Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Blood donation wikipedia , lookup
Autotransfusion wikipedia , lookup
Plateletpheresis wikipedia , lookup
Jehovah's Witnesses and blood transfusions wikipedia , lookup
Men who have sex with men blood donor controversy wikipedia , lookup
Hemolytic-uremic syndrome wikipedia , lookup
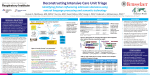
NUCLEATED RED BLOOD CELLS AS AN INDEPENDENT PREDICTOR OF ICU MORTALITY AND ICU RECIDIVISM Mooney, Owen1; Zarychanski, Ryan2; Bell, Dean3; Rimmer, Emily3; Kumar, Anand4; Houston, Don5; Turgeon, Alexis6; Doucette, Steve7 1 University of Manitoba, Department of Internal Medicine/Critical Care, Winnipeg, Canada; 2 University of Manitoba, Department of Hematology and Critical Care, Winnipeg, Canada; 3 University of Manitoba, Department of Anesthesia and Critical Care, Winnipeg, Canada; 3 University of Manitoba, Hematology, Winnipeg, Canada; 4University of Manitoba, Critical Care, Winnipeg, Canada; 5University of Manitoa, Hematology, Winnipeg, Canada; 6Laval University, Anesthesiology and Critical Care, Quebec City, Canada; 7Dalhousie University, Epidemiology, Halifax, Canada Introduction: Since the late 1940’s it has been recognized that the presence of nucleated red blood cells (nRBC’s) in a peripheral blood sample of patients portends a poor outcome. In the absence of certain hematologic conditions, such as sickle-cell disease or thalassemia major, these types of cells a generally absent from peripheral blood. It has been reported that the presence of these cells suggests a severe physiologic stress has been endured. To date, the precise nature of this stress is unclear. Although previously published in observational reports, recent prospectively collected studies confirms that a significant percentage (17-35%) of critically ill patients will have detectable nRBC’s in their peripheral blood at sometime during their illness. The identification of nRBC’s in peripheral blood has not been limited to a single diagnosis or physiologic derangement and has been described in a diverse number of disease states, from congestive heart failure to septicemia. What links these conditions mechanistically with the presence of nRBC’s and why their presence predicts poor outcomes is not understood. Objectives: The objectives of our study were to examine the independent association of nRBCs on ICU mortality. Secondly, we aimed to examine readmission rates of patients who remained nRBC-positive within 24 hours of ICU transfer compared to those patients who where nRBCnegative. Methods: We conducted a retrospective cohort study of patients admitted to tertiary care hospitals in Winnipeg, Canada from January 1st, 2006 to December 31st, 2011. A patient was determined to be ‘nRBC-positive’ if they had detectable levels of nRBCs (>19/ul) at any point during their ICU admission. A ‘nRBC-negative’ patient was defined as any patient who never demonstrated detectable nRBC’s during their ICU admission. Our primary outcome of interest was mortality. The independent prognostic significance of nRBCs was assessed using Cox proportional hazards regression modeling. Results: Of the 9809 admitted patients, 1391 (14%) had circulating nRBCs during their ICU admission. The mean age of the nRBC-positive and negative patients was 60.1 years. Males made up 54.9% of the nRBC-positive group and 64.5% of the nRBC-negative group. The most common diagnosis in the nRBC-positive group was septic shock (39.1%). Patients with nRBCs detected had a higher acuity of illness on admission as defined by APACHE II score (23.8 vs. 16.3). The baseline use of vasopressors (83% vs. 48.9%), and mechanical ventilation (91% vs. 65.3%) were higher in the nRBC-positive group. Baseline acidosis, defined by a blood pH <7.20, occurred more frequently in patients who were nRBC-positive (61.8% vs. 50.7%). In a Cox proportional-hazards model, adjusted for age, sex, APACHE II score, use of vasopressors, mechanical ventilation, acidosis, admission diagnosis, and the use of acute dialysis, the hazard ratio for ICU mortality associated with nRBC positivity was 1.3 (95% CI 1.15-1.48). Readmission rates between patients who remained nRBC positive within 24 hours of ICU transfer was significantly higher, 10% (18/189) vs. 4% (368 /8570) p=0.002. Mortality at 30 days did not differ significantly between those patients who remained positive prior to transfer. References: 1. Groen, J, Godfried G. The occurrence of normoblasts in the peripheral blood in congestive heart failure: an indication of unfavorable prognosis. Blood. 1948; 3: 1445-1452. 2. Swartz, S, Stansbury, F. Significance of Nucleated Red Blood Cells in Peripheral Blood: Analysis of 1496 cases. JAMA. 1954; 154(16): 1339-40. 3.. Stachon A, Bo¨ning A, Krismann M, et al. Prognostic significance of erythroblasts in blood after cardiothoracic surgery. Clin Chem Lab Med. 2001; 39:239 –243. 4.. Stachon A, Bolulu O, Holland-Letz T, Krieg M: Association between nucleated red blood cells in blood and the levels of erythropoietin, interleukin-3, interleukin-6, and interleukin-12p70. Shock 2005; 24:34-39. 5. Stachon, A, Becker A, et al. Reevaluation of Established Risk Scores by Measurement of Nucleated Red Blood Cells in Blood of Surgical Intensive Care Patients. J of Trauma, Injury, Infection, and Critical Care. 2008; 65:666–673. 6. Stachon, A, et al. Nucleated red blood cells in the blood of medical intensive care patients indicate increased mortality risk: a prospective cohort study. Critical Care. 2007; 11:R62 (doi:10.1186/cc5932).