Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
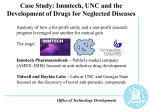
Clinical and Translational Research Center Addendum Version: 5/4/2017 CTRC Addendum to the IRB Application If you plan to use a CTRC Facility and any of its many services and resources, please complete the form below. The success of your study is important to us and it is imperative that you outline carefully what you need so that the CTRC Staff are ready and able to meet those needs. Along with the completed addendum, include the billing and cost assignment sheet, contract, budget and, if appropriate, time and event worksheet/flow sheets. Provide us with your study’s IRB application, industry or master protocol, and investigator brochure. Instructions are highlighted in yellow. You may delete both highlighted text and sections regarding optional services that you are not using prior to submitting this addendum. CTRC Protocol Number Title of Study: Protocol Version Date: Principal Investigator: UNC Medical Staff Appointment Yes Telephone #: Pager #: No Study Coordinator: UNC Medical Staff Appointment Yes Telephone #: Pager #: No Email Address: Email Address: Main Nurse Practitioner/PA (if applicable): UNC Medical Staff Appointment Yes No Telephone #: Pager #: Email Address: *Study Physician (if not Principal Investigator): UNC Medical Staff Appointment Yes No Telephone #: Pager #: Email Address: *Medical orders and physician oversight are required when research participants are admitted to the CTRC. 1 Clinical and Translational Research Center Addendum Check ALL services you plan to use Version: 5/4/2017 REQUIRED SECTIONS FOR ALL PROTOCOLS SECTION to complete X Safety Monitoring Plan A X Biostatistics and Database Management B X Cost Determination and Assignment C OPTIONAL CTRC SERVICES Study Medication or Investigational Agent Administration D Outpatient clinical services (CTRC at UNC Hospitals) E Outpatient clinical services (CTRC at Burnett-Womack) E Inpatient admissions (CTRC at UNC Hospitals) F Meals: Research diets, regular meals and/or nourishments G Research Nutritionist services G Body Composition Measurements G Dental Research: General Oral Health Center H Specimen Processing Facilities and Sample Storage I 2 Clinical and Translational Research Center Addendum Version: 5/4/2017 Section A. Safety Monitoring Plan (Revised June 23, 2009): All CTRC and TraCS supported protocols require a protocol-specific Safety Monitoring Plan (SMP). Providing the answers to the questions below will formulate a SMP that is specific for the study. The SMP can then be used by your study team as a guide when implementing and monitoring the protocol. Please read and answer each question carefully and completely. If the requested information can be found in the protocol and is too large to cut and paste into this form, you may reference the page number(s) and section(s) where the information is located. For information or assistance in writing a Safety Monitoring Plan, contact David Weber, phone 843-0725, [email protected] or Marie Rape, phone 966-6844 [email protected]. 1. What is the level of risk to subjects for this protocol? Please refer to the Protocol Risk Assessment and Monitoring Guidelines to assist you in determining and justifying the Risk Level. SELECT ONE: Level 1: No greater than minimal risk--Non-interventional or risk no more than experienced in daily life (e.g., blood draw, physical exam, MRI, exercise testing) Level 2: Minor increase over minimal risk Level 3: Moderate risk Level 4: High risk AND For Risk Levels 2-4: In a few sentences, please justify risk level: 2. What tests, evaluations, or observations will be performed to monitor subjects and minimize risks? Provide us with a visit table, schedule of events, or list of specific tests and evaluations that will be used, and their frequency, to assess subjects and monitor for toxicity. Describe any other measures in place to minimize risk. 3. Which classification scale will be used to grade the severity of adverse events (AE)? For protocols that do not have a specific grading scale, the most recent Common Terminology Criteria for Adverse Events (CTCAE scale) is recommended. A scale of mild-moderate-severe (as defined below) may be used for simple studies. NOTE: Although not anticipated, adverse events may occur in any study and should be tracked (whether or not they are reportable) and graded by the investigator or study physician. AE tracking templates can be uploaded from the OCT website. SELECT ONE: Adverse Event Grading Scale: Mild Adverse Event – Event results in mild or transient discomfort, not requiring intervention or treatment; does not limit or interfere with daily activities (e.g., insomnia, mild headache). Moderate Adverse Event – Event is sufficiently discomforting so as to limit or interfere with daily activities; may require interventional treatment (e.g., fever requiring antipyretic medication). Severe and undesirable Adverse Event – Event results in significant symptoms that prevents normal daily activities; may require hospitalization or invasive intervention (e.g., anemia resulting in blood transfusion). 3 Clinical and Translational Research Center Addendum Version: 5/4/2017 Common Terminology Criteria for Adverse Events v3.0 (CTCAE) Division of AIDS Table for the Grading the Severity of Adult and Pediatric Adverse Events (DAIDS AE Grading table) Other. Please describe or provide protocol reference: 4. To whom and with what frequency will Unanticipated Problems and Adverse Events be reported? PLEASE CHECK TO INDICATE YOUR UNDERSTANDING OF LOCAL REPORTING REQUIREMENTS Reporting of Unanticipated problems and adverse events to the IRB (IRB SOP Section 19.0) All NON-SERIOUS unanticipated problems and adverse events that are both unexpected AND related or possibly related to participation in the research will be reported to IRB within two weeks of the investigator becoming aware of the event. All SERIOUS unanticipated problems and adverse events will be reported within one week of the investigator becoming aware of the event. Upon review of the report, the IRB will make a final determination as to whether the event places the subjects or others at greater risk than previously recognized. All reports will be submitted directly to the IRB. AND Discuss reporting of unanticipated problems and adverse events to the sponsor, FDA or NIH: OR There are no additional reporting requirements for this study. Questions 5-8 pertain to studies with a research intervention (administering a medication, substance, or investigational agent; exposure to experimental conditions, etc.). Please mark N/A if not applicable to your study. Not Applicable (no research interventions included in study) 5. What are the subject stopping rules? List the specific reasons or adverse events (including grade or number) that would lead to a subject having the research intervention discontinued or put on hold. If there are any rules for dose escalation or de-escalation, please describe. 6. Identify the committee or group responsible for monitoring or reviewing adverse events in aggregate across the entire study population for the protocol SELECT ONE AND DESCRIBE Single-center, Moderate Risk protocols, Phase I or II trial: This study requires a plan for aggregate analysis of adverse events. Describe who (person or committee) is responsible for receiving and reviewing adverse events in aggregate across the entire study population; summarize how and at what intervals data will be reviewed. 4 Clinical and Translational Research Center Addendum Version: 5/4/2017 OR Multi-center, high-risk protocols or Phase III trials: This study requires a Data Safety Monitoring Board (DSMB) or Data Monitoring Committee (DMC) to monitor the protocol. Describe the committee that will monitor this study; provide a copy of the charter or details of the membership and frequency of meetings. If a DSMB or SMC will not be utilized, explain why not. 7. Are there any study-wide stopping rules for this protocol? Describe rules for when the entire study would be stopped (in all subjects) and re-evaluated for either safety or efficacy reasons. 8. Who will monitor this study? Provide the name of the company or organization and frequency of any monitoring. If there is no outside monitoring, describe who will handle study documentation and describe your plans for performing quality control/assessment of source documents to ensure the accuracy of data collected. SELECT ONE Industry Sponsor or CRO monitor: (name) Frequency of monitoring: OR No outside monitoring—Internal self-monitoring will be performed. At least 10% of individual case report forms and source documents will be reviewed to confirm that all recorded data is verifiable, accurate and complete. Areas to be assessed include informed consent process, subject eligibility, Case Report Form (CRF) and/or source document completion/accuracy, Adverse Event Reporting, and Drug Accountability (as applicable). OR No outside monitoring—Other Internal self-monitoring plan. Please describe: 5 Clinical and Translational Research Center Addendum Version: 5/4/2017 Section B. Biostatistics and Database Management All CTRC applications should provide sufficient detail to allow useful biostatistical review. A master protocol is recommended for all studies. If you have questions or if you would like a pre-review of your statistical plan, please contact Paul Stewart, [email protected], phone 966-7276. For assistance in completing Database Management questions, contact Clarence Potter, [email protected], phone 966-4802. 1. Does this study have a Master Protocol document with sections that completely specify the plans for data analysis and data management? a. Yes. Please submit the master protocol and list the appropriate page reference where this information can be found. IF all questions are completely addressed in the master protocol, you DO NOT need to answers questions 2 – 5 below. List page references: ____________ b. No. Please address questions 2 – 5. If you have access to a biostatistician, ask them to complete this section for you. If you do not have access to a biostatistician, please contact Paul Stewart for assistance in answering these questions. If a particular question has been addressed adequately in the IRB Application or in the Master Protocol, you may reference that section rather than repeat the details in the box below. 2. Characteristics: aims, study design, sample size, and randomization: a. What are the scientific aims and practical objectives of this study? (Examples: publication, get data for a grant proposal, pilot-test procedures, study feasibility, estimate parameters, generate hypotheses, test hypotheses, etc.) b. What were the primary considerations in choosing the proposed sample size? (Examples: stage of this line of research, specific aims, patient availability, costs, precision of statistical estimates, power of statistical hypothesis test) c. What is the plan for randomization (if any) and who will perform the computations? (Examples: stratified randomization, permuted blocks, constrained-block allocation sequences).) 3. As used in the analyses, what will be the units and scales of the most important variables? (Examples: HIV viral load (l og10 copies/mL), CD4+ (count), Weight (kg), etc. 4. Statistical analysis of the data a. Who will perform the statistical computations and who will analyze the results? 6 Clinical and Translational Research Center Addendum Version: 5/4/2017 b. For what parameters will statistical estimates be obtained? (Examples: proportions, medians, mean differences, variances, prevalence rates, etc.) i. What levels of precision are anticipated for the most important estimates? (Examples: expected width of confidence interval, expected magnitude of standard error, etc.) ii. What are your plans for computing confidence intervals for these estimates? c. What hypotheses (if any) will be tested and what test procedures will be used? i. What is your strategy for controlling the probability of type I errors? (Example issues: multiple comparisons, rate of false discoveries, test size (), etc.) ii. What levels of power are anticipated for each of the most important tests? iii. Will this study be a success even if no tests are statistically significant? 5. Database Management a. What are the plans for data management (RDM)? (Examples of aspects: data entry, quality assurance, data editing, data archival, etc.) b. How will you verify that the data has been entered into the database correctly? (Examples: quality assurance monitoring, double-entry, independent verifications, etc) c. What software will be used for database management? d. Who will perform the computations for data management? (Examples: data retrievals and numerical comparisons for monitoring, reporting, etc.) e. What are the plans for ensuring that custom-written algorithms, sub-routines, formulas, or macros perform correctly without error? 7 Clinical and Translational Research Center Addendum Version: 5/4/2017 Section C. Cost Determination and Assignment General Instructions: The information you provide by completing the Cost Assignment Sheet (see next page) will be used to determine resource utilization and cost of CTRC resources and to identify the person(s) responsible for specific costs. Protocol Categorization: Determination as to what extent a research project will be supported will be determined by the CTRC Oversight Committee. A research protocol is designated as one of the following categories: Category B Studies Study initiated by a Early-Stage Investigator (NIH/Grant, Foundation, Department sponsored, Network studies, or unfunded research) Category C Studies Study initiated by an investigator (NIH/Grant,Foundation, Network studies, Department sponsored, or unfunded research) Category D Studies Study initiated by an investigator or industry and sponsored by industry Definition of Early-Stage Investigator: A Principal Investigator is considered an “Early Stage Investigator” if he/she is within 10 years of completing his/her terminal research degree or is within 10 years of completing medical residency (or the equivalent). Investigator-initiated Protocols: Investigator-initiated studies are generally funded by a non-profit, state, or government agency; however in some cases, studies may also receive industry funding. For multi-center studies, UNC does not have to be the coordinating center; however; the research must meet all of the following criteria to receive a designation as an Investigator-initiated protocol: The research is within the investigators’ area(s) of academic research interest. The investigator(s) have had substantial input into protocol design for the proposed protocol and take responsibility for the quality of the protocol. The principal investigator will have full control of the data and will be the responsible author for all major publications that result from the research. IMPORTANT: For information or assistance in completing the Cost Assignment Sheet, please contact Leslie Powell, 919-843-0267, [email protected]. 8 3/3/09 Billing and Cost Assignment Sheet: Please Read Instructions Protocol Number: Title of Study: Principal Investigator: Telephone #: Pager #: Study Coordinator: Telephone #: Pager #: Departmental billing /Cost Sheet contact: Telephone #: Pager #: Email Address: Email Address: Email Address: Is this study (choose one): *Investigator initiated Industry initiated * Investigator-initiated studies must meet ALL of the four criteria listed in the instructions. Are you (choose one) : *Early-Stage investigator *Senior investigator *Refer to definitions in the instructions Are you requesting Research on Location (CTRC staff comes to in-patient hospital or outpatient clinic setting)? Yes No Are you requesting the CTRC Dietary Services to prepare meals for your patients (please note that there is now a charge for each meal)? Yes No Please indicate ALL funding sources that will pay for this study (check all that apply): Federal funds Industry funds Other (foundation, dept, etc.) If Other, name funding source: Are you applying for TraCS Pilot Funding? Yes No If yes, have you received APPROVAL for funding? Yes No If yes, FUNDING AMOUNT: $ Total number of subjects: Estimated duration of study (i.e., subject interaction): Number of outpatient subjects: Number of inpatient subjects: years Number of outpatient clinic visits/subject: Number of inpatient NIGHTS/subject: REQUEST FOR TESTS, PROCEDURES, MEDICATIONS AND/OR SUPPLIES Name of Test/Procedure (e.g., Lab, CXR, Dexascan, lidocaine, etc) See exceptions below(1) Number per Subject Test/Procedure billed to: (Check one) Lab or Department performing test See examples below(2) Investigato Subject / r 98 Insurance Account CTRC 3 DO NOT list “kit” labs (i.e., those being sent to a Central lab) or other non-billable tests and/or procedures for which the Sponsor has provided you with materials and/or equipment. 2. Examples: McLendon Labs, Investigator Lab, Body Composition, Cardiology, Pulmonary or Core Facility Labs. PLEASE NOTE: “ Core Lab” refers to UNC core facilities that provide support for clinical investigators, not McLendon Core Lab. 3. CTRC should not be chosen for any study approved after September 1, 2009. No Costs will be paid for by the CTRC if approved after this date. 1. 9 3/3/09 98 Account Number for Investigator charges: 98#: PI Signature: Date: CTRC Approval Signature: Date: Category of research for billing purposes (Designation to be made by CTRC): ____________________ 10 3/3/09 Optional Services: COMPLETE SECTION(S) RELEVANT TO YOUR STUDY Section D. Study Medication or Investigational Product Administration You are required to register with the Investigational Drug Service (IDS) Pharmacy if your study involves the administration and dispensing of any agents (commercial medications, supplements, or investigational drugs/products). This policy is a JCAHO requirement and a means of assuring compliance with Federal regulations and quality control. Information regarding IDS services, policies and application forms can be obtained at http://pharmacy.intranet.unchealthcare.org/services/investdrugs The Investigational Drug Service has two locations: 3rd floor, Main Hospital, Room 3001. Dispenses injectable medications and chemotherapy. Phone: 966-3469. Ground Floor Neurosciences, across from ENT clinic. Oral medications dispensed from this location. Phone: 966-8739. 1. Will study medications or agents be administered as part of the research protocol? Yes No 2. If you plan to utilize the services of IDS, have you submitted your proposal and the required forms to IDS? Yes No: If no, complete the Request for Investigational Drug Services form. Section E. Outpatient Clinical Services Outpatient clinical services are located at two clinics, the CTRC at UNC Hospitals and the CTRC at Burnett-Womack. Depending on the complexity of the research to be performed and/or the level of acuity of the research subjects we will assist you to develop a plan that will allow best utilization of our clinic space. Outpatient visits in the CTRC facilities can be scheduled using the online scheduling system, http://tracs.unc.edu/ctrc/patient-scheduling.html or by calling: CTRC at UNC Hospitals: 966-1437; CTRC at Burnett-Womack: 966-1404. Studies planning to use nutrition resources please schedule by email to [email protected] 1. If requesting CTRC Outpatient Clinical Services, indicate your facility preference or study requirement (you may check one or both facilities): (Check all that apply) CTRC at UNC Hospitals Types of clinical services requested (check those that apply): Phlebotomy Infusions / PK Visits (indicate visit length) 1-4 hrs 11 3/3/09 4-8 hrs 8-12+hrs Clinic room use for routine visits, medical exams giving questionnaires, Specialized equipment use in outpatient clinic rooms (PFT or ultrasound machines) Bionutrition Core resources. CTRC at Burnett-Womack Types of clinical services requested (check those that apply): Phlebotomy Infusions / PK visits (indicate visit length) 1-2hrs 2-4 hrs Clinic room use for ECGs, routine visits, medical exams, giving questionnaires, 2. CTRC Flow sheet. Extensive outpatient clinic visits (infusions, pharmacokinetic sampling) require a time and event/flow sheet outlining specific requirements of the protocol. Use the sample format found at: http://tracs.unc.edu/docs/ctrc/CTRC_Outpatient_Flow_Sheet.doc Yes – provide a copy with the CTRC addendum No – will submit a copy at a later date Not applicable to this study 3. Indicate any equipment or specific supplies required for your protocol. Please tell us if any supplies needed for your study must be ordered by the CTRC in advance 4. If your protocol requires assistance with processing samples, describe study needs. Please provide written processing and storage instructions before study begins. 5. Please list any study procedures/interventions that require the assistance of CTRC nursing staff (i.e., EKG, exercise testing, patient education, conscious sedation). Intervention / Procedure Who to Perform 12 Nursing Assistance Needed 3/3/09 Section F. Inpatient Admissions (CTRC Inpatient Unit at UNC Hospitals) Research subjects requiring an inpatient admission (in unit after midnight) will be admitted to the CTRC Inpatient unit located on the 3rd floor Bedtower, UNC Hospitals. This unit has 10 inpatient hospital rooms that can be utilized for TraCS Institute approved research protocols. Investigators utilizing the CTRC Inpatient Unit are required to provide written medical orders and physician oversight for the period of the admission. For more information, contact the CTRC Nursing Team Leaders , [email protected] , phone 843-0560, pager 216-6991. 1. How much advance notice will you have in scheduling admissions? Prior to one week Less than 48 hours notice Other: Please explain 2. What time of day do you anticipate subjects arriving for admission? Early Morning Afternoon Late Evening 3. If your protocol requires IV placement and/or IV fluid administration, provide details. 4. If your study requires administration of chemotherapy, medications, or infusions, provide details. Length of infusion: Frequency: 5. Please list any study procedures/interventions that require the assistance of CTRC nursing staff. (i.e., EKG, exercise testing, patient education, conscious sedation). Please describe the procedure/intervention: Intervention/ Procedure Who Will Perform procedure? CTRC Assistance Needed 6. If your protocol requires assistance with processing samples, describe study needs. Also include processing and storage instructions. 7. If this study involves infusions, pharmacokinetic sampling or other timed procedures, provide a nursing flow sheet to the team leaders prior to enrolling your first subject. Use the sample format found at: http://tracs.unc.edu/docs/ctrc/CTRC_Inpatient_Flow_Sheet.doc 8. Please provide any other information necessary for successful implementation of your study: 13 3/3/09 Section G. Nutrition, Body Composition, and Metabolic Food Lab The CTRC includes a Bionutrition Core which provides consultation for methods development and implementation of nutrition studies for investigators. The Bionutrition Core includes a state-of-the-art metabolic research kitchen located in the CTRC at UNC Hospitals. Many resources needed for the conduct of rigorous clinical nutrition studies are available for investigator use – i.e., body composition measurements by DXA, pQCT, and indirect calorimetry. The core has a well trained and experienced research and dietetic staff. . If you plan to use any of this core’s services, please clearly describe your requirements below. All research protocols requesting Bionutrition Core services and/or those that involve overnight admission in the CTRC at UNC Hospitals please complete #1 below. For assistance or information on the Bionutrition Core, contact Beth MacIntosh, [email protected], phone 966-4746. 1. Diet Requirements (please describe in detail or refer us to the correct page in the Master Protocol): Inpatient Meals Regular Research Therapeutic Describe Meal specifications: Outpatient Meals Regular Research Therapeutic Describe Meal specifications: 2. Procedures performed by Research Dietitian (please describe in detail or refer us to the correct page in the Master Protocol): Subject Screening for Research Diet Adherence Nutrition Assessment / Diet History Food Frequency Questionnaire Food Records/Dietary Intake Diet Instruction Nutrient Intake Analysis of Research Diet Describe in detail or refer to page in the Master Protocol: 3. Body Composition Measurements (please describe in detail or refer us to the correct page in the Master Protocol): All body composition procedures should be listed on the Cost Assignment Sheet. DXA (bone density, body composition). Indicate the measurements you are requesting: If yes, fill out the DXA Radiation Safety form located at the address below and send to Radiation Safety. http://tracs.unc.edu/docs/ctrc/App_for_Human_Use_of_Ionizing_Radiation_in_Research.doc Whole Body Bone Densitometry Whole Body Composition Lumbar Spine Hip IVA peripheral QCT (bone structure). Indicate the measurements you require. If yes, fill out the DXA Radiation Safety form located at the address below and send to Radiation Safety. http://tracs.unc.edu/docs/ctrc/App_for_Human_Use_of_Ionizing_Radiation_in_Research.doc 14 3/3/09 Radius Tibia Indirect Calorimetry (Resting Energy Expenditure, Respiratory Quotient) Bioelectric Impedance Analysis Anthropometric Measurements Physical Activity Monitors Physical Activity Questionnaires Other procedure or activity requested (please explain): 15 3/3/09 Section H. Dental Research: General Oral Health Center The General Oral (GO) Health Center is the CTRC dental clinical research facility. This clinic is located in 2040 Old Dental Building at the UNC School of Dentistry. Research protocols involving dental faculty and/or research subjects having dental procedures may utilize this clinic. Clinic Hours: Monday through Friday 8am-5pm, Telephone: 919-966-5271. 1. Do you plan to utilize the GO-Heath Center to conduct some or all of your dental research visits? Yes (please indicate on cost assignment sheet number of visits per subject) No 2. If yes, indicate any equipment or specific supplies required for your protocol. 16 3/3/09 Section I. Specimen Processing Facilities and Specimen Storage The CTRC offers temporary space for investigators to use in storing specimen samples. The Investigator Lab is located in Room 3104 Main Hospital in the CTRC at UNC Hospitals. This lab contains bench space for specimen processing, a hood, shelving and drawer space, and a -20 centigrade freezer. The specimen processing and mailing station in the CTRC at Burnett-Womack is also available to investigators. The site has a large storage area equipped with refrigerator and -80°C freezer for storing biological specimens. 1. Which of the CTRC Specimen Processing Facilities will you utilize? (you may check both) Investigator Lab Room 3104 (CTRC at UNC Hospitals) Specimen processing and mailing station (CTRC at Burnett- Womack) 2. Have personnel who will use these facilities completed UNC EHS safety training (blood borne pathogen, infection control, and/or laboratory safety)? Yes No - Training modules can be found at http://ehs.unc.edu/training/self.shtml 3. Do you plan to utilize laboratory freezers for temporary (< 90 days) sample storage? If yes, indicate preference of freezer location: Investigator Lab Room 3104 (CTRC at UNC Hospitals) Specimen Storage Area (CTRC at Burnett-Womack) 17