Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
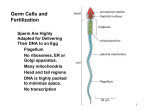
An overview of male reproduction in thalassaemia Vincenzo De Sanctis 1, Ashraf Soliman 2, Mohamed Yassin 3 1 2 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, 44121 Ferrara, Italy Departments of Pediatrics and 3 Hematology, Hamad Medical Center (HMC), Doha, Qatar An overview of male reproduction in thalassaemia Failure of pubertal growth, delay or absence of sexual development, infertility and sexual dysfunction due to hypogonadism and defective spermatogenesis are well recognized disturbances among male patients with thalassaemia major ( -thal). These problems are attributed mainly to the damage caused by chronic anaemia and deposition of iron in the pituitary gland and testicles. In our experience, more and more adult thalassemic patients in their second and third decade of life with the prospect of marriage wish to know their ability to father a child. It is possible to induce or restore spermatogenesis with exogenous gonadotrophins. Although knowing the importance of good compliance with treatment, clinicians have to consider the possibility that overzealous desferrioxamine treatment may adversely affect spermatogenesis and/or sperm function. Much progress has been achieved in the field of male infertility in both diagnostics and treatment. Assisted reproductive techniques may further help these patients to overcome previously untreatable causes of male infertility. This is not a comprehensive review of male fertility problems in thalassaemia. However, it is a short contribution written by pediatric endocrinologists and haematologist with a great interest in the subject and actively involved in the management of male infertility in -thal subjects. Key words: Thalassaemia, Hypogonadism, Iron overload, Chelation therapy, Spermatogenesis, Fertility in males. Endo-Thal Rivista Italiana di Medicina dell’Adolescenza - Volume 10, n. 2, 2012 Today many patients with thalassaemia major ( -thal) successfully survive into adult life, due to remarkable improvement of medical care and to a better understanding of pathogenesis, clinical manifestations and prevention of endocrine complications (1-5). Despite the improvement of the treatment, the involvement of the endocrine system still burdens the life of these patients. In fact, several studies have reported that as many as 51% to 66% of patients may have pubertal failure, sexual dysfunction and infertility, due to hypogonadism (1-5). The causes of male infertility in general population are multiple while in -thal are classically considered to be the result of iron deposition in the endocrine glands (4). Iron overload may be the result of economic circumstances (expense of the chelation therapy), late onset of chelation therapy or poor compliance with treatment (6). Toxicity starts when the iron load in a particular tissue exceeds the tissue or blood-binding capacity of iron, and free nontransferrin iron appears. The ‘free iron’ is a catalyst of the production of oxygen species that damage cells and peroxidize membrane lipids leading to cell destruction (7). Other possible causes of hypogonadism in -thal include liver disorders, chronic hypoxia and associated endocrine complications, such as diabetes (8). This is not a comprehensive review of male fertility problems in thalassaemia. It is not meant to be. However, it is a short contribution written by pediatric endocrinologists and haematologist with a great interest in the subject and actively involved in the management of male infertility in -thal subjects. Endocrine control of pubertal development in males Pubertal development is the result of increasing release of GnRH by the hypothalamus, which stimulates the pituitary to release both gonadotropins LH and FSH. The gonadotropins stimulate the gonads (testis) to develop and produce the sex steroids (testosterone) (Figure 1). FSH stimulates the seminiferous tubules to produce sperms. LH stimulates specialized cells in the testes called Leydig cells to secrete the male hormone, testosterone (9). The rate of LH secretion is influenced by the amount of testosterone circulat- Figure 1. Gonadotrophin secretion and feeback control in males. ing in the blood. FSH secretion is controlled by inhibin. The rate of inhibin secretion is governed by the amount of sperm being made by the seminiferous tubules (9, 10). Besides producing the male characteristics, testosterone enhances the production of sperm. Two important negative feedback loops exist to regulate the secretion of gonadotropins. The testosterone negative feedback loop is established in fetal life and inhibits hypothalamic and pituitary production of GnRH and LH. InhibinB, produced by the Sertoli cell, exerts inhibitory effects on FSH secretion from the pituitary gland, however this negative feedback loop is only established at around puberty (10). Any disruption of this system or dysfunction of its components may lead to infertility (11). The physical changes of puberty Timing of puberty is the result of both genetic constitution and environmental influences. Chronic systemic diseases are often associated with delayed puberty (3, 9). The initial physical sign of puberty is testicular enlargement. At birth testes measure about 1 ml, during the following 2-3 months volume increases to 2 ml, and then decreases again around 6 months 64 Endo-Thal V. De Sanctis, A. Soliman, M. Yassin An overview of male reproduction in thalassaemia Table 1. Pubertal assessment according to Tanner. Penile development Growth of pubic hair P1: Prepubertal PH1: Prepubertal P2: Early puberty (enlargement of scrotum and testes, 4-5 ml, little or no enlargement of penis) PH2: Early puberty (sparse growth) P3: Mid puberty (enlargement of penis and further growth of testes, 8-12 ml, and scrotum) PH3: Mid puberty (hair extends over the pubic junction) P4: Advanced puberty (enlargement of penis in length and breadth. Increased pigmentation of scrotal skin and enlargement of testicles, 15-25 ml) PH4: Advanced puberty (hair corresponds to adult growth but less extensive) P5: Adult PH5: Adult of life. These changes are due to an increase followed by a decrease of androgens during early infancy. Few changes occur until age 11-12 years, when the first signs of puberty develop with an increase in testes volume (3-4 ml) (Table 1). The maximum increase, about 4 ml per year, occurs at a bone age of about 13-14 years. Some children reach complete sexual development in less than 2 years, while others require more than 4 years (9). Testes enlargement is mainly due to the increase in volume and tortuosity of seminiferous tubules. Spermatogenesis commences during puberty and continues throughout life and until old age (12, 13). The assessment of testicular volume is done using Prader’s orchidometer (Figure 2). This is a series of plastic ellipsoids ranging from a volume of 1 ml to 25 ml. The testis, held longitudinally between thumb and index finger, is compared with the ellipsoid with the same volume (14). Physiology of testicular function The testes fulfil two tasks: steroidogenesis and spermatogenesis. Steroidogenesis takes place in the Leydig (interstitial) cells, situated between the seminiferous tubules. Spermatogenesis takes place in the germinal epithelium of these tubules. The germ cells undergo various stages of development from spermatogonia before spermatozoa (mature sperm) reach maturation (Figure 3). This process takes about 60 days to be produced and another 10-14 days for them to pass through the epididymis and vas deferens (12, 13). Disorders of pubertal development and iron overload On average puberty starts at approximately 11 years in boys, with 99% showing a testicular volume of 4 ml or greater by the age of 14 years (9, 14). Delayed puberty is defined as the complete lack of pubertal development in boys by the age of 14 and hypogonadism is defined as the absence of testicular enlargement (less than 4 ml) by the age of 16 years. Also, a pubertal arrest may result in hypogonadotropic hypogonadism after some spontaneous development (15, 16). Hypogonadotropic hypogonadism, which still remains the commonest endocrinopathy in patients with thalassaemia major, has been proven to be the result of hemosiderosis of the gonadotroph cells of the pituitary gland (17-19). An emerging endocrine disorder in young adult -thal subjects is late-onset male hypogonadism (LOMH). LOMH is a disorder caused by the inability of the testes to produce physiologic levels of testosterone and the normal number of spermatozoa as a result of a disruption of the hypothalamic- pituitary-gonadal axis (De Sanctis el al., personal observations). Figure 2. Prader’s orchidometer. Figure 3. Cross-section of human testis in an young adult (from: Reproductive Biology and Endocrinology 2003, 1:107, mod.) 65 Endo-Thal Rivista Italiana di Medicina dell’Adolescenza - Volume 10, n. 2, 2012 There are 2 types of male hypogonadism, regardless of age of onset. Primary; involves testicular failure that results in low testosterone levels, impairment of sper-matogenesis, and elevated gonadotropin levels. Secondary; results from central defects of the hypothalamus or pituitary and is associated with low- to- normal gonadotropin levels (LH and FSH) and low testosterone levels (20-27). The anterior pituitary gland is particularly sensitive to the free radicals produced by oxidative stresses and exposure to these radicals injurious to the gland. Magnetic resonance imaging (MRI) shows that even a modest amount of iron deposition within the anterior pituitary can interfere with its function. Excess iron deposition in the anterior pituitary leads to degranulation of the adenohypophysis and decreased hormone storage with ensuing hypogonadism due to pituitary hyporesponsiveness to gonadotrophin releasing hormone (4, 17-19). Histologically a reduced number of cells and moderate siderosis of the parenchymal cells of the anterior pituitary have been found. Testicular biopsies show various degrees of interstitial fibrosis and hyperpigmentation of undifferentiated seminiferous tubules and a decreased number of Leydig cells (4, 28). Genotype differences may influence the patient’s susceptibility to hypogonadotropic hypogonadism, possibly as a result of differences in the amounts of blood transfused and/or their vulnerability to free radical damage. The pituitary damage is rarely reversible (29). When hypogonadism develops before the age of puberty, the manifestations are those of impaired puberty: • small testes and phallus; • scanty pubic and axillary hair; • disproportionately long arms and legs (from delayed epiphyseal closure); • persistently high-pitched voice. When hypogonadism develops after the age of puberty, some signs and symptoms are suggestive of male hypogonadism, while others are less clearly associated. The patient presents with: • very small, soft or shrinking testes; • loss of libido and activity; • decreased spontaneous erections or impotence; • reduced muscle bulk and strength • reduction of seminal fluid or aspermia (24-27);. The history and the physical examination The cornerstone of the evaluation of infertile man is a careful history including the current problem/complaint, age, occupation, previous seminal analysis findings, any associated medical complication such as diabetes, smoking, alcohol and caffeine consumption (24-27). In the physical examination particular attention should be paid to: 1. Vital signs, body height and weight (BMI), arm-span, secondary sexual characters, and examination of thyroid gland. 2. Features of hypogonadism: Complete or partial development of secondary sexual characteristics (penis length, distribution of body hair, including beard growth, axillary hair and pubic hair). 3. Testicular size: Failure of one or both of the testes to descend into the scrotum or damage to the testicles, such as by injury or after a mumps infection, may reduce sperm production. Because approximately 85% of testicular mass consists of germinal tissue, a reduced germinal cell mass would be associated with a reduced testicular size and a soft consistency. 4. Presence of varicocele: Varicocele which is varicosity of the veins around the testes can occasionally cause infertility. 5. Presence of gynaecomastia: It may be the result of medications, genetic disorders, hyperprolactinemia, or chronic liver disorders. Hormonal measurements Hormonal screening can be limited to the determination of serum concentrations of follicle stimulating hormone (FSH), luteinising hormone (LH), testosterone (T), TSH and prolactin. A low testosterone level is one of the best indicators of hypogonadism of hypothalamic or pituitary origin (24-27). Low LH and FSH values concurrent with low testosterone levels indicate hypogonadotropic hypogonadism (24-27). Elevated FSH and LH values help to distinguish primary testicular failure (hypergonadotropic hypogonadism) from secondary testicular failure (hypogonadotropic hypogonadism) (Figure 4). An elevated FSH level associated with small, atrophic testes implies irreversible infertility (24-27). The total testosterone level should be drawn between 7:00 am and 11:00 am, as it is highest at this time of day. The American Association of Clinical Endocrinologists identifies a total testosterone level below 200 ng/dL as low, while The 66 Endo-Thal V. De Sanctis, A. Soliman, M. Yassin An overview of male reproduction in thalassaemia hypogonadism. MRI may also quantify the pituitary iron deposition (17-19). Figure 4. Hormonal assessment im primary and secondary hypogonadism. Endocrine Society identifies 300 ng/dL as the threshold (30). The diagnostic value of prolactin measurement is extremely low in men with semen abnormalities unless these are associated with decreased libido, erectile dysfunction, and evidence of hypogonadism. Prolactin measurement is warranted in patients with low serum testosterone levels without an associated increase in serum LH levels (24-27). Magnetic Resonance Imaging (MRI) MRI of the pituitary-to-fat signal intensity ratios and the pituitary height and volume are significantly lower in -thal with hypogonadotropic Macroscopic variables Macroscopic variables are volume, pH, coagulation, liquefaction, color and viscosity (Table 2). Table 2. Macroscopic parameters of the semen analysis. Parameters Normal values pH 7.8 Coagulation/liquefaction Coagulates and liquefies within 20 mins at room temperature Colour Whitish-gresy; pearl-white Viscosity 4 mm threading Table 3. Lower reference limits (5 centiles and their 95% confidence intervals) for semen characteristics (from: WHO manual for Semen Analysis, 5th Edn, 2010). th Parameter Semen volume (mL) Total sperm number (106 per ejaculate) Semen analysis Although semen analysis is not a test of fertility, a carefully performed semen analysis is a highly predictive indicator of the functional status of the male reproductive hormonal cycle, spermatogenesis and the patency of the reproductive tract. The World Health Organization Laboratory Manual for Examination of Human Semen and SemenCervical Mucous Interactions is highly recommended for technical details (31). In the detection of male factor fertility problems, basic semen analysis using the WHO criteria is a sensitive test (sensitivity of 89.6%, i.e. it is likely to detect nine out of ten men who have ‘true’ semen abnormality), but it has poor specificity (an abnormal test result does not always mean there is a true semen abnormality). Analysis of repeat semen samples provides greater specificity in identifying semen abnormalities; a single-sample analysis will falsely identify about 10% of men as abnormal, but repeating the test reduces this to 2% (31). Lower reference limit 1.5 (1.4-1.7) 39 (33-46) Sperm concentration (106 per mL) 15 (12-16) Total motility (progressive and non-progressive, %) 40 (38-42) Progressive motility (%) 32 (31-34) Vitality (live spermatozoa, %) 58 (55-65) Sperm morphology (normal forms, %) 4 (3.0-4.0) 67 Microscopic variables The microscopic parameters assess spermatogenesis (Table 3). The minimum number of specimens to define good or poor quality of semen is three samples over a 6-8 week interval with a consistent period of abstinence of 2-3 days. A repeat semen analysis should be requested after two to three months, bearing in mind that a complete spermatogenesis cycle lasts for 74 days. Classical semen analysis, which includes sperm concentration, motility and morphology, gives an approximate evaluation of the functional competence of spermatozoa. • Low numbers of sperms and poor sperm movement can have an impact on fertility. • Abnormally shaped sperms can also result in failure to conceive. • Abnormal level of white blood cells could indicate an infection. The fertilizing potential of sperm depends not only on the functional competence of spermatozoa but also on sperm DNA integrity. Sperms Endo-Thal Rivista Italiana di Medicina dell’Adolescenza - Volume 10, n. 2, 2012 with compromised DNA integrity, regardless of the degree of DNA damage, appear to have the capacity to fertilize oocytes at the same rate as normal sperm. However, the embryos produced by fertilization of an oocyte with DNA damaged sperm can not develop normally (32) . Therefore, the evaluation of sperm DNA integrity, in addition to routine sperm parameters, could add further information on the quality of spermatozoa and improved predictive values could be obtained from validated sperm DNA fragmentation assays. The most commonly used techniques to assess sperm DNA integrity are the TUNEL and sperm chromatin structure assays (SCSA) (32). What we know about fertility potential in thalassaemia? The personal experience Virtually very little is known about spermatogenesis in ( -thal). In summary, we found: • A normal sperm count and motility in 45% of fully sexually mature -thal subjects (33) • A possible detrimental effect of iron chelation therapy on spermatogenesis. Three out four patients with serum ferritin levels lower than 500 ng/ml had poor sperm motility (34) • A higher degree of defective chromatin packaging in -thal subjects with low sperm concentrations (32) • A low seminal plasma of zinc, citric acid and prostate specific antigen. These data suggest an impaired prostatic secretion (35) • An increase of seminal lipoperoxidation. These findings indicates an increase of oxidative stress in the semen of these patients that could contribute to the impairment of sperm motility (36) • An increase of DNA sperm damage and a negative correlation with sperm motility. These findings suggest that iron overload predispose sperm to oxidative injury (32) • Blood transfusion is associated with significant acute enhancement of sperm parameters and increased concentrations of serum T, LH, FSH, and IGF-1. These “acute” effects on spermiogenesis are reached by an unknown mechanism and suggest a number of pathways that need further human and/or experimental studies (5) • Abnormal seminal parameters and low serum acid folic levels have been found in subjects with thalassaemia intermedia (37). Iron chelation therapy Combined therapy (use of two chelators on the same day), may induce negative iron balance and may reverse hypogonadism and endocrine complications in severe iron overloaded -thal subjects (38-40). Long-term studies have shown that deferiprone and deferoxamine (DFO) have shown to accelerate iron chelation by rapidly reducing liver iron, serum ferritin, and myocardial siderosis.Combination chelation therapy with deferasirox and DFO has also been shown beneficial (39). Counselling Sometimes certain ‘lifestyle’ factors may be responsible for poor semen quality. For example obesity, alcohol abuse, use of anabolic steroids, extreme sports and increase in scrotal temperature through thermal underwear, sauna or hot tub use or occupational exposure to heat sources. A considerable number of drugs can also affect the spermatogenesis (41). Hormonal treatment Hormonal treatment of pubertal disorders in thalassaemia is a complex issue due to the many associated complications. Therefore, each patient has to be assessed individually. Collaboration between endocrinologists and other doctors is critical (42). The treatment of delayed or arrested puberty, and hypogonadotrophic hypogonadism depends on factors such as age, severity of iron overload, damage to the hypothalamo-pituitary-gonadal axis, chronic liver disease, and the presence of psychological problems resulting from hypogonadism (43). Although thalassaemics who fail to enter puberty or whose puberty is arrested before complete sexual maturation has occurred are considered to be sterile for life, we found that this is not necessarily true and that gonadotropin treatment (hCG and hMG) can achieve spermatogenesis (44, 45). Because of advances in fertilization and sperm banking technologies, all subjects, even those with extremely low sperm counts and motility, should be considered candidates for sperm cyropreservation (33). 68 Endo-Thal V. De Sanctis, A. Soliman, M. Yassin An overview of male reproduction in thalassaemia For delayed puberty in males, low dosages of intramuscular depot-testosterone esters (25 mg) are given monthly, at a bone age of about 12 years, for 6 months to stimulate growth velocity.This is accompanied by only an early pubertal development. In patients with hypogonadism therapy can continued and the dose increased to 100 mg/mo. until the growth rate begins to wane.The fully virilising dose is 75-100 mg of depot-testosterone esters every 10 days administered intramuscularly or 100 mg/m² twice a month. (46). The same effects can be achieved with topical testosterone gel. Treatment of hypogonadotropic hypogonadism may be initiated for 2 purposes: androgenization and/or induction of fertility. It is known that hCG binds to Leydig cell LH receptors and stimulates the production of testosterone. Male patients with onset of hypogonadotropic hypogonadism before completion of pubertal development may have testes generally smaller than 5 ml and usually require therapy with both hCG and human menopausal gonadotropin (or FSH) to induce spermatogenesis. The initial regimen of hCG is usually 1,000 to 2,000 IU administered intramuscularly two times a week. The clinical response is monitored, and testosterone levels are measured every 2 to 3 months. Dosage adjustments of hCG may be needed to determine an optimal schedule. The disadvantages of hCG include the need for more frequent injections and the greater cost. Larger testis volume is a useful prognostic indicator of response (44). If the patient is fully virilized and 8-12 months of hCG therapy have not led to the production of sperm, then FSH therapy should be initiated (44). FSH is available as human menopausal gonadotropin (hMG). Sperm banking procedures, even in subjects with reduced sperm count and motility is recommended (33). Once a pregnancy has occurred, the FSH therapy can be stopped and spermatogenesis can be maintained with hCG alone. Men with arrested puberty or with postpubertal, acquired hypogonadotropic hypogonadism may initiate and maintain production of sperm with hCG therapy only (47). Infertility In presence of infertility, the male and female partners are evaluated to determine the cause and best treatment options. Infertility is defined 69 by the World Health Organization as the “inability of a sexually active, non-contracepting couple to achieve pregnancy in one year”. Although no universally accepted consensus exists between specialties on the management of infertility, several algorithms have been devised to provide an initial assessment of the infertile male (48). Today new assisted reproductive techniques (ART) offer hopes to many couples (22-27): • intra-uterine insemination is used for mild male factor infertility problems; • intracytoplasmic sperm injection (ICSI) as a management for severe male factors or for recurrent unexplained failed in vitro fertilization (IVF) cycles (25). ICSI is a procedure that is performed in conjunction with IVF. With ICSI, a single sperm from the male partner is injected directly into a woman's egg (oocyte) in the laboratory. The pregnancy rate with ICSI is approximately 20% to 40% per cycle (22-24). • adoption is offered for cases with recurrent unexplained failed IVF cycles and donor insemination for azoospermia; • testicular sperm extraction (TESE) and intracytoplasmic sperm injection (ICSI) has been used in patients with Klinefelter syndrome and azoospermia (49). No case report in thalassaemia are available in literature but at our knowledge this is a procedure suggested by some Experts in reproductive thechniques in patients with azoospermia and arrested puberty. International guidelines are required to assist these patients because it is widely accepted that infertility and involuntary childlessness, and the decision to engage with assisted reproduction technology services as a patient, donor or surrogate can entail wide-ranging psychosocial issues (50). In conclusion, failure of pubertal growth, delay or absence of sexual development, infertility and sexual dysfunction due to hypogonadism and defective spermatogenesis are well recognized disturbances among male patients with thalassaemia major. These problems are attributed mainly to the damage caused by chronic anaemia and iron deposition in the pituitary gland and testicles. At present, one of the major problems dealing with adult patients with beta-thalassemia are “fertility” and “osteoporosis”. In our experience, more and more adult thalassemic patients in their second and third decades of life, with the prospect of marriage, wish to know their ability to father a child. Endo-Thal Rivista Italiana di Medicina dell’Adolescenza - Volume 10, n. 2, 2012 It is possible to induce or restore spermatogenesis with exogenous gonadotrophins in some of them. Clinicians should recognize that both big iron overload (defective chelation) and overzealous use of desferrioxamine may adversely affect spermatogenesis and/or sperm function. Much progress has been achieved in the field of male infertility, both in the diagnostics and treatment aspects. Assisted reproductive techniques may supplementary help these patients to overcome previously untreatable causes of male infertility. References 1. Galanello R, Origa R. Beta-thalassemia. Orphanet J Rare Dis 2010; 5:11. 2. De Sanctis V, Elawwa A, Angastiniotis M, et al. Highlights from the First Thalassaemia Forum on Growth and Endocrine Complications in Thalassemia Doha, (October 23, 2011). Pediatr Endocrinol Rev 2012; 9:672-679. 3. Proceedings of the Ares-Serono Foundation 2nd International Workshop on Growth and Endocrine Complications and Reproduction in Thalassaemia. Ferrara, Italy. April 2-4, 1998. J Pediatr Endocrinol Metab 1998; 11(Suppl 3):771-1008. 4. De Sanctis V, Giovannini M. Endocrine histology findings in a prepubertal thalassemic girl with multiple endocrine complications secondary to iron overload. Georgian Med News. 2011; 193:51-55. 5. Soliman A, Yasin M, El-Awwa A, et al. Acute effects of blood transfusion on pituitary gonadal axis and sperm parameters in adolescents and young men with thalassemia major: a pilot study. Fertil Steril 2012 Jun 28. [Epub ahead of print] 6. Hoffbrand AV, Wonke B. Iron chelation therapy. J Intern Med Suppl 1997; 740:37-41. 7. Hershko C.Pathogenesis and management of iron toxicity in thalassemia. Ann N Y Acad Sci 2010; 1202:1-9. 8. De Sanctis V, D'Ascola G, Wonke B. The development of diabetes mellitus and chronic liver disease in long term chelated beta thalassaemic patients. Postgrad Med J 1986; 62:831-836. 9. Sizonenko PC. Normal sexual maturation. Pediatrician 1987; 14:191-201. 10. Plant TM, Marshall GR. The functional significance of FSH in spermatogenesis and the control of its secretion in male primates. Endocr Rev 2001; 22:764-786. 11. McLachlan RI. The endocrine control of spermatogenesis. Baillieres Best Pract Res Clin Endocrinol Metab 2000; 14:345-362. 12. Urso L, De Sanctis V. The physiopathology of spermatogenesis in adolescents. A review of the literature and the authors' own experience. Minerva Pediatr 1998; 50:71-80. 13. De Sanctis V, Scialpi V, Urso L. Spermatogenesis in developmental age.Minerva Pediatr 1998; 50:269-274. 14. Zachmann M, Prader A, Kind HP, et al. Testicular volume during adolescence. Cross-sectional and longitudinal studies. Helv Paediatr Acta 1974; 29:61-72. 15. Belchetz PE, Barth JH, Kaufman JM. Biochemical 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. endocrinology of the hypogonadal male. Ann Clin Biochem. 2010; 47(Pt 6):503-515. Multicentre study on prevalence of endocrine complications in thalassaemia major. Italian Working Group on Endocrine Complications in Non-endocrine Diseases. Clin Endocrinol (Oxf). 1995; 42:581-586. Soliman AT, el Zalabany MM, Ragab M, et al. Spontaneous and GnRH-provoked gonadotropin secretion and testosterone response to human chorionic gonadotropin in adolescent boys with thalassaemia major and delayed puberty. J Trop Pediatr 2000; 46:79-85. Hekmatnia A, Radmard AR, Rahmani AA, et al. Magnetic resonance imaging signal reduction may precede volume loss in the pituitary gland of transfusion-dependent betathalassemic patients. Acta Radiol 2010; 51:71-77. Au WY, Lam WW, Chu WW, et al. A cross-sectional magnetic resonance imaging assessment of organ specific hemosiderosis in 180 thalassemia major patients in Hong Kong..Haematologica 2008; 93:784-786. Young J. Approach to the male patient with congenital hypogonadotropic hypogonadism. J Clin Endocrinol Metab 2012; 97:707-718. Grinspon RP, Loreti N, Braslavsky D, et al. Sertoli cell markers in the diagnosis of paediatric male hypogonadism. J Pediatr Endocrinol Metab 2012; 25:3-11. McLachlan RI, Krausz C. Clinical evaluation of the infertile male: new options, new challenges. Asian J Androl 2012; 14:3-5. Loughlin KR.Changes in male fertility in the last two decades. Urol Clin North Am 2012; 39:33-36. Schlegel PN. Male infertility: evaluation and sperm retrieval. Clin Obstet Gynecol. 2006; 49:55-72. Kim ED. An overview of male infertility in the era of intracytoplasmic sperm injection. Zhonghua Yi Xue Za Zhi (Taipei) 2001; 64:71-83. Schlegel PN. Evaluation of male infertility. Minerva Ginecol 2009; 61:261-283. Spitz A, Kim ED, Lipshultz LI. Contemporary approach to the male infertility evaluation. Obstet Gynecol Clin North Am 2000; 27:487-516. Vogt HJ, Weidenbach T, Marquart KH, Vogel GE. Idiopathic hemochromatosis in a 45-year-old infertile man. Andrologia 1987; 19:532-538. Vullo C, De Sanctis V, Katz M, et al. Endocrine abnormalities in thalassemia.Ann N Y Acad Sci 1990; 612:293-310. Petak SM, Nankin HR, Spark RF, et al. American Association of Clinical Endocrinologists.American Association of Clinical Endocrinologists Medical Guidelines for clinical practice for the evaluation and treatment of hypogonadism in adult male patients--2002 update. Endocr Pract 2002; 8:440-456. World Health Organisation. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed. Geneva: World Health Organization; 2010. De Sanctis V, Perera D, Katz M, et al. Spermatozoal DNA damage in patients with B thalassaemia syndromes. Pediatr Endocrinol Rev 2008; 6(Suppl 1):185-189. De Sanctis V, Katz M, Wonke B, et al. Semen parameters in patients with homozygous -thalassemia. Infertility 1989; 12:167-174. De Sanctis V, Borsari G, Brachi S, et al. Spermatogenesis in 70 Endo-Thal V. De Sanctis, A. Soliman, M. Yassin An overview of male reproduction in thalassaemia 35. 36. 37. 38. 39. 40. 41. 42. young adult patients with beta-thalassaemia major longterm treated with desferrioxamine. Georgian Med News 2008; 156:74-77. Carpino A, De Sanctis V, Siciliano L, et al. Epididymal and sex accessory gland secretions in transfusion-dependent betathalassemic patients: evidence of an impaired prostatic function. Exp Clin Endocrinol Diabetes 1997; 105:169-174. Carpino A, Tarantino P, Rago V, et al. Antioxidant capacity in seminal plasma of transfusion-dependent beta-thalassemic patients. Exp Clin Endocrinol Diabetes 2004; 112:131-133. De Sanctis V, Candini G, Giovannini M, et al. Abnormal seminal parameters in patients with thalassemia intermedia and low serum folate levels. Pediatr Endocrinol Rev 2011; 8 (Suppl 2):310-313. Farmaki K, Tzoumari I, Pappa C, et al. Normalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia major.Br J Haematol 2010; 148:466-475. Galanello R, Agus A, Campus S, et al.Combined iron chelation therapy. Ann N Y Acad Sci 2010; 1202:79-86. Berdoukas V, Farmaki K, Wood JC, Coates T. Iron chelation in thalassemia: time to reconsider our comfort zones. Expert Rev Hematol 2011; 4:17-26. Tournaye HJ, Cohlen BJ. Management of male-factor infertility.Best Pract Res Clin Obstet Gynaecol. 2012 Jun 15. [Epub ahead of print] Forti G, Krausz C. Clinical review 100: Evaluation and Corrispondenza: Vincenzo de Sanctis, MD Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy Phone: +39 0532 20 76 22 Email: [email protected] 71 43. 44. 45. 46. 47. 48. 49. 50. treatment of the infertile couple. J Clin Endocrinol Metab 1998; 83:4177-4188. Soliman AT, Nasr I, Thabet A, et al. Human chorionic gonadotropin therapy in adolescent boys with constitutional delayed puberty vs those with beta-thalassemia major. Metabolism 2005; 54:15-23. De Sanctis V, Vullo C, Katz M, et al. Induction of spermatogenesis in thalassaemia. Fertil Steril 1988; 50:969-975. Cisternino M, Manzoni SM, Coslovich E, Autelli M. Hormonal replacement therapy with HCG and HU-FSH in thalassaemic patients affected by hypogonadotropic hypogonadism. J Pediatr Endocrinol Metab 1998; 11(Suppl 3):885890. Rosenfield RL. Low-dose testosterone effect on somatic growth. Pediatrics 1986; 77:853-857. Depenbusch M, von Eckardstein S, Simoni M, Nieschlag E. Maintenance of spermatogenesis in hypogonadotropic hypogonadal men with human chorionic gonadotropin alone. Eur J Endocrinol 2002; 147:617-624. Curti G, Cánepa Cantú L, Montes JM M. Diagnosis of Male Infertility: A Need of Functional and Chromatin Evaluation. Actas Urol Esp. 2012 Jun 16. [Epub ahead of print] De Sanctis V, Ciccone S. Fertility preservation in adolescents with Klinefelter's syndrome. Pediatr Endocrinol Rev 2010; 8 Suppl 1:178-181. Blyth E. Guidelines for infertility counselling in different countries: Is there an emerging trend? Hum Reprod 2012; 27:2046-2057.