Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
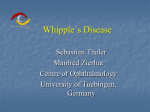
Q J Med 1997; 90:765-772 Whipple's disease without malabsorption: new atypical features S.A. MISBAH, B. OZOLS\ A. FRANKS2 and N. MAPSTONE1 From the Departments of Chemical Pathology and Immunology, ^Molecular Pathology and Neuropathology, Institute of Pathology, Leeds General Infirmary, Leeds, UK 2 Received 5 September 1997 Summary The diagnosis of Whipple's disease in the absence of intestinal involvement is difficult and often overlooked. We describe five patients aged 8-71 years with normal jejunal biopsies and disparate clinical features, previously unrecognized in Whipple's; all were investigated at a single institution over a period of 18 months. Routine histological examination for periodic acid-Schiff (PAS) positive macrophages and polymerase chain reaction (PCR) analysis for Tropheryma whippelii was performed on the small intestine in all patients. PCR analysis was also performed on various tissues including peripheral blood, lymph node, muscle, synovium and spleen in individual patients. Patients 1, 2, 4 and 5 had unusual presenting features not previously associ- ated with Whipple's: intractable immune thrombocytopenic purpura (ITP), juvenile chronic arthritis, isolated muscle weakness and quadriparesis, respectively. Patient 3 presented with pyrexia of unknown origin. All patients had histologically normal small-bowel biopsies with no evidence of PAS positive macrophages. PCR for T. whippelii was positive in all patients in one or more tissues: peripheral blood, intestine, muscle, lymph node and synovium. PAS-positive macrophages were found in 4/5 patients in various sites: lymph node, muscle, spinal cord. Whipple's disease presents with protean clinical features and should be considered in granulomatous disorders of unknown aetiology even in the absence of gastrointestinal involvement. Introduction The diagnosis of Whipple's disease has traditionally depended on the demonstration of diastase-resistant periodic-acid-Schiff (PAS)-positive macrophages in the small bowel of patients presenting with malabsorption and associated systemic features such as fever, lymphadenopathy, arthritis, uveitis and neurological involvement.1 While rare cases of Whipple's disease without obvious intestinal involvement were recognized before the availability of the polymerase chain reaction (PCR),2"6 this aspect of the disease has received little attention. The recent identification of the Whipple's bacillus, Tropheryma whippelii7'8 and the consequent development of diagnostic PCR has led to the description of further cases of Whipple's disease presenting without gastrointestinal features. Recent case reports have drawn attention to purely neurological and ocular cases, which in the absence of PCR are likely to have been misdiagnosed.9'10 We describe a further five patients with Whipple's disease presenting with disparate atypical clinical features without gastrointestinal involvement over a period of 18 months, that emphasize the protean features of this disorder and the role of PCR in diagnosis. Case histories Patient 1 A 22-year-old builder presented with fatigue, hepatosplenomegaly, night sweats, lymphadenopathy (abdominal and supraclavicular), and fever in Address correspondence to Dr S.A. Misbah, Department of Chemical Pathology and Immunology, Institute of Pathology, Leeds General Infirmary, Great George Street, Leeds LSI 3EX © Oxford University Press 1997 766 S.A. Misbah et al. September 1991. A lymph-node biopsy revealed multiple granulomata. In December 1991, he underwent laparotomy on account of continuing fever and abdominal pain. Multiple granulomas were demonstrated in the para-aortic nodes. In February 1992, a diagnostic splenectomy and further lymph-node biopsies were performed. Multiple granulomas were again noted in the spleen and lymph nodes. The presence of a Gram-positive rod was noted on splenic histology but cultures were sterile. Stains for fungi, mycobacteria and PCR for M. tuberculosis were negative. In April 1992, empirical treatment with tetracycline was undertaken in view of continuing fever and sweats, on the premise of a bacterial aetiology for his illness. For the duration of tetracycline therapy (6 months) he remained well, being able to return to work. Marked thrombocytopenia (platelet count 5 x 109/l) developed in May 1993, with resultant epistaxis. Bone-marrow biopsy revealed megakaryocytic hyperplasia with numerous granulomas. Between May 1993 and June 1995, he had eight episodes of profound thrombocytopenia requiring high-dose corticosteroids. In June 1995, an immunological opinion was requested. A diagnosis of Whipple's disease was considered at this stage, in view of the history of fever, granulomatous lymphadenopathy, the presence of an unculturable Grampositive rod on splenic histology, and previous clinical response to tetracycline therapy. PCR for T. whippelii (details of assay described below) was positive on peripheral blood, duodenum (despite no histological abnormality) and sections of stored spleen. Serology for cat-scratch disease was negative. Sarcoidosis was considered unlikely on the basis of a normal serum angiotensin-converting enzyme (104 U/l; NR 50-125) and a clear chest X-ray. Review of his original lymph-node biopsies showed PAS-positive macrophages. Immunological investigations revealed lgG-2 subclass deficiency associated with sub-optimal responses to test immunization with 23 valent pneumococcal polysaccharide but normal responses to tetanus and diphtheria toxoids. Reduction of nitroblue tetrazolium (NBT) by the patient's granulocytes was normal. During a 9-month course of oral cotrimoxazole, there was no obvious change in his well-being with three further episodes of marked thrombocytopenia and severe autoimmune haemolytic anaemia in September 1995, necessitating the use of high-dose steroids. He remained PCR-positive for T. whippelii in peripheral blood and duodenum throughout this period. Despite feeling well from January 1996, cotrimoxazole was replaced by a 7-month course of clarithromycin (500 mg b.d. for two weeks followed by 250 mg b.d. maintenance therapy) in March 1996 in view of persistent PCR positivity. Four weeks after clarithromycin treatment he was noted to be PCR- negative on peripheral blood for the first time, and able to undertake regular physical work. On review in August 1997, he was free of systemic symptoms but remains on low-dose steroids for ITP. His lgG-2 subclass deficiency worsened during the period June 1995 to July 1996 (0.77 to 0.23 g/l; reference range 1.2-6.6) but was not accompanied by bacterial infection. Since January 1997, however, lgG-2 subclass levels have steadily improved to 1.01 g/l. Patient 2 A 14-month-old baby girl presented in December 1987 with lymphadenopathy, hepatosplenomegaly, rash and a raised ESR. A provisional diagnosis of systemic Still's disease was made. Her subsequent course was characterized by recurrent arthritis of her knees and elbow joints associated with recurrent upper respiratory tract infection and an episode of orbital cellulitis in March 1991. In July 1992, she underwent laparotomy for intestinal obstruction. Numerous granulomas were noted in abdominal lymph nodes, and her appendix was removed at that time. Stains for acid-fast bacilli and fungi were negative. Immunological investigations revealed a polyclonally raised serum IgA but no evidence of primary antibody deficiency, chronic granulomatous disease or complement deficiency. In October 1995, following the diagnosis in patient 1, the possibility of Whipple's disease accounting for her unexplained arthropathy, periodic fever and lymph node granulomas was considered. PCR on peripheral blood, synovial and duodenal biopsies was positive for T. whippelii. Both duodenal and synovial biopsies were histologically normal. Review of the lymph-node biopsy from July 1992 did not reveal PAS-positive macrophages. Since commencing treatment with cotrimoxazole, steady clinical improvement with a decrease in the frequency and severity of flares was noted, accompanied by PCR negativity on peripheral blood. Patient 3 A 38-year-old man presented in May 1996 with a four-week history of lethargy, fever, myalgia and night sweats. An abdominal CT scan revealed marked para-aortic lymphadenopathy and splenomegaly. An abdominal lymph node biopsy obtained at diagnostic laparotomy revealed massive sinus expansion with large numbers of PAS positive macrophages. A jejunal biopsy revealed normal villous architecture with no evidence of PAS-positive macrophages, while a muscle biopsy showed mild non-specific myopathic changes. As with cases 1 and 2, PCR for T. whippelii was positive on histologically normal intestine. PCR analysis of peripheral blood and lymph node was Atypical Whipple's disease negative. Serology for brucellosis, mycoplasma, human immunodeficiency virus infection, Lyme disease and toxoplasmosis was negative. Treatment with oral cotrimoxazole was terminated after a week due to the development of an allergic rash. Tetracycline treatment led to rapid resolution of symptoms enabling him to resume his hobby of fell running. Patient 4 A 72-year-old female presented in September 1995 with a 2-year history of painful, bilateral muscle weakness associated with persistent sweating. On a presumptive diagnosis of polymyalgia rheumatica, steroid therapy had been started, but in view of progressive muscle weakness and loss of mobility, a muscle biopsy was performed. At the time she was only able to walk a distance of 200 yards, due to the pain in her legs. The muscle showed moderate variation in fibre diameters, but no evidence of interstitial inflammation, fibre necrosis or vasculitis. Focal endomysial and perimysial infiltrates of macrophages were noted around areas of myotendinous insertion (Figure 1); these contained granules that were PAS-positive but negative with Gram, Giemsa, Ziehl-Neilsen and desmin stains. PCR for T. whippelii on fresh frozen muscle was positive. Electron microscopy of reprocessed paraffin sections of muscle 767 showed the macrophage granules to consist of numerous aggregates of irregular fibrillar, dense material with occasional intact bacilliform structures. The patient denied any gastrointestinal symptoms, and no evidence of malabsorption was found on investigation. A duodenal biopsy was normal, with neither villous atrophy nor PAS positive macrophages. Oral cotrimoxazole was commenced, leading to substantial clinical improvement and resumption of normal daily activities. At follow-up 6 months later she had resumed competitive bowling. In view of her steady clinical improvement, cotrimoxazole therapy was stopped at 14 months. Patient 5 A 62-year-old, previously-well, female had a 7-week history of neck pain with paraesthesiae in arms and legs progressing to weakness due to a spastic quadriparesis with muscle strength of MRC grade 4 in the upper limbs and grade 2 in both lower limbs. All laboratory investigations, including CSF analysis were normal; oligoclonal bands were not detected. An MRI scan showed a high signal lesion in medulla and cervical spinal cord, but no supratentorial lesions. Empirical treatment with 12 mg dexamethasone daily was commenced but, despite an initial response, her symptoms progressed, and after a repeat MRI had shown extension of the cord lesion Figure 1. Muscle biopsy in patient 4, showing numerous interstitial macrophages filled with PAS-positive granules. Periodic Acid-Schiff stain, x 320. 768 S.A. Misbah et al. from C3 to T2 level, a spinal-cord biopsy was undertaken. This showed a widespread interstitial infiltrate of foamy macrophages in which PAS- and methenamine silver (Grocott)-positive bacilliform structures were plentiful. A presumptive diagnosis of Whipple's disease was made and a subsequent jejunal biopsy, although morphologically normal, was positive on PCR testing for T. whippelii. Review of her history revealed no gastrointestinal or systemic symptoms. She was treated initially with a combination of intramuscular streptomycin and oral cotrimoxazole. Cotrimoxazole was discontinued on account of a drug eruption, and was replaced by intravenous benzylpenicillin for 2 weeks followed by maintenance oral penicillin. Her subsequent course was complicated by a traumatic fracture of the femoral neck necessitating arthroplasty. At her latest follow-up, she was ambulant with a frame, and able to feed herself while continuing to show improvement in upper and lower limb function. Table 1 summarizes the key clinical features in these five patients. Methods Polymerase chain reaction Fresh tissue specimens were subjected to standard DNA extraction with proteinase K digestion and phenol chloroform purification, followed by DNA precipitation. Aliquots of 1 JLXI were then subjected to PCR following the protocol of Relman et al.8 Specifically, the primers used were pW3FE and pW2RB producing a 284 bp PCR product. The resulting samples were then examined under ultraviolet light following ethidium bromide staining and agarose gel electrophoresis, and a positive result confirmed by the presence of a band of the correct size (Figure 2). All specimens were DNA extracted with negative human DNA controls, which were subsequently submitted for PCR at the same time as the sample to exclude the possibility of contamination during DNA extraction. PCR was performed with positive controls and negative sample (water only) controls to exclude the possibility of contamination during setting up of PCR. Discussion We have described five patients with Whipple's disease whose presenting features would not, in the normal course of events, lead to a diagnosis of Whipple's. The first three patients presented with systemic disease characterized by lymphadenopathy, fever and splenomegaly as common features. Both pyrexia of unknown origin and granulomatous lymphadenopathy are well-documented features of Whipple's, but are not specific to this disorder.11'12 Relapsing thrombocytopenia was a prominent feature in patient 1, and has previously been described in only one patient with Whipple's. 13 In contrast, marked thrombocytosis with platelet counts ranging from 700 to 1100 x 109/l has been reported in some patients.14 The mechanism of the thrombocytopenia is unknown. If the Whipple's bacillus is present in platelets, this might result in up-regulation of platelet surface glycoproteins with consequent immune complex formation and clearance by macrophages. The cause of progressive lgG-2 subclass deficiency in patient 1 is unclear. It is debatable whether this is secondary to the disease process perse, or whether it preceded the development of Whipple's. If the latter, it could be argued that this patient exhibits many of the features of common variable immunodeficiency (CVI).15 Classical Whipple's disease has been documented in one patient with CVI, 16 while agammaglobulinaemia was noted in the late stages of the disease in another.17 These cases are exceptional, since serum immunoglobulin levels are reportedly elevated or normal in most patients.18 Although various abnormalities of cellular immunity have been described in Whipple's disease, including lymphopenia, increased expression of CD45 RO (marker of memory T cells), decreased expression of CD11b, impaired mitogen-induced lymphocyte transformation and reduced intracellular degradation of bacteria by macrophages, it is unclear whether these abnormalities are primary or secondary to the disease process.19'20 If a primary cellular immune defect is present, it is likely to be subtle, since patients with Whipple's disease are not prone to infection with opportunistic pathogens, in contrast with other cellular immune deficiency states. The articular manifestations of Whipple's disease have been well documented, commencing with Whipple's original description in 1907.21 Joint involvement is characterized in the main by a migratory symmetrical non-erosive polyarthritis affecting the knees, ankles and wrists.22 Where synovial biopsies have been performed, a spectrum of findings ranging from mild synovial cell hyperplasia to severe inflammation suggestive of septic arthritis has been reported.23'24 In contrast to the classical rheumatological features, patient 2 had a long history of ill health dating back to infancy, when a diagnosis of juvenile chronic arthritis (JCA) was made. Whether the onset of Whipple's disease in this patient coincided with her arthropathy in infancy is unclear. Presentation of Whipple's disease in infancy is exceptionally rare, but has been reported in a three-monthold baby at autopsy.25 Although other multisystem disorders may mimic JCA, there are no reports of Episodic fever, Hepatosplenomegaly, granulomatous, lymphadenopathy, ITP, AIHA, IgG 2 subclass, deficiency with impaired response to Pneumococcal immunization Arthropathy, episodic fever, hepatosplenomegaly, granulomatous lymphadenopathy Swinging fever, night sweats, splenomegaly, para-aortic lymphadenopathy Proximal muscle weakness, persistent sweating M 22 F 71 None None None Single episode of intestinal obstruction at the age of 6 yr None Gastro-intestinal symptoms No histological abnormality No histological abnormality PAS-positive macrophages in lymph node. Small bowel negative PAS-positve macrophages in muscle. Small bowel negative PAS-positive macrophages in spinal cord. Small bowel negative ND Pos ND ND ND ND ND Muscle Neg Pos" Negative in synovium lymph node and small bowel No histological abnormality No histological abnormality Pos" Blood PCR PAS-positive macrophages in lymph node. Small bowel negative PAS staining of tissues No histological abnormality Jejunal biopsy Pos ND Pos Pos Pos Intestine * Reverted to negative following treatment. ITP, immune thrombocytopenic purpura; AIHA, autoimmune haemolytic anaemia; ND, not done. 62 M 38 Spastic quadriparesis Clinical features Sex Age (years) Patient F Summary of key clinical features Table 1 ND ND ND Pos ND ND ND ND ND Pos Synovium Spleen ND ND Neg ND ND Lymph node 770 S.A. Misbah et al. Figure 2. Agarose gel electrophoresis of PCR-amplified DNA. Lanes 1 and 10, a 100 bp sized DNA ladder. Lane 2, positive control from a case of known gastrointestinal Whipple's showing a 284 bp PCR product. Lane 6, an identical PCR product from a representative patient in the study. Lanes 4, 8 and 9, negative controls comprising water (lane 4), human DNA extracted at a different time (lane 8) and human DNA extracted at the same time (lane 9) as the patient sample. Whipple's disease being mistaken for JCA. Despite histologically normal jejunal and synovial biopsies, patient 2 was PCR-positive in these tissues as well as in peripheral blood. The clinical presentation of patient 4 with isolated muscle weakness in the absence of systemic features suggestive of Whipple's is highly unusual, and has not been described before. Despite the absence of significant histological abnormality of the muscle fibres, focal endo- and perimysial infiltrates of PASpositive macrophages were observed, coupled with a positive PCR signal in muscle for T. whippelii. It is tempting to attribute the myalgic symptoms to the localization of inflammatory cells at the myotendinous junction where golgi tendon organs are present. Clinically overt myopathy has only been described previously in one patient with Whipple's disease. Swash et al. reported a 51-year-old man with antibiotic-responsive proximal myopathy associated with malabsorption and migratory arthralgia, in whom muscle biopsy showed mild type 2 fibre atrophy and PAS-positive macrophages.26 Tubular aggregates of uncertain nature in normal muscle without the presence of PAS-positive macrophages have also been described in a single patient with classical Whipple's. 27 The specificity of this finding for Whipple's disease is unclear, given the wide range of disorders in which tubular aggregates in muscle have been described.28 The appearances of interstitial macrophages with PAS-positive granules are similar to those illustrated by Banker and Engel, although clinical details were not given in this case.21 The neurological complications of Whipple's disease have been well described, with over a third of patients presenting with the characteristic triad of dementia, external ophthalmoplegia and facial myoclonus.29 Neurological involvement may either form part of systemic disease or present de novo without apparent gastrointestinal involvement. While such a presentation with the characteristic neurological triad would lead neurologists to consider the diagnosis of Whipple's, pure spinal involvement as in patient 5 would not. Despite the complete absence of gastrointestinal symptoms and a morphologically normal small bowel, PCR positivity for T. whippelii was demonstrated on jejunal biopsy. The use of PCR to demonstrate the presence of T. whippelii in peripheral blood mononuclear cells in addition to lymph nodes, duodenum and vitreous humour has raised the possibility of it being used as a non-invasive diagnostic test for Whipple's disease. PCR positivity in histologically-normal small bowel was noted in four of our patients and has also been recorded by others.10 This is an important observation which suggests the presence of sub-clinical bowel involvement in some patients. In patients who are PCR-positive on peripheral blood at initial assessment, it may prove to be a useful means for monitoring response to treatment. Enthusiasm for the use of PCR in the diagnosis and monitoring of Whipple's disease does not, however, mean that the search for PAS-positive macrophages can be discarded since Marth et al. have recently reported negative PCR results in peripheral blood from eight patients with Whipple's disease30 (4 with active disease, 4 with treated inactive disease). Whether PCR analysis should supplant the demonstration of PAS-positive macrophages as the gold standard for the diagnosis of Whipple's disease is unclear at present, and requires prospective study. We failed to demonstrate PAS positivity in one of our patients (patient 2) despite positive PCR signals from peripheral blood, duodenum and synovium. Similarly, Cohen et al. reported a case of purely neurological Whipple's diagnosed on the basis of PCR positivity on cerebrospinal fluid with no evidence of PAS-positive cells either in the CSF or small intestine.9 Given the atypical clinical presentations in these cases we did consider the possibility that our PCR results were artefactual. However, we believe that the unequivocal presence of PAS-positive macrophages in four patients, reversion of PCR positivity with treatment in 2/5 patients and the clinical response to prolonged antibiotic treatment suggests that this was unlikely to be the case. The five patients that we have described illustrate the wide heterogeneity of clinical presentation of Atypical Whipple's disease Whipple's disease and the considerable difficulties associated with making a diagnosis when the clinical presentation is atypical. Even when Whipple's disease is considered as part of the differential diagnosis, the absence of gastrointestinal involvement clinically, as in our patients, and negative PAS staining of small bowel may lead to the diagnosis being rejected. We suggest that the possibility of Whipple's be considered in any patient with an unexplained granulomatous disorder, even in the absence of gastrointestinal involvement. Our experience also suggests that the quest for PAS-positive macrophages in suspected cases should be accompanied by PCR analysis of relevant tissue. The pattern of clinical, pathological and laboratory findings in these cases suggests that we should view the relationship between man and the Whipple's bacillus as a spectrum. This ranges from the presence of the bacillus with no discernible morphological reaction (but detectable with PCR), through a localized inflammatory reaction at the site of initial infection (the classical intestinal form) to a more widespread dissemination of the bacillus (detectable by PCR) but with variable reactions in a range of tissues, which may include a necrotizing macrophage response or a granulomatous response. What it is that determines the pattern in an individual is conjectural, but immune competence and infective doses will be important variables. We do not know how widespread exposure to the bacillus which causes Whipple's disease is, or how many cases of infection occur without clinical disease. The availability of a sensitive tool in the form of PCR opens up the possibility of conducting the population studies necessary to answer these questions. We are extremely grateful to Dr M. Galvin for patient 1, Drs with negative jejunal histology. N Engl J Med 1979; 300:907-8. 4. Adams M, Rhyner PA, Day J, ef al. Whipple's disease confined to the central nervous system. Ann Neurol 1987; 21:104-8. 5. Wroe SJ, Pires M, Harding B, et al. Whipple's disease confined to the CNS presenting with multiple intracerebral mass lesions. J Neurol Neurosurg Psychiatry 1991; 54:989-92. 6. Adler CH, Caletta SL. Oculo-facial-skeletal myorhythmia in Whipple's disease: treatment with Ceftriaxone. Ann Intern Med 1990; 112:467-9. 7. Wilson KH, Blitchington R, Frothingham R, Wilson JAP. Phylogeny of the Whipple's disease associated bacterium. Lancet 1991; 338:474-5. 8. Relman DA, Schmidt TM, MacDermott RP, Falkow S. Identification of the uncultured bacillus of Whipple's disease. N Engl J Med 1992; 327:293-301. 9. Cohen L, Berthet K, Dauga C, ef al. Polymerase chain reaction of cerebrospinal fluid to diagnose Whipple's disease. Lancet 1996; 347:329. 10. Rickman LS, Freeman WR, Green WR, ef al. Uveitis caused by Tropheryma whippelii (Whipple's bacillus). N Engl J Med 1995; 332:362-6. 11. Fleming JL, Wiesner RH, Shorter RC. Whipple's disease: Clinical, biochemical and histopathologic features and assessment of treatment in 29 patients. Mayo Clin Proc 1988; 63:539-51. 12. James DG, Williams WJ. Report of the Commission on granulomatous diseases. Ann NY Acad Sci 1986; 465:304-12. 13. Finelli PF, McEntee WJ, Lessell S, ef al. Whipple's disease with predominantly neuroophthalmic manifestations. Ann Neuron 977; 1:247-52. 14. Nuzum CT, Sandier RS, Paulk HT. Thrombocytosis in Whipple's disease. Gastroenterology 1981; 80:1465-7. 15. Spickett GP, Misbah SA, Chapel HM. Primary antibody deficiency in adults. Lancet 1991; 337:281-4. 16. Cochran M, Cook MG, Gallagher JC, Peacock M. Hypogammaglobulinaemia with Whipple's disease. Postgrad Med} 1973; 49:355-8. Acknowledgements referring 771 S. Wyatt, D. Spence, C.J. Mitchell, C.E. Clarke and C.E. Millson for permission to report on their patients, Drs Andrew Jack and M. Dixon for histological reports, Dr S. Chitturi for serial endoscopies on patient 1, Dr D. Veale for synovial biopsy on patient 2, and to Faye Storey for typing the manuscript. References 1. Dobbins WO III. The diagnosis of Whipple's disease. N Engl JMed 1995; 332:390-2. 2. Mansbach CM, Shelburne JD, Stevens RD, Dobbins WO III. Lymph node bacilliform bodies resembling those of Whipple's disease in a patient without intestinal involvement. Ann Intern Med 1978; 89:64-6. 3. Feurle CE, Volk B, Waldherr R. Cerebral Whipple's disease 17. Anton AT. Agammaglobulinaemia complicating Whipple's disease. Ohio State Med} 1961; June:650-2. 18. Dobbins WO III. Is there an immune deficit in Whipple's disease? Dig Dis So 1981; 26:247-52. 19. Marth T, Roux M, von Herbay A, ef al. Persistent reduction of complement receptor 3 *-chain expressing mononuclear blood cells and transient inhibitory serum factors in Whipple's disease. Clin Immunol Immunopathoh 994; 72:217-26. 20. Bjerkness R, Odergaard S, Bjerkvig R, ef al. Whipple's disease—demonstration of a persisting monocyte and macrophage dysfunction. Scand} Gastroenterol 1988; 23:611-19. 21. Whipple GH. A hitherto undescribed disease characterised anatomically by deposits of fat and fatty acids in the intestinal mesenteric lymphatic tissues. John Hopkins Hosp Bull 1907; 18:382-91. 22. Weiner SR, Utsinger PD. Whipple's disease. Seminars in Arthritis and Rheumatism 1986; 15:157-70. 23. Caughey DE, Bywaters EG. The arthritis of Whipple's syndrome. Ann Rheum Dis 1963; 22:327-35. 772 S.A. Misbah et al. 24. Rubinow A, Canoso JJ, Goldenberg DL, Cohen AS. Arthritis in Whipple's disease. IsrJ Med Sci 1981; 17:445-50. 25. Aust CH, Smith EB. Whipple's disease in a three month old infant. AmJClin Pathol 1962; 37:66-74. 26. Swash M, Schwartz MS, Vandenburg MJ, Pollock DJ. Myopathy in Whipple's disease. Cut 1977; 18:800-4. 27. Stamboulis E, Manta P, Kararizou E, Crivas L. Whipple's disease with tubular aggregates in asymptomatic muscle. Clin Neuropathoh 993; 12:121-4. 28. Banker BQ, Engel AC. Basic reactions of muscle. In Engel AC, Franzini-Armstrong C, eds. Myology, 2nd edn. New York, McCraw Hill, 1994:832-88. 29. Dobbins WO III. Whipple's disease. Springfield, Charles C Thomas, 1987:113. 30. Marth T, Fredricks D, Strober W, Relman DA. Limited role for PCR-based diagnosis of Whipple's disease from peripheral blood mononuclear cells. Lancet 1996; 348:66-7.