individual differences of the strength
of a sensory signal for any given
duration.
In the present experiment, masking
functions were calculated for four
intervals between termination of the
target and presentation of the mask
(i.e., interstimulus intervals). These
were 20, 60, 120, and 300 ms. A nomask control was also used, which is
an infinite interval between the two
stimuli. For each interval, there were
10 consecutive presentations of the
randomly presented T or A. The
mask was presented for 50 ms, which
provided a mask energy that always
exceeded that of the stimulus
regardless of a subject's CSD. A
typical masking trial was as follows:
The subject fixed on the dot in the
center of the visual field. The
stimulus was presented at the previously determined CSD. There then
followed a dark interval at one of the
four interstimulus intervals. Then the
mask was presented. Subjects
reported orally, "T" or "A." If no
response was given or if they were
not sure, subjects were instructed to
guess T or A before the next trial
began.
Results
Table 1 presents the mean CSDs for
the groups. A single classification
analysis of variance revealed no
statistically significant differences in
these means. Indeed, the range of
CSDs for the three psychotic groups
was less than 6 ms. However,
because the mean of the nonpsychotic depressed group was more
than two times smaller than that for
the three psychotic groups, a series
of individual f tests were conducted
in which each group was compared
to each of the others. Significant
differences were found between the
nonpsychotic depressed group and
each of the other three (p < .05),
indicating this group's target
exposure duration was indeed below
that of the three other groups.
Results for the masking experiment
were evaluated in a 4 (Group) X 5
(Interstimulus Interval) repeated
measures analysis of variance with
repeated measures on the last factor.
There were significant main effects
for Group (F = 4.34, df = 3/40,
p < .01) and Interstimulus Interval
(F = 68.37, df = 4/160, p < .001).
The Group X Interstimulus Interval
interaction was also significant
(F = 1.85, df = 12/160, p < .05).
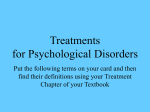
Newman-Keuls analysis of the main
effects indicated no statistically
significant differences among the
schizophrenic (M — 6.00), schizoaffective (M = 6.49), and bipolar
(M = 6.64) disorders (p > .05). All
three of these groups, however, were
significantly below the nonpsychotic
depressed group (p < .01). (See figure
1.) Newman-Keuls analysis of the
main effect for Interstimulus Interval
revealed the typical finding that as
the interval between the stimulus and
mask increased, so did performance.
Newman-Keuls analysis of the interaction indicated that at the 20 ms, 60
ms, and no mask intervals, when
subjects were performing approximately at chance or ceiling, none of
the groups differed significantly
(p > .05). At the 120 ms and 300 ms
intervals, the depressed group was
significantly better than all other
groups (p < .01), who did not differ
significantly from each other.
Discussion
The data revealed that schizophrenic
patients could not be distinguished
from the schizoaffective and bipolar
affective patients on a cross-sectional
basis, with all three groups showing
evidence of a masking deficit.
Consistent with Schubert, Saccuzzo,
and Braff (1985), the data indicate an
information-processing dysfunction
in actively symptomatic schizoaffective and bipolar-disordered
patients. These results, in
conjunction with our previous
findings, are consistent with an interpretation of information-processing
dysfunction as both an enduring trait
of patients with schizophrenia
spectrum disorders and as a state
that probably covaries with the
presence of thought disorder and
psychotic symptoms in psychotically
disordered patients.
From a theoretical standpoint,
there remains the question of why
actively psychotic patients have difficulty with the masking task. One
possibility, which we have favored
(Saccuzzo, Hirt, and Spencer 1974;
Saccuzzo and Braff 1981), is that the
poor masking performance reflects
abnormally slow information
processing. Presumably, the schizophrenic does not rapidly transfer
input to more complex cognitive
operations that theoretically are
dependent on cerebral cortical
mechanisms. This information
transfer problem results in underprovision of accurate information due to
temporal processing limitations and
ultimately leads to distortions of
reality testing. It is also possible,
however, as suggested by Knight
(1984), that at least some schizophrenics process too much inf or-
452
SCHIZOPHRENIA BULLETIN
Figure 1. Backward-masking performance of schizophrenic,
schizoaffective, bipolar, and nonpsychotic depressed inpatients
10r
c
o
Q
o
o
E
• Schizophrenics
A Schizoaftectives
o Bipolars
A Nonpsychotic Depressives
c
to
01
20
300
120
NM
Interstimulus Intervals (msec)
mation because they allocate
unnecessary resources to the
processing of an irrelevant, noninformation mask. In this case, the
problem would be overprovision of
information, a formulation in accord
with impaired filter theories of
schizophrenia. A unifying concept is
that psychotic states deplete an
individual's processing resources,
putting an additional strain on an
already limited system that leads to
impaired performance for all tasks
that require the full use of processing
capabilities (Nuechterlein and
Dawson 1984).
The idea that cognitive dysfunction
in schizophrenia is due to alternating
underprovision (or underutilization)
or to overprovision (or overutilization) of input is consistent with
the traditional theories of schizophrenia advocated by Venables
(1964), Silvertnan (1964), McGhie
and Chapman (1961), Weckowicz
(1958), Yates (1966), and others. Cast
in the context of psychophysiological
(Venables 1984) and psychopharmacological (Matthysse 1974) formulations, information-processing studies
of schizophrenia support a general
theory in which poor prognosis/poor
premorbid schizophrenics and genetically linked spectrum-disordered
patients can be characterized by
underprovision or overprovision of
cortically dependent operations,
caused by an imbalance in normal
disinhibitory or inhibitory processes.
According to the ideas of Venables
(1964) and Mednick (1958), an
affected individual might be plagued
by overprovision at one point in the
disorder that is followed at another
point by overcompensation and then
underprovision at some later time.
The reverse might also be true, with
some individuals beginning with an
imbalance that leads to underprovision followed by overcompen-
sation. Still others might be afflicted
with a lifetime imbalance in only one
direction. Unfortunately, such
complex and variable formulations
seem somewhat inconsistent and are
not easily disconfirmed. However,
this sort of formulation does lend
itself to a nonlinear topographic
analysis (Winfree 1983) that may
ultimately prove of great utility in
analyzing data from schizophrenicdisordered patients. Such nonlinear
approaches also encourage
researchers to obtain multiple,
detailed dependent measures on
schizophrenic patients in order to
chart the time course of schizophrenic deficits. This type of formulation is quite consistent with
Bleuler's (1950) original idea that
there is a heterogeneous and complex
group of schizophrenias.
Based on the ideas of Meehl (1962)
and those of Zubin and Spring
(1977), it seems reasonable to assume
that an information-processing
dysfunction may vary on a
continuum of severity across afflicted
individuals. If it is extreme, then the
impaired processing will almost
certainly lead to the development of
a thought disturbance. At less severe
levels, the processing impairment
might affect personality and social
functioning but not necessarily, or by
itself, cause thought disorder.
Individuals whose inhibitory-disinhibitory imbalance leads to information overutilization will manifest
hypersensitivity and painful anxiety,
especially in social situations. When
the imbalance leads to underutilization, the individual becomes
grossly insensitive to social stimuli.
Missing many of life's subtleties, the
individual fails to experience its
rewards and there is a strong
tendency to social withdrawal.
Whether the individual experiences a
full-blown schizophrenic disorder
depends on a number of factors
453
VOL. 12, NO. 3, 1986
including the stability of the personality organization that evolves, the
flexibility and effectiveness of learned
coping strategies, and, as suggested
by Zubin and Spring (1977), the
severity of the processing impairment
in relation to the degree of environmental stress.
When a high-risk (i.e., severely
impaired information-processing)
individual with an unstable personality organization confronts stressful
events that overtax existing coping
skills, limited processing resources
become further strained. A vicious
cycle may ensue in which strained
resources further limit the
individual's capacity to cope, which,
in turn, enhances the impact of the
stressful event, causing a still further
drain of resources. Eventually the
individual becomes overwhelmed.
Consciousness either spills over with
an uncontrollable flood of input or
becomes brittle and fragmented. And
when the episode is over—the major
symptoms brought under control by
medication and therapy or by
natural cyclic remission, the
individual's processing capabilities
revert to their previous marginal
levels while the sequelae of a schizophrenic episode may linger on. Once
this path has been traveled, it is
somehow facilitated so that it
becomes more easily followed when
the next processing storm occurs.
Current Status of the Icon and Visual
Masking Mechanisms. Interpreting
the results of visual informationprocessing experiments is far from
easy. Allik and Bachmann (1983)
have pointed out that 50 to 100
experiments are published each
month about visual information
storage, iconic memory, visual
persistence, and related issues. Since
Sperling (1960) originally argued that
there is a large capacity, short
duration store of visual information,
thousands of studies have been
completed on the issue of initial
visual storage as high capacity,
evanescent, information store,
termed iconic storage by Neisser
(1967). Related to iconic storage, the
phenomenon of visual persistence has
been unequivocally demonstrated,
but the theoretical significance and
anatomical locus of such persistence
has been debated, dissected, and
disputed. Is there a retinally or
centrally based informational store7
Is there a need to deify such a
storage capacity with a special place
in a sequential informationprocessing theory? After hundreds of
studies and countless hours of
debate, researchers have reached no
clear consensus about this issue.
Haber (1983) has commented extensively on the "demise of the icon"
and the "sharp empirical debates"
that this issue has engendered. To
illustrate the sheer weight of this
literature, Haber (1983) notes that
Long (1980) and Coltheart (1980)
have produced two lengthy reviews
of over 60,000 words and that
neither of these authors "ever raises
any of the questions or concerns
posed by theorists such as Neisser,
Hochberg, Eriksen and Schultz or
Turvey" (Haber 1983, p. 3). Haber's
11-page article received "open peer
commentary" from 32 authors, and
there was wide disagreement about
the utility and accuracy of theories of
iconic memory. If the issue of iconic
memory is controversial when
measured in small groups of normal
subjects, this complexity is greatly
increased when a masking paradigm
is used in groups of psychopathological subjects.
Still, we can summarize the state
of the literature in this area:
• A visual stimulus creates a
retinal response that decays over
time.
• This retinal response has central
correlates.
• The visual response persists after
stimulus termination, and this
persistence probably has retinal and
central components.
• The visual response can be
analyzed for information content and
also is subject to interference by
masking.
• Theories of iconic memory as a
static, purely retinally based "photograph" are outdated and not particularly useful.
Unfortunately, this evaluation
leads to a more complicated
question. How does the mask act in a
visual masking paradigm? Is its
major effect retinal or central? Is the
masking mechanism integrative or
interruptive7 The answer is that
masking can act retinally or
centrally. It also can probably act via
the "merging" of target and mask
stimuli (integration) or via the interruption of target processing via the
action of the mask (interruption). All
of these mechanisms are possible,
depending on the specific conditions
of the experiment (Felsten and
Wasserman 1980).
Visual Processing in Schizophrenic
Patients. For our purposes, we
should examine the conditions of our
typical visual masking paradigm
using schizophrenic patients. In our
studies of psychopathological
subjects, we have used a dark
adaptation period that tends to
increase the duration of visual
persistence to stimuli. We have also
used a target duration (whether fixed
for all subjects or at the CSD) close
to the visual identification threshold
and a powerful (bright and long
duration) mask to limit visual
persistence and to control the pulse
duration of information delivered to
454
the subject Under these conditions,
we initially felt that at longer ISIs
(> 100 ms), masking acts through
central interruptive mechanisms.
According to this formulation, the
masking paradigm performance
deficits of schizophrenic patients
reflect a slowness of information
processing. In addition some schizophrenics, as we have noted, also
show deficient processing of
unmasked stimuli, as revealed by
increased CSDs (Saccuzzo, Hirt, and
Spencer 1974; Braff and Saccuzzo
1981). Initially we interpreted such
CSD findings as evidence for a deficit
in input capabilities in some schizophrenics. Additional studies have not
definitively resolved this issue.
Knight and colleagues (e.g.,
Knight, Sherer, and Shapiro 1977;
Knight and Sims-Knight 1980) used a
picture integration technique and
concluded that schizophrenics had
normal information-processing
functions in the first 100 ms
following stimulus input. Using a dot
integration procedure, Spaulding et
al. (1980) reached similar conclusions. In related work, however,
Schwartz, Winstead, and Adinoff
(1983) specifically evaluated speed of
information processing in schizophrenic patients and normal controls
using a backward-masking paradigm
with varying target stimulus
durations and other paradigmatic
manipulations to evaluate iconic and
visual persistence factors. They
concluded that the retarded
processing shown by schizophrenics
is due, at least in part, to visual
signal abnormalities caused by an
instability or a slower than normal
rate of decay of visual stimuli.
Schwartz, Winstead, and Adinoff
(1983) interpret their findings as
suggesting that temporal integration
is defective in schizophrenia, perhaps
due to increased target stimulus
visual persistence. Thus, the status of
SCHIZOPHRENIA BULLETIN
information processing at the icon
level has yet to be fully understood.
With debates raging over the
theoretical interpretations of iconic
and masking factors, a relatively
atheoretical and clear descriptive
approach seems warranted. Varying
interpretations of masking experiments abound. For example, it is
quite clear that if schizophrenics
show deficits in visual persistence,
their masking deficits may occur via
integrative (versus interruptive)
mechanisms at retinal or CNS levels.
In normals, there is evidence that
masking by integration yields
complex stimuli that register event
related potentials (ERPs) intermediate
between target and mask ERPs
(Schwartz, Whittier, and Schweitzer
1979). This "mixed" ERP occurs even
when the target cannot be
consciously identified. When a
second mask is used, the original
mask becomes ineffective and the
target is once again correctly
identified, but the ERP to the targetmask stimulus is unchanged. Perhaps
the defect shown by schizophrenics in
the visual masking paradigm results
from their inability to screen out the
mask features from the target-mask
stimulus and to identify the critical
target-identifying features from the
montage of a fused or complex
target-mask stimulus. The physiological basis for this phenomenon
would be slowed rates of resolution
of the visual response to the target
and mask stimuli. Thus, the visual
information-processing data in
schizophrenics could be reinterpreted
along the lines of impaired filters as
well as slowness of processing.
Lest we confound issues further,
suffice it to say that the visual
masking paradigm has usefully and
reliably identified a time-linked
deficit in schizophrenic patients. This
deficit occurs in acutely psychotic
schizophrenics and seems to persist
across time in poor prognosis schizophrenics, in schizotypal patients, and
so-called vulnerable but asymptomatic schizotypes identified by 2-7-8
MMPI profiles. In this current study,
the visual-masking abnormality is
reported to be state as well as trait
dependent. Schizoaffective and
thought-disordered bipolar patients
show visual processing deficits
similar to those of schizophrenics.
These results support the idea of both
state- and trait-dependent deficits in
visual information processing by
schizophrenic and other psychotic
patients.
Related Time-Linked Findings. It is
important to note that various information-processing paradigms have
identified schizophrenic patients'
deficits in the epoch of 500 ms after
stimulus presentation (Braff and
Saccuzzo 1984). Thus, a number of
related paradigms, using auditory
and visual processing systems, show
strikingly similar time-linked deficits
in schizophrenia spectrum patients
(Braff 1985). For example;
• Braff, Callaway, and Naylor
(1977) examined self-stimulated
auditory ERPs where the subject
triggers the ERP-eliciting stimulus
after a delay. Normally, ERP
amplitude is inhibited in the selfstimulated versus randomly presented
conditions. Schizophrenics, though,
seemed to show loss of normal
amplitude inhibition in the 250 ms
"ISI" condition (the ISI being the
delay between key release and
stimulus presentation). These results
were interpreted as supporting a loss
of normal inhibitory or sensory
gating influences in information
processing in schizophrenic patients.
• Freedman's group has used an
ERP paradigm that reflects sensory
gating. In a series of systematic and
revealing studies, this group has
VOL. 12, NO 3, 1986
examined the ERP P50 wave to
paired stimuli with a 500 ms conditioning-testing ISI. The second
stimulus-elicited P50 wave is normally
inhibited by the effects of the first
stimulus. Schizophrenic patients and
their first degree relatives share a loss
of normal inhibitory influences as
reflected by increased P50 waves to
the second stimulus (Adler et al.
1982; Freedman et al. 1983; Siegel et
al. 1984). Interestingly, Freedman's
group also reports that this gating or
inhibitory abnormality seems related
to a trait-dependent schizotaxic
factor and a transient, statedependent factor that occurs in
bipolar manic patients (Franks et al.
1983). These results provide a
striking parallel to the visual
masking trait/state formulation.
Adler, Rose, and Freedman (1985)
have also recently reported success in
creating an animal (rodent) model of
their PM gating paradigm which will
allow this group to test specific
neurobiological hypotheses about the
observed P,o abnormalities.
• A third related line of evidence
utilizing human and animal data in
the 50 to 500 ms interval following
stimulus input has evolved from
experiments using the prepulse
inhibition (PPI) of the acoustic startle
response (ASR). This paradigm uses
the blink reflex (in humans) or whole
body startle (in rats) to strong
auditory stimuli. Normally, weak
prestimulation at certain ISIs inhibits
the ASR amplitude in normal
humans. Braff et al. (1978) reported
the loss of this normal prepulse
inhibitory (PPI) effect in the 60 ms
ISI condition in a group of schizophrenic patients. This time-linked
deficit is parallel to the findings of
Freedman and associates. To assess
the possibility that this loss of PPI is
due to dopaminergic dysfunction,
Swerdlow et al. (1986), using
stimulus parameters similar to those
455
used in humans, stimulated rats'
supersensitive dopamine receptors
with low-dose apomorphine and
found a loss of normal PPI of the
ASR with mesolimbic (nucleus
accumbens) but not frontal cortical
supersensitive dopamine stimulation.
This result was also time dependent
and loss of normal inhibition was
maximal in the 60 and 120 ms ISI
conditions. These findings added
significant support to the idea that
the observed time-linked abnormalities in schizophrenic performance
may well be linked to the putative
underlying increase in mesolimbic
dopaminergic tone in schizophrenic
patients.
• There are a host of other, less
time-linked deficits in auditory and
visual information processing in
schizophrenic patients. These include
deficits in tests of distractibility
(Oltmanns and Neale 1975), dichotic
listening (Straube and Germer 1979),
the continuous performance task
(CPT) (Wohlberg and Kornetsky
1973), skin conductance orienting
response (SCOR) (Spohn and
Patterson 1979), startle response
habituation (Geyer and Braff 1982),
smooth pursuit eye movements
(SPEM) (Holzman, Levy, and Proctor
1976), conventional cortical ERPs
(Shagass 1976), and other measures
(see Braff 1985). All these experiments reveal deficits in the ability of
schizophrenic patients to maintain
normal attentional and informationprocessing functions. These results
are compatible with the idea that the
information-processing deficit accrues
in schizophrenia from an inability to
process stimuli serially. None of
these approaches are as time-based
specific as are the visual masking,
ERP, PM, and ASR studies cited
above, but future research may well
examine the interrelationships of
these attention-dependent measures in
schizophrenic patients. We may also
see the effects of increasing
dopaminergic tone and of using
antipsychotic medications on the
information-processing performance
of schizophrenic patients.
Summary
In sum, the viability of an
information-processing approach to
schizophrenia and psychotic illnesses
is supported by numerous interlocking studies, such as those
involving visual masking. While a
complete model has yet to be
developed, the informationprocessing perspective provides a
way of conceptualizing trait/state
and other major theoretical formulations of the psychological and
neurobiological deficits in the group
of schizophrenias and related
psychotic states.
References
Adler, L.E.; Pachtman, E.; Franks,
R.D.; Pecevich, M.; Waldo, M.C.;
and Freedman, R. Neurophysiological evidence for a defect in
neuronal mechanisms involved in
sensory gating in schizophrenia.
Biological Psychiatry, 17:639-654,
1982.
Adler, L.E.; Rose, G.M.; and
Freedman, R. Sensory gating in
rats: Parallels with psychosis. New
Research Program & Abstracts,
American Psychiatric Association
Meeting, 1985. p. 28.
Allik, }., and Bachmann, T. How
bad is the icon? Behavior and Brain
Science, 6:12-13, 1983.
Asarnow, R.F., and MacCrimmon,
D.J. Residual performance deficits in
clinically remitted schizophrenics: A
marker of schizophrenia? Journal of
Abnormal Psychology, 87:597-608,
1978.
SCHIZOPHRENIA BULLETIN
456
Asarnow, R.F.; Steffy, R.A.;
MacCrimmon, D }.-, and Cleghorn,
J.M. An attentional assessment of
foster children at risk for schizophrenia. In: Wynne, L.C.;
Cromwell, R.L.; and Matthysse, S.,
eds The Nature of Schizophrenia:
New Approaches to Research and
Treatment. New York: John Wiley &
Sons, 1978. pp. 339-358.
Balogh, D.W., and Merritt, R.D.
Susceptibility to type A backward
pattern masking among hypothetically psychosis-prone college
students. Journal of Abnormal
Psychology, in press.
Bleuler, E. Dementia Praecox or the
Group of Schizophrenias. (1911)
Translated by J. Zinkin. New
York: International Universities
Press, Inc., 1970.
Braff, D.L. Impaired speed of information processing in nonmedicated
schizotypal patients. Schizophrenia
Bulletin, 7:499-508, 1981.
Braff, D.L. Attention, habituation
and information processing in psychiatric disorders. In: Psychiatry III.
Philadelphia: Lippincott Co., 1985.
pp. 1-12.
Braff, D.L., Callaway, E; and
Naylor, H. Very short term memory
(VSTM) in schizophrenia. Archives
of General Psychiatry, 34:25-30,
1977
Braff, D.L., and Saccuzzo, D.P.
Information processing dysfunction
in paranoid schizophrenia- A two
factor deficit. American Journal
of Psychiatry, 138:1051-1056,
1981.
Braff, D.L., and Saccuzzo, D.P. The
effects of antipsychotic medication on
speed of information processing in
schizophrenic patients. American
Journal of Psychiatry, 139:11271130, 1982.
Braff, D.L.; Stone, C ; Callaway, E.,
Geyer, M.; Glick, I.; and Bali, L.
Prestimulus effects on human startle
reflex in normals and schizophrenics.
Psychophysiology, 15:339-343, 1978.
Brody, D.; Saccuzzo, D.P.; and
Braff, D.L. Information processing
for masked and unmasked stimuli in
schizophrenia and old age. Journal of
Abnormal Psychology, 89:617-622,
1980.
Callaway, E., and Naghdi, S. An
information processing model for
schizophrenia. Archives of General
Psychiatry, 39:339-347, 1982.
Coltheart, M. Iconic memory and
visual persistence. Perception and
Psychophysics, 27:183-228, 1980.
Endicott, J.; Spitzer, R.L.; and Fleiss,
J.L. The Global Assessment Scale: A
procedure for measuring overall
severity of psychiatric disturbance.
Archives of General Psychiatry,
33:766-771, 1976.
or negative symptoms. American
Journal of Psychiatry, 141:12731275, 1984.
Gur, R.E. Motoric laterally
imbalance in schizophrenia: A
possible concomitant of left
hemisphere dysfunction. Archives of
General Psychiatry, 44:33-37, 1977.
Gur, R.E. Left hemisphere
dysfunction and left hemisphere
overactivation in schizophrenia.
Journal of Abnormal Psychology,
87:226-238, 1978.
Haber, R.H. The impending demise
of the icon: A critique of the concept
of iconic storage in visual information processing. The Behavioral
and Brain Sciences, 6:1-11, 1983.
Heston, L.L. Psychiatric disorders in
foster home reared children of
schizophrenic mothers. British
Journal of Psychiatry, 112:819-825,
1966.
Franks, R.; Adler, L.E.; Waldo, M.;
Alpert, J.; and Freedman, R. Neurophysiological studies of sensory
gating in mania: Comparison with
schizophrenia. Biological Psychiatry,
18:989-1005, 1983.
Felsten, G., and Wasserman, G.S.
Visual masking: Mechanisms and
theories. Psychological Bulletin,
88:329-353, 1980.
Freedman, R.; Adler, L.E.; Waldo,
M.C.; Pachtman, E.; and Franks,
R.D. Neurophysiological evidence for
a defect in inhibitory pathways in
schizophrenia: Comparison of
medicated and drug-free patients.
Biological Psychiatry, 18:537-551,
1983.
Geyer, M.A., and Braff, D L.
Habituation of the blink reflex in
normals and schizophrenics. Psychophysiology, 19-1-6, 1982.
Green, M., and Walker, E. Susceptibility to backward masking in
schizophrenic patients with positive
Heston, L.L. The genetics of schizophrenic and schizoid disease. Science,
167:249-256, 1970.
Holzman, P.; Levy, D.; and Proctor,
L. Smooth pursuit eye movements,
attention, and schizophrenia.
Archives of General Psychiatry,
33:1415-1420, 1976.
Kahneman, D. Method, findings, and
theory in studies of visual masking.
Psychological Bulletin, 70:404-425,
1968.
Kietzman, M.L.; Spring, B.; and
Zubin, J. Science of human
behavior. Contributions of the
psychological sciences. In. Kaplan,
H.L.; Freedman, A.M.; and Sadock,
B.W., eds. Comprehensive Textbook
of Psychiatry III. Baltimore: Williams
& Wilkins Co , 1980. pp. 334-371.
Kietzman, M.L., and Zubin, ).
Sensory and perceptual behavioral
markers in schizophrenia. Psychopharmacology Bulletin, in press.
Knight, R.A. Converging models of
VOL 12, NO. 3, 1936
cognitive deficit in schizophrenia.
In: Spaulding, W.D., and Cole, J.K.,
eds. Nebraska Symposium on
Motivation, 1983: Theories of
Schizophrenia and Psychosis.
Lincoln: University of Nebraska
Press, 1984. pp. 93-156.
Knight, R.A.; Sherer, M.; and
Shapiro, J. Iconic imagery in
overinclusive and nonoverinclusive
schizophrenics. Journal of Abnormal
Psychology, 86:242-255, 1977.
Knight, R.A., and Sims-Knight, J.E.
Integration of visual patterns in
schizophrenia. Journal of Abnormal
Psychology, 89:623-634, 1980.
Long, G.M. Iconic memory: A
review and critique of the study of
short-term visual storage. Psychological Bulletin, 88:785-820, 1980.
Long, G.M. The pretreatment of
weighting technique. Journal of
Experimental Psychology: Human
Perception and Performance,
10:140-143, 1984.
Magaro, P.A. Cognition in Schizophrenia and Paranoia: The
Integration of Cognitive Processes.
Hillsdale, NJ: Lawrence Erlbaum,
1980.
Matthysse, S. A theory of the
relation between dopamine and
attention. In: Wynne, L.C.;
Cromwell, R.L.; and Matthysse, S.,
eds. The Nature of Schizophrenia:
New Approaches to Research and
Treatment. New York: John Wiley &
Sons, 1978. pp. 307-310.
McGhie, A., and Chapman, J.
Disorders of attention and perception
in early schizophrenia. British
Journal of Medical Psychology,
34:102-116, 1961.
Mednick, S.A. A learning theory
approach to research in schizophrenia. Psychological Bulletin,
55:316-327, 1958.
Meehl, P.E. Schizotaxia, schizotypy,
457
schizophrenia. American Psychologist, 17:827-838, 1962.
Merritt, R.D., and Balogh, D.W. The
use of a backward masking paradigm
to assess information-processing
deficits among schizotypics: A reevaluation of Steronko and Woods.
Journal of Nervous and Mental
Disease, 172:216-224, 1984.
Miller, S.; Saccuzzo, D.P.; and
Braff, D.L. Information processing
deficits in remitted schizophrenics.
Journal of Abnormal Psychology,
88:446-449, 1979.
Nakano, K., and Saccuzzo, D.P.
Schizotaxia, visual informationprocessing, and the MMPI 2-7-8
code type. British Journal of Clinical
Psychology, in press.
Neisser, U. Cognitive Psychology.
New York: Appleton-CenturyCrofts, 1967.
Nuechterlein, K.H., and Dawson,
M.E. Information processing and
attentional functioning in the developmental course of schizophrenic
disorders. Schizophrenia Bulletin,
10:160-203, 1984.
Oltmanns, T., and Neale, J. Schizophrenic performance when distractors
are present: Attention deficit or
differential task difficulty? Journal of
Abnormal Psychology, 34:205-209,
1975.
Payne, R.W. The measurement and
significance of overinclusive thinking
and retardation in schizophrenic
patients. In: Hoch, P., and Zubin, ].,
eds. Psychopathology of Schizophrenia. New York: Grune &
Stratton, 1966.
Saccuzzo, D.P. Bridges between
schizophrenia and gerontology:
Generalized or specific deficits.
Psychological Bulletin, 84:595-600,
1977.
Saccuzzo, D.P. Input capability and
speed of processing in mental retar-
dation: A reply to Stanovich and
Purcell. Journal of Abnormal
Psychology, 90:172-174, 1981.
Saccuzzo, D.P. An informationprocessing interpretation of theory
and research in schizophrenia.
In: Ingram, R., ed. Information
Processing Approaches to Psychopathology. New York: Academic
Press, in press.
Saccuzzo, D.P., and Braff, D.L.
Early information processing deficits
in schizophrenia: New findings using
schizophrenic subgroups and manic
controls. Archives of General
Psychiatry, 38:175-179, 1981.
Saccuzzo, D.P.; Braff, D.L.; and
Sprock, J. The effect of mental retardation and schizophrenia on
information-processing. Journal of
Nervous and Mental Disease,
170:102-106, 1982.
Saccuzzo, D.P.; Braff, D.L.; Sprock,
].; and Sudik, N. The schizophrenia
spectrum: A study of the
relationship among the Rorschach,
MMPI, and visual backward
masking. Journal of Clinical
Psychology, 40:1288-1294, 1984.
Saccuzzo, D.P.; Hirt, M.; and
Spencer, T.J. Backward masking as a
measure of attention in schizophrenia. Journal of Abnormal
Psychology, 83:512-522, 1974.
Saccuzzo, D.P.; Kerr, M.; Marcus,
A.; and Brown, R. Visual information processing in mental retardation. Journal of Abnormal
Psychology, 88:341-345, 1979.
Saccuzzo, D.P., and Michael, B.
Speed of information-processing and
structural limitations in retarded and
dual diagnosed retardedschizophrenic persons. American
Journal of Mental Deficiency,
89:487-495, 1984.
Saccuzzo, D.P., and Miller, S. The
critical interstimulus interval in
458
delusional schizophrenics and
normals. Journal of Abnormal
Psychology, 86:261-266, 1977.
Saccuzzo, D.P., and Schubert, D.L.
Backward masking as a measure of
slow processing in schizophrenic
spectrum disorders. Journal of
Abnormal Psychology, 90:305-312,
1981.
Saccuzzo, D.P., and Schubert, D.L.
Information-processing in the schizophrenia spectrum: A reply to
Schwartz. Journal of Abnormal
Psychology, 92:503, 1983.
Sagi, D., and Julesz, B. "Where" and
"what" in vision. Science, 228:
1217-1219, 1985.
Schubert, D.L.; Saccuzzo, D.P.; and
Braff, D.L. Information-processing in
borderline patients. Journal of
Nervous and Mental Disease,
173:26-31, 1985.
Schwartz, B. Backward masking as a
measure of slow processing in the
schizophrenia spectrum: A reply to
Saccuzzo and Schubert. Journal of
Abnormal Psychology, 92:504, 1983.
Schwartz, B.D.; Winstead, D.K ; and
Adinoff, B. Visual processing deficits
in acute and chronic schizophrenics.
Biological Psychiatry, 17:1377-1387,
1983.
Schwartz, M.; Whittier, O.M.; and
Schweitzer, P.K. Evoked responses in
retroactively masked stimuli. Physiological Psychology, 7:107-111, 1979.
Shagass, C. An electrophysiological
view of schizophrenia. Biological
Psychiatry, 11:3-29, 1976.
Siegel, C ; Waldo, M.; Mizner, G.;
Adler, L.E.; and Freedman, R.
Deficits in sensory gating in schizophrenic patients and their relatives.
Archives of General Psychiatry,
41:607-612, 1984
Silverman, J. The problem of
attention in research and theory in
schizophrenia. Psychological Review,
SCHIZOPHRENIA BULLETIN
71:352-379, 1964.
Spaulding, W.; Rosenzweig, L.;
Huntzinger, R.; Cromwell, R.L.;
Bnggs, D.; and Hayes, T. Visual
pattern integration in psychiatric
patients. Journal of Abnormal
Psychology, 89:635-643, 1980.
Sperling, G. The information
available in a brief visual presentation. Psychological Monographs,
74 (11, Whole N o . 498), 1960.
Spitzer, R.L.; Endicott, } . , a n d
Robins, E. Research Diagnostic
Criteria (RDC) for a Selected Group
of Functional Disorders. 3rd ed. New
York: New York State Psychiatric
Institute, 1977.
Spohn, H., and Patterson, T. Recent
studies of psychophysiology in
schizophrenia. Schizophrenia
Bulletin, 5:581-611, 1979.
Stanovich, K.E., and Purcell, D.G.
Comment on "Input Capability and
Speed of Processing in Mental Retardation" by Saccuzzo, Kerr, Marcus,
and Brown. Journal of Abnormal
Psychology, 90:168-171, 1981.
Steronko, R.J., and Woods, D.J.
Impairment in early stages of visual
information processing in nonpsychotic schizotypic individuals.
Journal of Abnormal Psychology,
87-481-490, 1978.
stimuli. Psychological Review,
80:1-52, 1973.
Venables, P.H. Input dysfunction in
schizophrenia. In: Maher, B.A., ed.
Progress in Experimental Personality
Research, Vol. I. New York:
Academic Press, 1964. pp. 1-47.
Venables, P.H. Input regulation and
psychopathology. In: Hammer, M.;
Salzinger, K.; and Sutton, S., eds.
Psychopathology: Contributions
From the Social, Behavioral, and
Biological Sciences. New York: John
Wiley & Sons, 1973. pp. 261-285.
Venables, P.H. Cerebral mechanisms,
autonomic responsiveness, and
attention in schizophrenia.
In: Spaulding, W.D., and Cole, J.K.,
eds. Nebraska Symposium on
Motivation, 1983: Theories of
Schizophrenia and Psychosis.
Lincoln: University of Nebraska
Press, 1984. pp. 47-91.
Weckowicz, T.E. Autonomic activity
as measured by the mecholyl test and
size constancy in schizophrenic
patients. Psychosomatic Medicine,
20:66-71, 1958.
Weckowicz, T.E., and Blewett, D.B.
Size constancy and abstract thinking
in schizophrenic patients. Journal of
Mental Science, 105:909-934, 1959.
Winfree, A.T. Sudden cardiac
death: A problem in topology.
Scientific American, 248(5):144-161,
1983.
Straube, E.R., and Germer, C.K.
Dichotic shadowing and selective
attention to word meaning in schizophrenia. Journal of Abnormal
Psychology, 88:346-353, 1979.
Swerdlow, N.R.; Braff, D.L.; Geyer,
M.A.; and Koob, G.F. Central
dopamine hyperactivity in rats
mimics abnormal acoustic startle
response in schizophrenics. Biological
Psychiatry, 21:23-33, 1986.
Yates, A.J. Psychological deficit.
Annual Review of Psychology,
17:111-144, 1966.
Turvey, M.T. On peripheral and
central processes in vision- Inferences
from an information-processing
analysis of masking with patterned
Zubin, J., and Spring, B. Vulnerability. A new view of schizophrenia. Journal of Abnormal
Psychology, 86.102-126, 1977.
Wohlberg, G., and Kornetsky, C.
Sustained attention in remitted
schizophrenics. Archives of General
Psychiatry, 28:533-537, 1973.
459
VOL. 12, NO. 3, 1986
Acknowledgment
The work reported was supported by
a grant from the Scottish Rite
Foundation on Schizophrenia
Research.
Videotapes on
Schizophrenia
Available
The Authors
Dennis P. Saccuzzo, Ph.D., is
Professor, Department of
Psychology, San Diego State
The Video Center of the George
Warren Brown School of Social
Work, in cooperation with several
community and mental health organizations, has produced four videotapes on the following topics relating
to survival issues for chronically
mentally ill persons and their families
in the community.
Coping With a Chronically
Mentally 111 Relative in the
Community—The two videotapes on
this topic were produced in cooperation with the Alliance for the
Mentally 111, St. Louis Chapter. Each
videotape presents the experiences of
a family which has had some success
surviving the multiple problems
arising from caring for a mentally ill
relative in the community. The
videotapes are intended for an
audience of parents and relatives of
chronically mentally ill persons who
could benefit from a vicarious
University, and David L. Braff,
M.D., is Associate Professor,
Department of Psychiatry, School of
Medicine, University of California,
San Diego.
sharing of experiences with the
families on the videotapes.
Psychosocial Rehabilitation: Two
Agencies Based on the Fountain
House Model—These two videotapes
were produced in cooperation with
the Missouri Department of Mental
Health, Independence Center, and
Places for People, St. Louis, MO.
Each videotape presents a psychosocial rehabilitation agency from the
point of view of its members. The
tapes are intended for professional
audiences as well as for families and
mentally ill persons who could
benefit from knowing what it's like
to experience psychosocial rehabilitation "from the inside."
For more information about the
rental or purchase of these videotapes, please contact: Dr. David
Katz, Video Center, Box 1196,
Washington University, St. Louis,
MO 63130.