Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Turner syndrome wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Pericardial heart valves wikipedia , lookup
Electrocardiography wikipedia , lookup
Echocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Aortic stenosis wikipedia , lookup
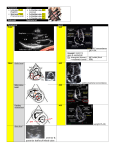
11/11/11 Objectives Point-of-Care Echocardiography Rimon Bengiamin, MD, RDMS • Discuss the goals of point-of-care cardiac ultrasound • Review the cardiac anatomy • Explore strategies for image (window) acquisition • Develop recognition of pathology on images • Discuss integration of point Why do echo in the Emergency Department? • Faster! • Expedite care • Narrow the differential • Get much of the same information In what capacity should it be used? • Keep the exam straightforward • Evaluate for gross abnormalities and overall cardiac function obtained by invasive monitoring 1 11/11/11 Primary Indications • Cardiac arrest • Pericardial Effusion • Massive PE • LV function • Unexplained hypotension • Estimation of CVP Anatomy Advanced Applications • Severe valvular dysfunction • Proximal aortic dissection • Myocardial ischemia Flow 2 11/11/11 Anatomy Cardiac Probe • Small footprint • Deep penetration • 2-4 MHz • Good for motion not clarity Image/Probe Orientation I m confused!!! • Most confusing study in terms of orientation • Based on standard echo views in cards • Usually when you set the machine to the cardiac probe, it will flip the normal image orientation. However, this isn t always true. • Just learn the standard views and recognize structures Radiology Cardiology 3 11/11/11 I can t get images!!! • Difficult • Few sonographic windows because of ribs, the sternum, and lungs in the way • Bone shadows • Lungs are air filled so they don t transmit sonographic sound waves Subxiphoid 4-chamber The Standard Views • Subxiphoid • 4-Chamber • Short Axis • Subcostal Long Axis/IVC • Parasternal • Long Axis • Short Axis • Apical 4 chamber • Suprasternal Subxiphoid 4-chamber • Most useful view in emergency ultrasound • Can see: • Effusion • Chamber size and function • Both AV valves • Similar to the FAST view 4 11/11/11 Subxiphoid 4-chamber Subxiphoid Short-Axis • Similar to the parasternal RA short axis view RV • Evaluate wall motion, LV mitral valve, and aortic valve • Great in COPD patients • Rotate your probe 90 o LA Subxiphoid Short-Axis counterclockwise from the four-chamber view Subxiphoid Short-Axis LV 5 11/11/11 Subxiphoid Long-Axis • Good for Subcostal Long-Axis evaluating the IVC for volume status and right-sided heart pressures • Aim the probe dot toward the patient s feet Subcostal Long-Axis Parasternal Long-Axis • Ventricle function Liver and size • Mitral/aortic valve • Aortic outlet RA IVC 6 11/11/11 Parasternal Long-Axis Parasternal Long-Axis RV AoV Ao LV Parasternal Short-Axis MV LA Parasternal Short-Axis • LV wall motion • Mitral/aortic valve function 7 11/11/11 Parasternal Short-Axis Parasternal Short-Axis LA LV Apical 4-Chamber • Overall heart function • Ventricle/atrial chamber size • Wall motion • Valve function • Pericardial fluid • pressure gradients 8 11/11/11 Apical 4-Chamber Apical 4-Chamber Septum RV LV MV TrV RA Suprasternal LA Suprasternal • Aortic arch, brachiocephalic artery, left carotid and left subclavian 9 11/11/11 Suprasternal Ao Arch Ascending Ao Clinical Indications Right PA Descending Ao Cardiac Arrest/PEA • Palpation of pulses is unreliable • Studies showing that some patients with pressures of 50-80 systolic did not have palpable pulses (Mandavia et al). • Examination of cardiac function with US during codes can help assess patient prognosis Cardiac Arrest/PEA • Ultrasound is most helpful in guiding/narrowing the differential • Differential of PEA • 5 H s - hypovolemia, hypoxia, acidosis (hydrogen), hypo/hyperkalemia, hypoglycemia, hypothermia • Those with contractility should undergo active • 5 T s - tox, tamponade, pneumo (tension), MI • Those with cardiac standstill are unlikely to be • Ultrasound can pick up hypovolemia, MI, PE, and resuscitation revived (Salen et al). (thrombus) , PE (thrombus) tamponade. 50% of your differential isn t bad! 10 11/11/11 Cardiac Arrest PEA Pericardial Effusion Pericardial Effusion • Plummer et al • 100% sensitivity • decreased time to diagnosis from 42.4 minutes to 15.5 minutes • increased survival from 57.1% to 100% • Variable, nonspecific presentation in the setting of nontraumatic effusions • At risk include idiopathic/viral pericarditis, HIV, hepatitis B, bacterial pericarditis, fungal pericarditis, autoimmune processes, Dressler syndrome, drug induced (INH, cyclosporine), neoplastic, radiation, renal failure, hypothyroid, etc, etc, etc. 11 11/11/11 Pericardial Effusion Pericardial Tamponade • Any patient with a pericardial effusion is at risk for developing tamponade • Remember the starling curve • Slowly accumulating effusion gives the pericardium time to stretch • A quickly accumulating effusion reaches a critical point where cardiac function is impaired ( last drop phenomenon) Pericardial Tamponade Pericardiocentesis 12 11/11/11 Pericardial Clot Massive Pulmonary Embolism • 70% of patients who die from PE die within the first hour • Early thrombolytic therapy or embolectomy is required • Don t wait for time-consuming imaging in unstable patients • A combination of echo and DVT study can help you determine whether or not to consider lytics or call CT surgery Massive Pulmonary Embolism Dilated RV • Findings • Massive right ventricular dilatation • Right sided heart failure • Small, vigorously contracting left ventricle • Know the patient s history • Some patients have chronic right heart strain such as those with pulmonary hypertension 13 11/11/11 Dilated RV Undifferentiated Hypotension • Broad differential for shock patients • Main goal is to narrow that differential • Is the patient euvolemic or hypovolemic? • Look at the IVC • Keep in mind other causes of hypotension (tamponade, pneumo, PE, etc) Undiffentiated Hypotension Distended IVC • IVC • Normal IVC diameter is 1.5-2.5 cm • Normal respiratory variation in size • Should collapse around 50% with deep inspiration • Complete collapse = hypovolemia • No collapse = hypervolemia 14 11/11/11 Myocardial Ischemia • Good for use as an extra diagnostic tool • Can help differentiate CHF from COPD in Wall Motion Abnormality The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again. chest pain patients • Look for left ventricular dysfunction • Look for large IVC • Look for wall motion abnormality LV function poor normal LV function poor normal 15 11/11/11 Valvular Dysfunction Mitral Stenosis • Ultrasound can be useful for evluation of valvular dysfunction that results in critical failure • Usually an incidental finding • Advanced • With time and studies you will start to recognize abnormalities Aortic Aneurysm/ Dissection normal abnormal Aortic Aneurysm/Dissection • Look at the aortic root in the long axis parasternal view • Look at the aortic arch by attempting the suprasternal view • Normal aortic root is approx 3 cm • Look for a false lumen Normal Abnormal 16 11/11/11 Aortic Dissection Summary • Learn basic views • Start with subxiphoid and paraternal • Try to produce standard images • Always use the same method • Practice on normal patients • Abnormalities may be obvious False Lumen Questions ? 17