Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
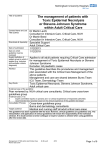
Case presentation Overlap Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: a case report Overlap Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: a case report Overlap Sindrom Stevens Johnson/Necroliza epidermică toxică: prezentare de caz Dr. Radu-Nicolae Grigore(1), A/Prof. Carmen Maria Sălăvăstru(1,2), Prof. Dr. George Sorin Țiplică(1,2) (1) - 2nd Clinic of Dermatology, Colentina Clinical Hospital (2) - University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania Corresponding author: A/Prof. Carmen Maria Sălăvăstru, 2nd Clinic of Dermatology, Colentina Clinical Hospital, Șoseaua Ștefan cel Mare Nr. 19-21, Bucharest, Romania Email: [email protected] Open Access Article Abstract Keywords: Stevens Johnson Syndrome, Toxic Epidermal Necrolysis, Lamotrigine, Overlap SJS / TEN Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but potentially lethal acute dermatologic condition. SJS and TEN can be induced by drugs. We present the case of a 30 year-old woman who was admitted for generalized skin eruption consisting of erythematous, dusky-red macules which evolved to flaccid blisters, painful mucous erosions, conjunctivitis, malaise, fever and chills. Three weeks before admission she started taking Lamotrigine for bilateral temporal arachnoid cysts. Based on the affected body surface area (> 10%, but <30%) the diagnosis was: Overlap SJS/TEN induced by Lamotrigine. The patient was successfully treated with corticosteroids and supportive measures and was discharged after 26 days in good health. The chronic complications that occurred, involved the eyes (entropion, trichiasis) and nails (onychomadesis and nail plate detachment). Rezumat Cuvinte-cheie: Received: August 2014 Accepted: September 2014 Cite this article: Dr. Radu-Nicolae Grigore, A/Prof. Carmen Maria Sălăvăstru, Prof. Dr. George Sorin Țiplică, Overlap Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: a case report. RoJCED 2014; 1(1):28-31. 28 Sindrom Stevens Johnson, necroliză epidermică toxică, lamotrigină, overlap SJS / TEN Sindromul Stevens-Johnson (SJS) şi necroliza epidermică toxică (TEN) sunt afecţiuni dermatologice rare, acute şi cu potenţial letal. SJS şi TEN pot fi induse de medicamente. Prezentăm cazul unei femei în vârstă de 30 de ani care a fost internată pentru o erupție cutanată generalizată constituită din macule roșii-violacee pe care s-au dezvoltat bule flasce, eroziuni mucoase dureroase, conjunctivită, stare generală alterată, febră și frisoane. Cu 3 săptămâni înaintea internării pacienta a început tratament cu Lamotrigină pentru chisturi arahnoidiene temporale bilaterale. A fost stabilit diagnosticul Overlap SJS/TEN indus de Lamotrigină datorită suprafeței corporale afectate mai mare de 10%, dar mai mică de 30%. Pacienta a fost tratată cu succes folosind terapia cu corticosteroizi și măsuri suportive și a fost externată după 26 de zile cu stare generală bună. Singurele complicații cronice au fost afectarea oculară (entropion și trichiazis) și unghială (onicomadeză). R O M A N I A N J O U R N A L o f C L I N I CA L a n d E X P E R I M E N TA L D E R M ATO LO GY Radu-Nicolae Grigore, Carmen Maria Sălăvăstru, George Sorin Țiplică Introduction Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but potentially lethal acute adverse drug reactions, characterized by erythema and epidermal detachment of the skin and mucous membranes. They are estimated to occur in 1–3people/million/year in Europe and the USA(1, 2). They are characterized by a low incidence but high mortality, and drugs are most commonly implicated in 80% of cases(3, 4). The most common triggers are antibiotics, nonsteroidal anti-inflammatory drugs and anticonvulsants. Symptoms usually occur within 1–3 weeks after the first drug intake. Pathophysiology of the disease is characterized by cytotoxic T-lymphocytes and other cytokine pathways which cause keratinocyte apoptosis(5). It presents clinically with cutaneous purpuric macules disseminated over the trunk and limbs and characteristic periorificial purpuric macular lesions covered by hematic crusts. Oral mucosa is affected (painful erosions covered by membranes) and also conjunctivitis can be present. The skin lesions progress to superficial (epidermal) necrosis. A positive Nikolsky sign can be elicited, and the skin resembles wet cigarette paper when detached(6). The SJS and TEN are considered the same disease process; the distinction is made based on body surface area involvement. The SJS is characterized by <10% of the body surface area of epidermal detachment, SJS/TEN overlap by 10–30%, and TEN by >30%(7). The SCORTEN level(7) is used to predict disease severity and mortality, and is calculated within 24 hours of admission and on day 3. The score is the sum of 7 variables, each contributing 1 point, including the following: (1) Age > 40 years; (2) Heart rate > 120 beats per minute; (3) Positive cancer history; (4) Epidermal detachment > 10% body area; (5) Blood urea nitrogen > 28 mg/dL; (6) Glucose > 252 mg/dL; (7) Bicarbonate < 20 mEq/L. A score of 2 or less is associated with a maximum of 12% mortality; a score of 4 predicts 58% mortality, and a score of 5 or more is predictor for a 90% death rate(8). SJS/TEN positive diagnosis relies on clinical symptoms and on histological features: full thickness epidermal necrolysis due to extensive keratinocyte apoptosis(9). Differential diagnosis includes Erithema multiforme major, Acute generalized exanthematous pustulosis, Generalized bullous fixed drug eruption, Thermal burns, Chemical burns, Phototoxic reactions, Paraneoplastic pemphigus and Staphylococcal scalded skin syndrome. Several therapies have been proposed, with contradictory results. Currently, intravenous immunoglobulins (IVIG) and plasmapheresis are considered most effective(10, 11). Corticosteroids are Figure 1. The skin lesions at admission to hospital: 9% of body surface area was involved. Note the “atypical target” aspect that the lesions presented effective if administered within 72 h from the onset of first symptoms(12). The use of Cyclosporine A was associated with lower levels of hepatic, renal and cardiac injury and lower mortality(13). Despite the increased knowledge regarding the immunological aspects, only prompt withdrawal of suspect medication and general management of the patient as a burn patient are the only evidencebased therapies(14,15). Case report A 30 year old non-smoker female patient presented with generalized skin eruption consisting of erythematous, dusky-red macules which evolved to flaccid blisters, painful mucous erosions, conjunctivitis affecting both eyes, malaise, fever and chills. The patient had no history of allergies and was diagnosed 6 months before admission with bilateral temporal arachnoid cysts (right one 15/19/10 mm, left one 32/31/23 mm). The patient was on Valproic acid 1000 mg/ day for the past 6 months (for chronic headache induced by the arachnoid cysts). Three weeks before admission her neurologist decided to replace Valproic acid with Lamotrigine 25 mg/day with progressive increase of dosage, because the patient was willing to obtain a pregnancy. One week before symptoms began, the patient was on a 50 mg of Lamotrigine/day dose. Symptomatology began 2 days before admission and she was treated as outpatient with antihistaminics and intravenous Hydrocortisone hemisuccinate. The clinical examination revealed fever (39.1oC) and slight tachycardia (100 beats/minute). Examination of the skin and mucous membranes revealed generalized skin eruption consisting of erythematous, dusky-red, irregularly shaped macules, with symmetrical distribution, atypical target lesions with dark center, which evolve to flaccid blisters (with 9% of BSA that presented a October 2014 29 Case presentation Overlap Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: a case report Figure 2. Patient in the 10th day of admission: 27% of body surface area was involved positive Nikolsky sign at admission (Figure 1). On face, neck, palms and soles the lesions tended to coalesce. The patient had erosions, grayish-white pseudomembranes on the surface of the lips, oral cavity and tongue erosions. Both eyes were affected by conjunctival hyperemia, grey-yellow adherent pseudomembranes. Genital erosions were also present. All the skin and mucous lesions were extremely painful. Lab tests at admission showed hiperglycaemia – 152 mg/dl, slightly elevated liver enzymes, slight lymphopenia and thrombocytopenia. The patient was treated with corticosteroids in high doses for the first three days (1 g/day), then the dosage was tapered. Antipyretics, antibiotics, anticoagulants, fluid replacement solutions, diuretics and vitamins were also used. The patient was fed with standardized solutions with high calories count (1 mL = 1 kcal). Lamotrigine was excluded from the patient’s treatment scheme and Acetaminophen was used instead for the patient’s headaches. Topical treatment with antiseptics, colloidal silver cream, corticosteroids and biomembrane dressings were used for the skin lesions. Mucous lesions were treated with antibiotics and corticosteroids. Blood pressure, pulse, body temperature and renal function were closely monitored and the patient was seen by an Ophthalmologist every day. New lesions continued to appear during the first 10 days of admission. Older lesions followed their course leaving massive areas of skin denudated. 30 By day ten 27% of BSA was affected (Figure 2). Mucous membranes became more and more affected, causing difficulty to eat and breath. The patient was able to open the eyes with great effort. Fever ceased after the 5th day of admission. The laboratory tests showed: leucopenia, neutropenia and thrombocytopenia, elevated liver enzymes (4x normal values), anemia (HGB – 9.52g/dL), hyperglycemia (maximum value 195 mg/dL), hypoalbuminemia (lowest value 2.52 g/ dL), hypoproteinemia (lowest value 4.28 g/dL) and hypokalemia (lowest value 3.01 mmol/L). Treatment was supplemented with human albumin and potassium. Urea and creatinine had normal values during the hospitalization. SCORTEN in the 3rd day after admission was 1 (BSA=11%) and stayed the same during admission period. Predicted mortality based on SCORTEN was 3.2%. No new lesions occurred after the 10th day, the areas of skin which were denudated began to heal (Figure 3), the mucous membrane lesions healed at a lower pace than the skin lesions and the lab test results slowly returned to normal values. Her headaches were easily controlled with acetaminophen during hospitalization. Discussions Anti-epileptic drugs can be associated with a wide spectrum of cutaneous adverse reactions. These rashes are well documented with older antiepileptic drugs like phenytoin, phenobarbital and carbamazapine. Lamotrigine is a newer antiepileptic drug used in the treatment of partial and generalized seizures and as maintenance treatment of bipolar I disorder(16, 17). It is known to cause skin rashes in 3-10% of new users(18). Several factors are likely to increase the development of serious rashes. Coadministration of valproic acid with lamotrigine significantly increases the risk for development of serious adverse cutaneous reactions(19). It has been hypothesized that valproic acid interacts with lamotrigine by inhibiting its hepatic inactivation. The elimination half life of lamotrigine when used as monotherapy is 25-30 hours and it is more than doubled to 60 hours when combined with valproic acid(20,21). It has also been suggested that a high starting dose and a rapid dose escalation may increase the occurrence of skin rashes with lamotrigine(19,21). Severe cutaneous reactions to antiepileptic drugs are more frequently associated with female sex, probably due to hormonal factors(22). The skin lesions in SJS/TEN are similar to seconddegree burns(3) and lead to extreme pain, massive loss of fluid and protein, bleeding, evaporative heat loss with subsequent hypothermia, and infection. Our patient didn’t suffer an infection of the cutaneous lesions, thus the prognosis R O M A N I A N J O U R N A L o f C L I N I CA L a n d E X P E R I M E N TA L D E R M ATO LO GY Radu-Nicolae Grigore, Carmen Maria Sălăvăstru, George Sorin Țiplică remained favorable. She did suffer tough a massive loss of fluid and proteins that required prompt intervention. She received important quantities of replenishment fluids, electrolytes and human albumin. A patient with TEN is suffering from “acute skin failure” and the condition can be complicated by major metabolic abnormalities, sepsis, multi-organ failure, pulmonary embolism and gastrointestinal hemorrhage(23). Our patient did not suffer any of those complications. Apart of the acute complications, SJS/TEN patients can develop long term complications: late ophthalmic complications (synblepharon, corneal ulcerations, ectropion, entropion, trichiasis, dryness of the eye), postinflamatory skin hypo/ hyperpigmentation, nail plate abnormalities, genital complications (dyspareunia, dryness, pain, bleeding, adhesions), post traumatic stress disorder. At a follow-up visit one month after checkup the patient had disseminated hyperpigmented macular lesions, onychomadesis, entropion, trichiasis and dry eyes. At the two months followup visit the main complaints of the patient were eye dryness, entropion and trichiasis. New nail plates were growing normally on all fingers. The patient had no episode of headache that couldn’t be controlled by using acetaminophen during those two months after discharge. Conclusions Skin failure can be induced by antiepileptic drugs. Lamotrigine or lamotrigine potentiated by previous chronic intake of valproic acid Figure 3. Patient in the 15th day of admission (left image) versus the 26th day of admission (right image) was the inducer of the SJS/TEN overlap in our patient. The avoidance of skin supra-infection and the iv support (albumin, potassium) were essential in the recovery of the patient. This work is licensed under a Creative Commons Attribution 4 .0 Unported License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc/4.0/ Bibliography 1) Fritsch PO, Sidoroff A. Drug-induced Stevens-Johnson syndrome/toxic epidermal necrolysis. Am J Clin Dermatol., 2000, 1(6): 349–360. 2) Harrand T, French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis, 2010, 5 (1):39. 3) Palmieri TL, Greenhalgh DG, Saffleetal JR. A multicenter review of toxic epidermal necrolysis treated in U.S. burn centers at the end of the twentieth century. J Burn Care Rehabil, 2002, 23(2): 87–96. 4 Kim HI, Kim SW, Park GY et al. Causes and treatment outcomes of StevensJohnson syndrome and toxic epidermal necrolysis in 82 adult patients. Korean J Intern Med, 2012, 27(2): 203–210. 5) Heyea P, Desclouxa A, Singerb G, Rosenberga R, Kochera T. Perforated Sigmoid Diverticulitis in the Presence of Toxic Epidermal Necrolysis. Case Rep Dermatol, 2014, 6: 49–53. 6) French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome: our current understanding. Allergol Int, 2006, 55: 9–16. 7) Roujeau JC. Stevens-Johnson syndrome and toxic epidermal necrolysis are severity variants of the same disease which differs from erytema multiforme. J Dermatol, 1997, 24:726-9. 8) Guegan S, Bastuji-Garin S, Poszepczynska-Guigne E, Roujeau JC, Revuz J. Performance of the SCORTEN during the first five days of hospitalization to predict the prognosis of epidermal necrolysis. J Invest Dermatol, 2006, 126(2):272-6. 9) Moitra S, Sen S, Banerjee I, Das P, Tripathi SK. Diclofenac-serratiopeptidase combination induced Stevens - Johnson Syndrome - a rare case report with review of literature. J Clin Diagn Res. 2014, Vol-8: 8-11 10) Fromowitz JS, Ramos-Caro FA, Flowers FP. Practical guidelines for the management of toxic epidermal necrolysis and Stevens-Johnson syndrome. Int J Dermatol 2007; 46: 1092-4. 11) Knowles S, Shear NH. Clinical risk management of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis spectrum. Dermatol Ther 2009; 22: 441-51. 12) Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis: Part II. Prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol 2013; 69: 187.e1-6. 13) Arevalo JM, Lorente JA, Gonzales-Herrada C. Treatment of toxic epidermal necrolysis with cyclosporine. A. J Trauma 2000; 48: 473-8. 14) Downey A, Jackson C, Harun N, Cooper A. Toxic epidermal necrolysis: review of pathogenesis and management. J Am Acad Dermatol,2012, 66 (6):995–1003. 15) Lissia M, Mulas P, Bulla A, Rubino C. Toxic Epidermal Necrolysis (Lyell’s disease). Burns, 2010, 36 (2): 152–163. 16) Dichter MA, Brodie MJ. New antiepileptic drugs. N Engl J Med. 1996;334:1583–90. 17) Keck PE, Jr, McElroy SL, Strakowski SM. Anticonvulsants and antiepileptics in the treatment of bipolar disease. J Clin Psychiatr. 1998;59(suppl 6):74–81. 18) Sukhjot K, Alka D. Toxic Epidermal Necrolysis due to concomitant use of Lamotrigine and Valproic Acid. Indian J Dermatol, 2013, 58(5): 406. 19) Hirsch LJ, Weintraub DB, Buchsbaum R et al. Predictors of Lamotrigineassociated rash. Epilepsia. 2006;47:318–22. 20) Patsalos PN, Bourgeois BFD. The Epilepsy Prescribers Guide to Antiepileptic Drugs 1st ed. Cambridge: Cambridge University Press; 2010. Lamotrigine. 111– 23. 21) Guberman AH, Besag FM, Brodie MJ, et al. Lamotrigine-associated rash: Risk/ benefit considerations in adults and children. Epilepsia. 1999;40:985–91. 22) Alvestad S, Lydersen S, Brodtkorb E. Rash from antiepileptic drugs: Influence by gender, age, and learning disability. Epilepsia. 2007;48:1360–5. 23) Pereira FA, Mudgil AV, Rosmarin DM. Toxic epidermal necrolysis, J Am Acad Dermatol, 2007, 56 (2): 181–200. October 2014 31