Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Pharmacognosy wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
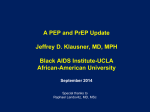
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
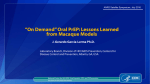
Pharmacogenomics wikipedia , lookup
HIV vaccine wikipedia , lookup
Iniciativa PrEx PrEP Initiative Introduction to the PREP concept Javier R. Lama, MD, MPH Robert M. Grant, MD, MPH 1 Management of genital infections (STIs) Microbicides Cervical Barriers HIV PREVENTION Condoms Behavioral Counseling and Testing Vaccines HSV-2 Suppressive therapy Male circumcision Chemoprophylaxis MTCTP PEP PrEP 2 Prevention Disappointments • Trials showing no efficacy or harm… – – – – – – Intensive counseling in MSM (Koblin Lancet 2004) Microbicides: N-9/Savvy/Cellulose Sulfate Diaphragms (Padian Lancet 2007) Mass STI treatment (Wawer Lancet 1999) Herpes suppression (Celum CROI 2008) An adenovirus-vectored vaccine (Buchbinder CROI 2008) 3 Male circumcision Condoms Behavioral Counseling and Testing (Intensive not better than standard) HIV PREVENTION (Not known to be helpful for men who have sex with men) Chemoprophylaxis MTCTP (PEP PrEP have unknown efficacy) 4 PrEP Goes Back to Basics • HIV Infection is The Cause of AIDS – Not Sex, Not Drugs – Antiretroviral Agents Target HIV Directly • People Like Sex – For Pleasure, Intimacy, Company, Livelihood, – and Pregnancy.... – Prevention is less used if it alters sex • Abstinence Programs, Condoms, Diaphragm. • Microbicides? • Male circumcision? 5 Why Chemoprophylaxis? • Anti-HIV Drugs – Inhibit HIV directly – Are already formulated and mass produced – Prevent mother to child transmission • A pill is at least as female controlled as a topical microbicide • Chemoprophylaxis is a proven concept – EG: Malaria, TB pneumonia, meningitis – A mainstay of prevention if no vaccine 6 Why Pre-exposure? • Pre-exposure dosing increases efficacy – SHIV exposed nonhuman primates (Garcia Lerma 2008) • People have difficulty recognizing exposure – Denial (Schechter JAIDS 2004) – Substance use – Imperfect communication with partners • For those at highest risk – Pre- and post-exposure periods overlap 7 Why FTC/TDF? 8 Some Chemoprophylactic Agents Zidovudine Therapy year licensed 1987 Lamivudine 1995 Nevirapine Tenofovir 1996 2001 Emtricitabine 2003 Entry Inhibitors 1st in 2007 Integrase Inhibitors 1st in 2007 Prevention Indications MTCTp PEP MTCTp PEP MTCTp PEP Oral PrEP Microbicide MTCTp PEP Oral PrEP PrEP Microbicide TBD Status licensed used used used efficacy shown used phase II/III phase II/III safety used phase II/III primates primates TBD 9 FTC and TDF have Long Intracellular Half Life Approved as BID Approved as QD or BID Approved Approved Approved as QD or BID as QD or BID as QD or BID 50 Approved as QD ** >60 45 40 T1/2 (hours) Approved as QD 35 30 25 20 24 hours ‡ * 15 10 5 12 hours § * 0 ZDV d4T ABC 3TC Serum/Plasma half-life †Data ddI TDF FTC Intracellular half-life from Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51(RR-7):1-64 unless otherwise noted 10 *Anderson et al. AIDS 2003; 17(15):2159-2168. ‡Piliero et al. 43rd ICAAC, Chicago, 2003. ** Hawkins et al. 5th IWCPHT, Rome, 2004 § Wang et al. IAC, 2002, poster #4546. Drug Exposure in the Male Genital Tract Percent of Blood Plasma Levels Kashuba et al. and CROI 13 Abstract 569 (Vourvahis), 13th CROI Abstracts 396 (Stekler), Abstract 618 (Katzenstein) 0 50% 100% APV (20%) NVP (70%) ENF (ND) 150% ABC (150%) 200% 500% ZDV (200%) TDF (500%) 600% 3TC (600%) IDV (100%) d4T (2%) EFV (3%) SQV (3%) RTV (3%) LPV (5%) NFV (5%) 11 NRTI PI NNRTI FI Mitochondrial DNA Depletion DDI>DDC>D4T>AZT>Abacavir = 3TC = TDF (Birkus, Hitchcock, Cihlar. Antimicrob Agents Chemother 2002) 12 Preclinical Evaluation of Tenofovir (TDF) + Emtricitabine (FTC) • Either FTC or TDF were protective – 70% to 100% Effective • Emtricitabine + Tenofovir – The combination was 100% effective – Even after repeated rectal exposures (14) – Even if given once prior to exposure, and once after • Protection probably reflects – High concentrations in genital tissues and fluids – Long intracellular half life – Activity in Macrophages Tsai ‘95; Van Rompay ‘99 ‘00 ‘01 ‘04; Subbarao ’05; Heneine’06 ‘07 ‘08 13 FTC/TDF Toxicity Concerns • TDF – Few Case Reports of Renal Failure • Risk Factors: Small Body Size, Overdosage, Concomitant use of DDI or Kaletra – Headache, Dizziness, Cramps, Flatulence, – Small changes in bone density in HIV positives • FTC – Skin or nail discoloration (0-8%; blacks>>latinos>whites) – Never severe; does not lead to stopping medications • Both – HBV flare in those stopping • Risk Factors: baseline cirrhosis, baseline transaminitis, HBeAg+ – Lactic Acidosis? • All case reports involve other drugs as well (especially D4T or DDI) • Monitor Anion Gap and Total CO2 – Drug Resistance 14 2007 • Conducted between June 2004 and March 2006 • West Africa • Daily dose of 300 mg oral Tenofovir DF vs. placebo • All participants received testing, condoms, and counseling. • Safety evaluated in N=936 including 428 person years 15 Findings From the West African PREP Study • Safety in seronegatives confirmed – No increase in grade 1 renal abnormalities – No grade 2 or greater renal toxicity – No flares among 23 known to be HBsAg+ • A trend toward efficacy – 8 seroconversions (2 TDF: 6 Placebo; P=0.34) – 2 seroconversions after 1 and 2 months of TDF • No specimens to Rule Out Pre-PREP infection • No bona fide case of PREP failure yet documented Peterson, Plos Clinical Trials, 2007 16 The iPrEx Study: Safety, Efficacy, Behavior, and Biology Sponsored by NIH/NIAID/DAIDS with co-funding by the Bill and Melinda Gates Foundation and drug donated by Gilead Sciences 17 The iPrEx Study: Safety, Efficacy, Behavior, and Biology Gladstone Institute of Virology and Immunology 18 19 The iPrEx Study • • • • Plans to Enroll 3000 High Risk MSM Randomized 1:1 Daily Oral PREP FTC/TDF vs Placebo Followed on Drug for: – – – – – – – HIV seroconversion Adverse Events (especially renal & liver) Metabolic Effects (Bone, Fat, Lipids) HBV Flares among HBsAg+ Risk Behavior & STIs Adherence If infected • Drug Resistance • Viral load • Immune responses & CD4 Count 20 Why MSM? “We Love You… Be Part of Something Big” INMENSA, Peru 21 Why MSM? • From 2002 to 2004, – The PREP Agenda Did Not Include MSM • MSM Bear a Major Burden of the Epidemic – Throughout the Americas – In At Least Some Parts of Asia – The Burden in Africa Is Increasingly Appreciated • Efficacy Could Be Different After Rectal Exposure – Higher Efficiency of Transmission – Possibly Different Tissue Penetration of Virus and Drug • iPrEx is Still The Only Efficacy Study in MSM 22 “Let’s Communicate” From February 2004, the iPrEx study communicated with participants, activists, government, sponsors, physicians… 23 Lessons Learned • Ethical Discussions Focus on – – – – Autonomy if rich Benefits if poor Poverty impinges on autonomy EG: Visit Reimbursement Rates • Poor People Want More • Risk Compensation or “Dis-inhibition” – Major concern for straight-appearing gay men – Not mentioned by travesties and others • Fragile communities rely on delicate practices for generating income, resisting violence, and maintaining health – Any Change is Frightening. 24 After 3 Years of Preparation, iPrEx is Enrolling on Schedule 800 700 Enrollment 600 500 400 300 200 100 0 Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar07 07 07 07 07 07 07 08 08 08 25 Ju n0 Se 7 pDe 0 7 cM 07 ar -0 Ju 8 n0 Se 8 pDe 0 8 cM 08 ar Ju 09 n0 Se 9 pDe 0 9 cM 09 ar -1 Ju 0 n1 Se 0 pDe 1 0 c10 Enrollment Planned iPrEx Enrollment 3500 3000 2500 2000 1500 1000 500 0 26 Why Was iPrEx Expanded? • To Provide Power to Detect Cost-Effective Levels of Efficacy – Cost Effective if >60% Efficacy – Not Cost Effective if <30% Efficacy – Efficacy in Practice < Efficacy in Trials Grant et al, IAS Meeting, Toronto 2006 27 Future Optimization • Requires Non-Inferiority Margins – Minimal Evidence of Efficacy From A Single “Proof of Concept” Trial Could Hinder Future Optimization • Optimizing The Regimen – To Minimize Toxicity, Resistance and Costs • Optimizing Dosing Route and Interval – To Maximize Convenience and Efficacy 28 Adherence • Measured by – CASI (quarterly) – Self Report to Counselor (monthly) – Pill Count • Improves After First On-Drug Visit • Individualized Counseling Strategies Used – People Go From Pharmacy to Counseling • Periodic Blinded Drug Levels 29 The Importance of CASI • PREP is a Behavioral Intervention – Requires Adherence – Could Alter Risk Behavior • Behavior is Complicated – Especially Sexual Behavior – Numbers of partners, types of partners, practices with each partner 30 Other Possible Effects of PEP/PREP • Encourages People to PREPare for Sex. – Take Protection Along. – Have The Safe Sex Talk Early. • Serves As A Reminder Of Risk. – Foster A Vision For An AIDS-free Life. – Investment In Future Health. • Builds Stronger Communities. – Bridge Across Positive And Negative Factions. – De-stigmatize “At Risk” and infected groups. • Stabilizes Sexual Relationships. – By Protecting Those Drawn To Positive Persons. – By Protecting Those Desiring Pregnancy. 31 The Importance of CASI • Measures Drug Exposure • Measure Sexual Behavior – Numbers of Partners – Types of Partners – Activities with Each Type of Partner 32 Drug Resistance • Standard Population Genotype • Standard Population Phenotype • Allele Specific PCR for Mutations – Using a ultra-selective enzyme – And mutation specific primers – TDF: K65R, K70E – FTC: M184I/V, K65R 33 Will Chemoprophylaxis Have Immunological Benefits? PBMCs are for immunological and virological substudies led by Douglas Nixon, Oscar Guerra, Esper Kallas, Robert Grant Viral antigen exposure during chemoprophylaxis may induce antiviral immune responses that could provide future protection, or, attenuate the course of infection among seroconverters. 34 Minimum Effective Concentration of PREP Agents • The Best We Surrogate Marker of Protection We Could Have • PBMC Concentrations Reflect Longer Term Exposure • Yet Another Reason PBMC Collection is Very Important in iPrEx 35 “…Señor Ministro de Salud: ¿qué hacer? ¡Ah! desgraciadamente, hombres humanos, hay, hermanos, muchísimo que hacer!” LOS NUEVE MONSTRUOS César Vallejo, 1939 THE NINE MONSTERS “… Mr. Minister of Health: What to do? 36 Ay, unfortunately, fellow humans, there is, brothers, so much to do!”