Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
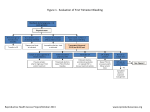
The significance of quantitative serum Beta Human Chorionic Gonadotropin level availability during pelvic ultrasonography for suspected obstetric or gynecologic pathology Michael Roux, MD; John Gonzales, MD; Jonathan Gromis, MS,BA; Kathy Solomon, MD; Victor McLaughlin, MD; Alexander Kagen, MD Purpose: Ultrasonography is among the few highly operator-dependent modalities in diagnostic radiologic imaging, requiring an understanding of anatomy, physiology, and the suspected pathology being investigated at the time of image acquisition. Interpretation of sonographic images is also highly dependent on the available clinical findings and laboratory data. Requests for emergent pelvic ultrasonography are received with variable accompanying clinical information available. The importance of quantitative serum Beta Human Chorionic Gonadotropin (β-HCG) level to the interpreting radiologist was studied, in our quest to provide timely, accurate, and high-quality diagnostic reporting. Materials/Methods Used: In this study we reviewed emergent pelvic ultrasonography studies performed at our institution for suspected obstetric or gynecologic pathology, to determine if the report generated would have changed significantly if the quantitative β-HCG level were available at the time of interpretation. Attending radiologists were presented with previously-unknown β-HCG values for retrospective analysis and then interviewed regarding aspects of their report which would have differed given the additional information. Results: Initial analysis demonstrates that knowledge of the patient's quantitative serum β-HCG level at the time of image interpretation will lead to the reporting of more specific diagnostic information in many instances, and can potentially alter the interpretation of a study altogether. Conclusions: Given promising initial results from our analysis, further research into this subject is warranted. In this retrospective study we were unable to assess whether or not the availability of relevant laboratory data would have influenced the images acquired by the technologist or by the resident or attending radiologist, though we do suspect that such information may provide additional pre-imaging value which may justify the routine practice of imaging after the availability of laboratory data. Authors Michael Roux, MD; John Gonzales, MD; Jonathan Gromis, MS,BA; Kathy Solomon, MD; Victor McLaughlin, MD; Alexander Kagen, MD Department of Radiology Icahn School of Medicine at Mount Sinai Beth Israel Disclosures: Nothing to disclose. Introduction • Ultrasonography is among the few highly operator-dependent modalities in diagnostic radiologic imaging, requiring an understanding of anatomy, physiology, and the suspected pathology being investigated at the time of examination. • Interpretation of sonographic images is also highly dependent on the available clinical findings and laboratory data. • Requests for emergent pelvic ultrasonography are received with variable accompanying clinical information. • The importance of quantitative serum Beta Human Chorionic Gonadotropin (β-HCG) level to the interpreting radiologist was studied, in our quest to provide timely, accurate, and highquality diagnostic reporting. Background • β-HCG is the hormone most utilized both qualitatively and quantitatively in the diagnosis of pregnancy. After implantation, it is produced by the syncytiotrophoblast, the embryonic placental epithelial layer. Circulating β-HCG binds to the ovarian luteinizing hormone/choriogonadotropin receptor (LHCGR) in order to preserve the corpus luteum during the first trimester of pregnancy, maintaining synthesis of progesterone. Progesterone, in turn, promotes myometrial relaxation and endometrial morphologic changes which maintain the fetus during early gestation. • Quantitative β-HCG levels characteristically double approximately every 29 to 53 hours within the first 30 days following normal intrauterine implantation. The rate of increase in hormone level then begins to progressively slow, to an eventual peak between approximately 8 to 10 weeks gestation. Peak levels may reach 200,000 mIU/ml or greater, and range widely. From weeks 10-20, β-HCG levels decrease to an average of 12,000 mIU/ml. Subsequently, β-HCG levels remain relatively constant until the end of pregnancy. • After delivery or termination, the serum β-HCG declines to undetectable levels within 7 to 60 days, depending on the level at the time of delivery or termination. The hormone level decreases with a half time of 9 to 31 hours within the first several days, slowing to a half time between 55 and 64 hours thereafter. Background • The serum β-HCG level, particularly when trended, may help distinguish a normal viable intrauterine pregnancy (IUP) from multiple gestation, ectopic pregnancy, molar pregnancy, fetal demise, or abortion variants. • Imaging findings in combination with the β-HCG level help guide medical vs surgical therapy for ectopic pregnancy – β-HCG level less than 5,000 mIU/ml, absence of fetal cardiac activity, and absence of tubal rupture (or secondary signs thereof) are important to the clinician considering Methotrexate therapy • It has generally been accepted that an intrauterine pregnancy should be detectable sonographically by a β-HCG level between 1,000-2,000 mIU/ml. • Criteria from the Society of Radiologists in Ultrasound 2012 Consensus Conference advocate for an increased threshold of 3,000 mIU/ml before a pregnancy of unknown location is presumed to be ectopic, and that even in this circumstance a repeat β-HCG level and sonogram are recommended prior to treatment. • ACR Appropriateness Criteria for First Trimester Bleeding specifies that imaging results should be correlated with the quantitative β-HCG level and with clinical presentation, and that lack of IUP above a discriminatory β-HCG level does not necessarily indicate ectopic pregnancy. Methods and Data Analysis • In this study we reviewed emergent pelvic ultrasonography studies performed at our institution in 2014 for patients with known or suspected pregnancy and unknown β-HCG level, to determine if the report generated would have changed significantly if the quantitative β-HCG level were available at the time of interpretation. • In many instances, the result of a urine dipstick qualitative analysis for pregnancy is available while the quantitative βHCG value is unknown. Methods and Data Analysis 1151 emergent pelvic ultrasound studies ordered by the highest volume emergency department at our institution in the year 2014 were identified. Studies performed in the setting of known or suspected pregnancy were then extracted, and filtered by interpreting attending radiologist. Studies with simultaneously-obtained quantitative β-HCG levels which were unknown to the radiologist during interpretation, but available in the EMR, were extracted and recorded. Available attending radiologists were presented with β-HCG values for retrospective review of studies which they originally interpreted. These radiologists were asked to consider if their impression or follow-up recommendations would have differed in a clinically-meaningful way given the additional information. Repeat analysis was performed after excluding examinations performed on women with known prior ultrasound imaging performed by the Department of Radiology and/or OB/GYN for the same pregnancy. Results After exclusion of all studies which did not meet the defined criteria, and those for which the interpreting radiologist was unavailable: • 25 studies remained for analysis • In 3 of 25 studies (12%) the impression would have differed • In 2 of 25 studies (8%) the follow-up recommendations would have differed After the additional exclusion of examinations with known prior ultrasound imaging performed by the Department of Radiology and/or OB/GYN for the same pregnancy: • 18 studies remained for analysis • In 2 of 18 studies (11.1%) both the impression and follow-up recommendations would have differed Discussion of Results • In 12% of cases, knowledge of the quantitative serum β-HCG level may lead to a different impression than that which would be reported on the basis of imaging alone. In 8% of cases, this knowledge may lead to different follow-up recommendations. • The presence or absence of prior imaging for the same pregnancy did not appear to alter the significance of this lab value to the radiologist. • In one instance where both the impression and followup recommendations would have differed, β-HCG level availability would have led the radiologist to report a very high suspicion for ectopic pregnancy, potentially prompting more expeditious OB/GYN referral. Limitations • Faculty turnover and availability considerations limited the number of studies available for analysis. • In this retrospective study we were unable to assess whether or not the availability of relevant laboratory data would have influenced the images acquired by the technologist or by the resident or attending radiologist. • This study also did not assess for overall differences in patient outcomes due to its retrospective design. Conclusion and Implications • Knowledge of the patient's quantitative serum β-HCG level at the time of image interpretation will lead to the reporting of more clinically-meaningful diagnostic information in many instances, and can potentially alter the interpretation of a study altogether. • Given promising initial results from this study, further research into this subject using larger data sets is warranted. • Assessment for inter-observer agreement would also bring strength to future studies. • Such future investigations may guide the development of uniform departmental policies regarding lab value availability during emergent pelvic sonography in the patient with known or suspected pregnancy. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. American College of Radiology ACR Appropriateness Criteria®: First Trimester Bleeding. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/FirstTrimesterBleeding.pdf. Updated 2012. Accessed April 2014. Billieux M.H., et al. Early and Late Half-life of Human Chorionic Gonadotropin as a Predictor of Persistent Trophoblast After Laparoscopic Conservative Surgery for Tubal Pregnancy. Acta Obstetricia et Gynecologica Scandinavica 2003;82(6):550. Butts S.F., et al. Predicting the Decline in Human Chorionic Gonadotropin in a Resolving Pregnancy of Unknown Location. Obstetrics and Gynecology 2013; 122(2 Pt 1):337-43. Doubilet, P., et al. Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester. N Engl J Med 2013;369:1443-51. Johnson, S.R., et al. Levels of Urinary Human Chorionic Gonadotropin (hCG) Following Conception and Variability of Menstrual Cycle Length in a Cohort of Women Attempting to Conceive. Current Medical Research &Opinion 2009;25(3):741-8. Jou H.J., et al. Second Trimester Maternal Serum hCG in an Asian Population: Normal Reference Values by Ultrasound Dating. Journal of Maternal Fetal Medicine. 2000;9(2):118-21. Kirchler, H.C., et al. Early Diagnosis of Tubal Pregnancy: Changes in Tubal Blood Flow Evaluated by Endovaginal Color Doppler Sonography. Obstetrics and Gynecology 1993;82(4 Pt 1):561. Lipscomb, G.H., et al. Predictors of Success of Methotrexate Treatment in Women with Tubal Ectopic Pregnancies. N Engl J Med 1999;341(26):1974-8. Menon, S., et al. Establishing a Human Chorionic Gonadotropin Cutoff to Guide Methotrexate Treatment of Ectopic Pregnancy: A Systemic Review. Fertility and Sterility. 2007;87(3):481-4. Midgley, A.R. and Jaffe R.B. Regulation of Human Gonadotropins. Disappearance of Human Chorionic Gonadotropin Following Delivery. Journal of Clinical Endocrinology and Metabolism. 1968;(12):1712. Mock, P., et al. The Apparent Late Half-life of Human Chorionic Gonadotropin (hCG) After Surgical Treatment for Ectopic Pregnancy. A New Approach to Diagnose Persistent Trophoblastic Activity. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1998;78(1):99. Steier J.A., et al. Human Chorionic Gonadotropin in Maternal Plasma After Induced Abortion, Spontaneous Abortion, and removed Ectopic Pregnancy. Obstetrics and Gynecology 1984;64(3):391.