Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
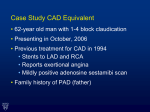
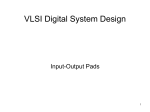
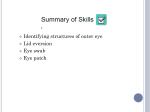
Page 1 of 24 Effects of Peripheral Arterial Disease on Outcomes in Advanced Chronic Systolic Heart Failure: A Propensity-Matched Study Mustafa I. Ahmed, MD,a Wilbert S. Aronow, MD,b Michael H. Criqui, MD, MPH,c Inmaculada Aban, PhD,a Thomas E. Love, PhD,d Eric J. Eichhorn, MD,e Ali Ahmed, MD, MPHa,f,* a University of Alabama at Birmingham, Birmingham, AL b New York Medical College, Valhalla, New York; c University of California, San Diego, La Jolla, CA d Case Western Reserve University, Cleveland, OH e Cardiopulmonary Research Science and Technology Institute, Dallas, las, TX f Veterans Affairs Medical Center, Birmingham, AL *** *Corresponding onding author: Ali Ahmed, MD, MPH, University of Alabama at Birmingham, Birmingham m 1530 3rd Ave A South, CH–19, Ste–219, Birmingham AL 35294–2041; Telephone: 1–205 1–205– 5 934–9632; Fax: 1–205–975–7099; Email: [email protected] Running head: Peripheral arterial disease outcomes in heart failure Word Count: 2453 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 2 of 24 Background– The effect of peripheral arterial disease (PAD) on outcomes in patients with chronic heart failure (HF) has not been examined in propensity-matched studies. Methods and Results–Of the 2689 patients with advanced chronic systolic HF in the BetaBlocker Evaluation of Survival Trial, 441 had a history of PAD. Propensity scores for a history of PAD, calculated for each patient using a multivariable logistic regression model, were used to assemble a matched cohort of 299 and 1015 patients respectively with and without PAD who were well-balanced on 65 measured baseline characteristics. Cox regression models were used to estimate hazard ratios (HR) and 95% confidence intervals (CI) for associations between PAD and outcomes during 4.1 years of follow-up. Patients p Patie ieent n s had a mean age of 63 (±11) years, 19% were women and 19% were African Americans. All-cause ican A meri me riica cans ns. Al All llmortality occurred in 43% and 33% of patients with and without a history of PAD, o respectively e (HR when PAD was compared with no-PAD, 1.40; 95% CI, 1.14–1.72; ely p=0.001). All-cause hospitalization occurred in 78% and 63% off patients with and witho without o PAD, respectively 1.16–1.58; p pectively (HR when PAD was compared with no-PAD, 1.36; 95% CI, 1.16–1.5 5 p<0.0001). PAD-associated HRs for cardiovascular mortality, HF mortality and HF hospitalization were respectively 1.31 (95% CI, 1.04–1.63; p=0.019), 1.40 (95% CI, 0.97– 2.02; p=0.076) and 1.05 (95% CI, 0.86–1.29; p=0.635). Conclusions– In a well-balanced propensity-matched population of chronic systolic HF patients, a history of PAD was independently associated with increased mortality and hospitalization. Key Words: heart failure, peripheral artery disease, mortality, hospitalization Word Count = 245 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 3 of 24 Peripheral arterial disease (PAD) is a manifestation of systemic atherosclerosis and predicts adverse cardiovascular outcomes.1-7 In a propensity-matched cohort of communitydwelling older adults, we have previously demonstrated that the presence of PAD had an independent association with increased all-cause and cardiovascular mortality.8 However, the extent to which PAD may be independently associated with outcomes in heart failure (HF) patients has not been previously examined in a propensity-matched study. In the current study, we used a public-use copy of the Beta–Blocker Evaluation of Survival Trial (BEST)9 dataset to determine the association between a baseline history of PAD and long-term outcomes in a propensity-matched population of advanced chronic systolic sys y tolic HF ppatients atient ntss iin nt which those with and without PAD were well-balanced in all measured ured ba bbaseline seli se line li ne characteristics. stics. Methodss Study Data ta and Patients h BEST was a multicenter randomized placebo-controlled clinical trial of he The bucindolol, a beta-blocker, in advanced systolic HF, methods and results of which have been previously published.9 Briefly, 2708 patients with advanced systolic HF were enrolled from 90 different sites across the United States and Canada between May 1995 and December 1998. At baseline, patients had a mean duration of 49 months of HF and had a mean left ventricular ejection fraction of 23%. All patients had New York Heart Association class IIIIV symptoms and over 90% of all patients were receiving angiotensin-converting enzyme (ACE) inhibitors, diuretics, and digitalis. Study Exposure and Outcomes The public-use copy of the BEST dataset included 2707 patients (one patient did not consent to be included in the public-use copy). After excluding 18 patients without data on smoking pack-years, a total of 2689 patients were included in the current analysis. Overall, Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 4 of 24 441 (16%) patients had a history of PAD at baseline. Data on a history of PAD were collected by study investigators and were not centrally adjudicated. Data on sociodemographic, clinical, sub-clinical and laboratory variables were collected at baseline. BEST participants were enrolled during a 3-year period and were followed up for a minimum of 18 months and a maximum of 4.5 years.9 Primary outcomes for the current analysis were allcause mortality and all-cause hospitalization during 4.1 years of follow-up (mean, 2 years; range, 10 days to 4.14 years). Secondary outcomes were mortality due to cardiovascular causes, heart failure and sudden cardiac death and hospitalizations due to HF. Assembly of a Balanced Cohort of Patients with and without PAD AD tics bbetween ettwe ween en ppatients atie at ient ie ntss with nt As there were significant imbalances in baseline characteristics ut PAD before matching (Table 1), we used propensity score matching to asse e and without assemble of patients whereby those with and without PAD would be well-balanced on alll a cohort of measured baseline covariates.10-12 Propensity score for PAD for a patient would be that patient’s probability p of having PAD given his or her measured baseline characteristics. Propensity scores for PAD were estimated for each of the 2689 patients using a nonparsimonious multivariable logistic regression model. In the model, PAD was the dependent variable and 65 baseline characteristics displayed in Figure 1 were used as covariates in the model. A number of clinically relevant interactions such as age by smoking, coronary artery disease (CAD) by smoking etc were also were included in initial models but were excluded from the final model due to lack of statistical significance. We used a greedy matching protocol, described in detail elsewhere, to match one patient with PAD with up to 4 patients without PAD. Using this approach, we were able to match 299 patients with PAD with 1015 patients without PAD.13-17 Because propensity score models are sample-specific adjusters and are not intended to be used for out-of-sample prediction or estimation of coefficients, measures of fitness and Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 5 of 24 discrimination are not important for the assessment of the model's effectiveness. As such, measures of fitness and discrimination are irrelevant for the assessment of the model's effectiveness.13-17 We assessed propensity score models by estimating pre- and post-match absolute standardized differences for measured baseline covariates between patients with and without PAD. Absolute standardized differences directly quantify bias in the means (or proportions) of covariates across the groups. They are expressed as a percentage of the pooled standard deviation and are presented in Love plots.13-17 An absolute standardized difference of 0% indicates no residual bias and differences <10% are considered inconsequential. Statistical Analysis a aplan-Meier Kaplan-Meier and Cox regression analyses were used to determine associations durin 4.1 years ars of follow-up. follow- . Log-minus-log Lo minus-lo scale survival surviva between PAD and outcomes during plots weree used to check proportional hazards assumptions. Formal sensitivity analyses were i conductedd to quantify the degree off a hidden bias that would need to be present to invali invalidate our conclusions based on significant association between PAD and primary outcomes among matched patients.18 Subgroup analyses were conducted to determine the homogeneity of association between a history of PAD and all-cause mortality. All statistical tests were twotailed with a p-value <0.05 considered significant. All data analyses were performed using SPSS for Windows version 15 (SPSS Inc., Chicago, IL).19 Results Baseline Characteristics Matched patients had a mean age of 63 (±11) years, 19% were women and 19% were African Americans. Significant imbalances in several baseline characteristics before matching and the balances achieved after matching are displayed in Table 1 and Figure 1. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 6 of 24 After matching, standardized differences for all measured covariates were <10% (most were <5%), suggesting substantial covariate balance across the groups (Figure 1). PAD and Mortality All-cause mortality occurred in 43% and 33% of patients with and without PAD respectively (hazard ratio, 1.40; 95% confidence interval, 1.14–1.72; p=0.001; Figure 2a and Table 2). In the absence of hidden bias, a sign-score test for matched data with censoring provides relatively strong evidence (p=0.035) that patients without PAD clearly outlived those with PAD. A hidden covariate that is a near-perfect predictor of mortality may potentially explain away the association between PAD and all-causee mortality would y if thatt wo w increase the odds of PAD by only 1. 3% No heterogeneity of association PAD ation n bbetween ettwe ween en P AD aand all-cause mortality Associations m was detected in any of the subgroups of patients (Figure 3). Associat t of PAD with w mortality due to cardiovascular causes, HF, and sudden cardiac death are displayed in Table 2. PAD and Hospitalization All-cause hospitalization occurred in 78% and 63% patients with and without PAD respectively (HR, 1.36; 95% CI, 1.16–1.58; p<0.0001; Figure 2b and Table 2). In the absence of hidden bias, a sign-score test for matched data with censoring provides strong evidence (p=0.001) that patients without PAD clearly had fewer hospitalizations due to all causes than those with PAD. A hidden covariate that is a near-perfect predictor of hospitalization, could potentially explain away our observed association between PAD and all-cause hospitalization, should it increase the odds of PAD by 9.4%. Other pre- and postmatch associations of PAD with hospitalizations are displayed in Table 2. Discussion Findings from the current study demonstrate that the prevalence and the burden of CAD was high among systolic HF patients with a history of PAD, and a history of PAD was Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 7 of 24 associated with increased risk of mortality and hospitalization in these patients. Significant strong bivariate associations of PAD with major natural history endpoints suggest that the presence of PAD may be used to identify advanced systolic HF patients who are at an increased risk for poor outcomes. The significant associations of PAD with all-cause mortality and all-cause hospitalization after propensity score matching suggest that the effect of PAD was independent of the 65 measured baseline characteristics that included major cardiovascular risk factors. These findings are important as PAD is common in patients with advanced systolic HF.20 Strong bivariate associations between PAD and outcomes aree likelyy due to ell llit itus it us, th thee pr pprevalence eval ev al confounding by covariates such as age, smoking, CAD, and diabetess me mellitus, of which was w higher in those with PAD than in those without PAD. However, associatio associations o P between PAD and all-cause mortality and all-cause hospitalization persisted despite riskk adjustments n using multiple approaches including propensity matching. This suggests an nts intrinsic association a between PAD and outcomes in HF that was independent of the measured meaa covariates in our study. However, we are not aware of any mechanistic pathway of a direct and intrinsic effect of PAD on death or hospitalization. One possible explanation is that atherosclerotic diseases in PAD patients are of a greater severity and more advanced or widespread.1, 21, 22 This is evident from the higher prevalence and burden of CAD and other morbidities in pre-match patients with PAD. While these and other measured confounders were well-balanced after matching, it is possible that atherosclerosis progressed at a faster rate during follow-up in patients with PAD than in those without PAD. Findings from our subgroup analysis also suggest a significant PAD-associated increase in mortality among those with CAD. It is also possible that HF patients with clinical PAD may restrict their physical activity to avoid claudication pain, potentially leading to deconditioning and deterioration of cardiovascular fitness and poor outcomes.23 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 8 of 24 Findings from population-based studies suggest that age, smoking, systolic blood pressure, and serum glucose are significantly associated with large vessel PAD.24 Before matching patients with PAD in our study were older, with a significantly higher prevalence of current smokers and higher pack-years of smoking, higher systolic blood pressure and higher serum glucose, all indicating the presence of large vessel PAD. Large vessel PAD has been shown to be independently associated with increased mortality.4 Smoking is one of the strongest predictors for progression of large vessel PAD.6, 25 Although our matched patients were balanced on pack-years of smoking and prevalence of current smokers, it is possible d in the ppresence resencee of that the deleterious effects of continued smoking was more profound PAD.26, 27 An n examination of the associations between PAD and cause-specific mortalities u urther patiee provide further insight into how PAD may affect mortality in advanced systolic HF patients. Sudden cardiac a ardiac death was a major mode of death in our study, accounting for over half of o all deaths. However, o owever, PAD apparently was not associated with fatal cardiac arrhythmias underlying sudden deaths. This lack of a statistically significant association between PAD and sudden death suggests that the effect of PAD in HF may be predominantly non-sudden in nature. PAD, however, had significant associations with cardiovascular death, and its association with HF death was of borderline significance. PAD has also been shown to be associated with increased risk of fatal acute myocardial infarction (AMI).5 However, only <5% of all deaths in our study were due to AMI, which may explain the non-significant association between PAD and AMI death. PAD-associated increase in the risk of other cardiovascular mortality highlights its impact on vascular deaths such as those due to stroke. Unfortunately, we had limited data on cause-specific hospitalizations with which to gain insights into the PAD-associated increase in all-cause hospitalization in advanced systolic HF patients. Extrapolating from cause-specific mortality data, it may be suggested that PAD- Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 9 of 24 associated increase in hospitalization was primarily due to cardiovascular causes. However, recent reports have suggested an association between PAD and non-cardiovascular morbidities.28, 29 To the best of our knowledge this is the first report of an association of PAD with mortality and hospitalization in a propensity matched population of advanced chronic systolic HF patients. Our findings of increased mortality and morbidity in chronic HF patients with PAD have important clinical and public health implications. PAD may be a manifestation of more severe and/or advanced systemic atherosclerosis, and thus its presence can be used to identify HF patients with poorer prognosis. This may be useful as ann inexpensive inexpe p nsive clinical clin in nic ica tool fte t n be be in developing nations to risk stratify HF patients. Importantly PAD mayy of often m matic and hence under-diagnosed. It is relatively easy, however, to accurately asymptomatic t presence and severity PAD by measures such as the ankle-brachial pressuree diagnose the h index. Ourr findings of independent associations of PAD with poor outcomes highlight th the c of prevention and timely detection of PAD, and aggressive treatment of ce importance atherosclerotic risk factors in HF patients. Management of PAD in HF is similar to that in the general population with a few exceptions. Current recommendations for management of PAD patients are mainly based on reduction of systemic cardiovascular risk, which include smoking cessation, exercise, treatment of hypertension and diabetes, and the use of antiplatelet agents and statins.30 Walking and physical training have been shown to improve claudication distance in patients with PAD.31, 32 Cilostazol, a phosphodiesterase-3 inhibitor approved for use in symptomatic PAD, is contraindicated in HF (a black-box warning). Pentoxifylline, a phosphodiesterase-4 inhibitor, also approved for use in symptomatic PAD, may be safe in HF.33 However, its efficacy in improving walking distance is very limited.32 Statins and ACE inhibitors have shown some efficacy for walking distance, however there is no labeled indication for these Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 10 of 24 drugs.34-37 Despite concerns that beta-blockers may cause or worsen claudication in patients with PAD these drugs are not contraindicated in these patients.30 We observed that the effect of PAD on mortality appeared to be heterogeneous between patients receiving and not receiving bucindolol, a beta-blocker. However, the lack of a significant interaction (p=0.140: Figure 3) precludes any inference of heterogeneity. It is possible that the non-significant interaction may be due to inadequate power. Considering the potential clinical importance of these findings, future studies with adequate sample sizes are needed to examine the heterogeneity of the effect of PAD on outcomes in HF patients receiving and not receiving beta-blockers. ed. Findings Fin i di ding ngss off this thi thi hiss sstudy Several limitations of the current study must be acknowledged. a systolic HF patients enrolled in n a clinical trial may nott be generalizab b to based on advanced generalizable w mild-moderate systolic HF or diastolic HF. Data on ankle-brachial pressuree patients with r not available and diagnosis of PAD was based on patient past medical histor re r as index were history b study investigators. This may have misclassified some PAD patients and assessed by underestimated the true prevalence of PAD. Data were not available on the extent and severity of PAD. It is possible that patients without PAD at baseline may have developed PAD during follow-up, thus resulting in regression dilution bias, which is another potential source of underestimation of the true association between PAD and outcomes38. Finally, the findings of our sensitivity analyses suggest that our conclusions were rather sensitive to an unmeasured confounder. However, sensitivity analysis cannot determine if an unmeasured confounder exists or not. To be a confounder, an unmeasured covariate, in addition to being associated with PAD, would also need to have a near-perfect association with outcomes, without any strong association with any of the 65 measured baseline covariates used in our study, a possibility which seems highly unlikely. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 11 of 24 In conclusion, PAD in advanced chronic systolic HF patients was associated with increased risk of death and hospitalization, which was independent of 65 baseline characteristics including major cardiovascular risk factors. PAD-associated poor outcomes in HF patients are likely non-sudden in nature and likely to be predominantly atherosclerotic in origin. PAD may be useful as an inexpensive screening tool to risk stratify HF patients. Acknowledgement: “The Beta–Blocker Evaluation of Survival Trial (BEST) is conducted and supported by the NHLBI in collaboration with the BEST Study Investigators. This Manuscript was prepared using a limited access dataset obtained from and om the NHLBI an nd ddoes not necessarily reflect the opinions or views of the BEST or the NHLBI.” LBI. I” Funding/Support: Dr. Ahmed is supported by the National Institutes of Health throughh S Support: grants (R01-HL085561 0 01-HL085561 and R01-HL097047) from the National Heart, Lung, and Blood Institute and a a generous gift from Ms. Jean B. Morris of Birmingham, Alabama Conflict of Interest Disclosures: None Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 12 of 24 References: 1. Criqui MH. Systemic atherosclerosis risk and the mandate for intervention in atherosclerotic peripheral arterial disease. Am J Cardiol. 2001;88:43J-47J. 2. Criqui MH, Denenberg JO. The generalized nature of atherosclerosis: how peripheral arterial disease may predict adverse events from coronary artery disease. Vasc Med. 1998;3:241-245. 3. Langlois M, Duprez D, Delanghe J, De Buyzere M, Clement DL. Serum vitamin C concentration is low in peripheral arterial disease and is associated with inflammation and severity of atherosclerosis. Circulation. 2001;103:1863-1868. 1868 18 68.. 68 4. Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, MR McCann McCa Mc Cann Ca nn TJ, TJ Browner Bro r D. Mortality over a period of 10 years in patients with peripheral arterial disease disease. N Engl n J Med. 1992;326:381-386. ngl 5. Golomb BA, Dang TT, Criqui MH. Peripheral arterial disease: morbidity and o olomb mortality o ortality implications. Circulation. 2006;114:688-699. 6. Criqui MH, Ninomiya JK, Wingard DL, Ji M, Fronek A. Progression of peripheral arterial disease predicts cardiovascular disease morbidity and mortality. J Am Coll Cardiol. 2008;52:1736-1742. 7. Criqui MH, Coughlin SS, Fronek A. Noninvasively diagnosed peripheral arterial disease as a predictor of mortality: results from a prospective study. Circulation. 1985;72:768-773. 8. Aronow WS, Ahmed MI, Ekundayo OJ, Allman RM, Ahmed A. A propensitymatched study of the association of peripheral arterial disease with cardiovascular outcomes in community-dwelling older adults. Am J Cardiol. 2009;103:130-135. 9. The BEST Investigators. A trial of the beta-blocker bucindolol in patients with advanced chronic heart failure. N Engl J Med. 2001;344:1659-1667. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 13 of 24 10. Rosenbaum PR, Rubin DB. The central role of propensity score in observational studies for causal effects. Biometrika. 1983;70:41-55. 11. Rubin DB. Using propensity score to help design observational studies: Application to the tobacco litigation. Health Services and Outcomes Research Methodology. 2001;2:169-188. 12. Rubin DB. Estimating causal effects from large data sets using propensity scores. Ann Intern Med. 1997;127:757-763. 13. Ahmed A, Aban IB, Vaccarino V, Lloyd-Jones DM, Goff DC, Jr., Zhao J, Love TE, Ritchie C, Ovalle F, Gambassi G, Dell'Italia LJ. A propensity-matched y matched studyy of tthe yeffect of diabetes on the natural history of heart failure: variations ations ns bby y se sexx an andd ag aage. age g Heart. e eart. 2007;93:1584-1590. 14. Ahmed M, h hmed A, Allman RM, Fonarow GC, Love TE, Zannad F, Dell'italia LJ, White M Gheorghiade M. Incident heart failure hospitalization and subsequent mortality in h heorghiade i chronic 2008;14:211-218. r ronic heart failure: a propensity-matched study. J Card Fail. 2008;14:211-218 8 15. Ahmed A, Husain A, Love TE, Gambassi G, Dell'Italia LJ, Francis GS, Gheorghiade M, Allman RM, Meleth S, Bourge RC. Heart failure, chronic diuretic use, and increase in mortality and hospitalization: an observational study using propensity score methods. Eur Heart J. 2006;27:1431-1439. 16. Ahmed A, Pitt B, Rahimtoola SH, Waagstein F, White M, Love TE, Braunwald E. Effects of digoxin at low serum concentrations on mortality and hospitalization in heart failure: a propensity-matched study of the DIG trial. Int J Cardiol. 2008;123:138-146. 17. Ahmed A, Rich MW, Sanders PW, Perry GJ, Bakris GL, Zile MR, Love TE, Aban IB, Shlipak MG. Chronic kidney disease associated mortality in diastolic versus systolic heart failure: a propensity matched study. Am J Cardiol. 2007;99:393-398. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 14 of 24 18. Rosenbaum PR. Sensitivity to Hidden Bias. In: Rosenbaum PR, ed. Observational Studies. 2 ed. New York: Springer-Verlag; 2002:110 - 124. 19. SPSS for Windows, Rel. 15 [computer program]. Version. Chicago, IL: SPSS Inc., Chicago, IL; 2008. 20. Ness J, Aronow WS, Newkirk E, McDanel D. Prevalence of symptomatic peripheral arterial disease, modifiable risk factors, and appropriate use of drugs in the treatment of peripheral arterial disease in older persons seen in a university general medicine clinic. J Gerontol A Biol Sci Med Sci. 2005;60:255-257. 21. Criqui MH, Langer RD, Fronek A, Feigelson HS. Coronary disease and stroke kee iin n patients with large-vessel peripheral arterial disease. Drugs. 1991 1991;42 Suppl 5:16-21. 1;4 42 Su S pp pl 5: 5:16 1616 22. Sukhija R, Yalamanchili K, Aronow WS. Prevalence of left main coronary arteryy u ukhija disease, of three- or four-vessel coronary artery disease, and of obstructive coron coronary s sease, n artery t tery disease in patients with and without peripheral arterial disease undergoingg coronary angiography for suspected coronary artery disease. Am J Cardiol. r ronary 2003;92:304-305. 23. Garg PK, Tian L, Criqui MH, Liu K, Ferrucci L, Guralnik JM, Tan J, McDermott MM. Physical activity during daily life and mortality in patients with peripheral arterial disease. Circulation. 2006;114:242-248. 24. Criqui MH, Browner D, Fronek A, Klauber MR, Coughlin SS, Barrett-Connor E, Gabriel S. Peripheral arterial disease in large vessels is epidemiologically distinct from small vessel disease. An analysis of risk factors. Am J Epidemiol. 1989;129:1110-1119. 25. Aboyans V, Criqui MH, Denenberg JO, Knoke JD, Ridker PM, Fronek A. Risk factors for progression of peripheral arterial disease in large and small vessels. Circulation. 2006;113:2623-2629. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 15 of 24 26. Frohlich M, Sund M, Lowel H, Imhof A, Hoffmeister A, Koenig W. Independent association of various smoking characteristics with markers of systemic inflammation in men. Results from a representative sample of the general population (MONICA Augsburg Survey 1994/95). Eur Heart J. 2003;24:1365-1372. 27. Fushimi H, Kubo M, Inoue T, Yamada Y, Matsuyama Y, Kameyama M. Peripheral vascular reactions to smoking--profound vasoconstriction by atherosclerosis. Diabetes Res Clin Pract. 1998;42:29-34. 28. von Muhlen D, Allison M, Jassal SK, Barrett-Connor E. Peripheral arterial disease and osteoporosis in older adults: the Rancho Bernardo Study. y Osteoporos y. Osteopporos Int. Intt. 20 22009. 29. Collins TC, Ewing SK, Diem SJ, Taylor BC, Orwoll ES, Cummings Strotmeyer ummi miing ngss SR SR, St S tro otm tme ES, S Ensrud KE. Peripheral arterial disease is associated with higher rates of hip bbone S, loss s and increased fracture risk in older men. Circulation. 2009;119:2305-2312. ss 30. Hirsch Hiratzka i irsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratz z LF, KA, Sacks D, Stanley JC, Ta Taylor F Murphy WR, Olin JW, Puschett JB, Rosenfield F, f a LM, Jr., White CJ, White J, White RA, Antman EM, Smith SC, Jr., Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 16 of 24 Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113:e463-654. 31. Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA. 1995;274:975-980. 32. Girolami B, Bernardi E, Prins MH, Ten Cate JW, Hettiarachchi R, Prandoni P, Girolami A, Buller HR. Treatment of intermittent claudication with physical training, smoking cessation, pentoxifylline, or nafronyl: a meta-analysis. Arch Intern Med. 1999;159:337-345. 33. Sliwa K, Woodiwiss A, Candy G, Badenhorst D, Libhaber C, Norton G, Skudicky Skuudi dicck D, Sareli P. Effects of pentoxifylline on cytokine profiles and left eft ventricular vent ve nttricu riicula lar performance in patients with decompensated congestive heart failure secondary to r rformance t idiopathic i iopathic dilated cardiomyopathy. Am J Cardiol. 2002;90:1118-1122. 34. Hirsch inhibition i irsch AT, Duprez D. The potential role off angiotensin-converting enzyme inhib b in peripheral arterial disease. Vasc Med. 2003;8:273-278. 35. McDermott MM, Guralnik JM, Greenland P, Pearce WH, Criqui MH, Liu K, Taylor L, Chan C, Sharma L, Schneider JR, Ridker PM, Green D, Quann M. Statin use and leg functioning in patients with and without lower-extremity peripheral arterial disease. Circulation. 2003;107:757-761. 36. Mohler ER, 3rd, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral arterial disease. Circulation. 2003;108:1481-1486. 37. Ahimastos AA, Lawler A, Reid CM, Blombery PA, Kingwell BA. Brief communication: ramipril markedly improves walking ability in patients with peripheral arterial disease: a randomized trial. Ann Intern Med. 2006;144:660-664. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 17 of 24 38. Clarke R, Shipley M, Lewington S, Youngman L, Collins R, Marmot M, Peto R. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol. 1999;150:341-353. Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 18 of 24 Figure Legends Figure 1. Love plot displaying absolute standardized differences in baseline covariates between patients with and without peripheral arterial disease, before and after propensity score matching (ACE=angiotensin-converting enzyme; ARB=angiotensin receptor blocker) Figure 2. Kaplan-Meier plots for (a) all-cause mortality and (b) all-cause hospitalization by a history of peripheral arterial disease (PAD) Figure 3. Association between peripheral arterial disease (PAD) and all-cause mortality nd al lll ca caus usee mo mort rttal alit ity in it subgroupss of propensity score-matched patients in the BEST trial (CI=confidence interv interval) v Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 19 of 24 Table 1 Baseline patient characteristics by history of peripheral artery disease (PAD) before and after propensity matching Before propensity matching No history of PAD (n=2248) 60 (r13) History of PAD (n=441) 64 (r10) Female 497 (22) African American After propensity matching <0.0001 No history of PAD (n=1015) 63 (r11) History of PAD (n=299) 64 (r10) 86 (20) 0.224 196 (19) 58 (19) 0.973 530 (24) 89 (20) 0.121 204 (20) 54 (18) 0.435 Duration of heart failure, months 49 (r48) 53 (r49) 0.087 51 (r51) 51 (r49) 0.655 Left ventricular ejection fraction, % 23 (±7) 24 (±7) 0.118 23 (±7) 24 (±7) 0.629 Right ventricular ejection fraction, % 35 (r12) 35 (r11) 0.215 35 (±12.0) 35 (±11) 0.920 New York Heart Association class III 2077 (92) 386 (87) 0.001 914 (90) 272 (91) 0.637 Coronary artery disease 1231 (55) 353 (80) <0.0001 739 (73) 222 (74) 4) 0.622 Angina pectoris 1107 (49) 284 (64) <0.0001 616 61 6 (6 (61) 1) 181 18 1 (6 (61)) (61) 0.962 Coronary artery stenosis >70% 946 (42) 289 (66) <0.0001 584 (5 (58) 8 8) 180 18 0 (6 ((60) 0) 0.412 Stress perfusion n test positive 426 (19) 114 (26) 0.001 249 (25) 73 (24) 0.967 Left bundle branch a anch block 589 (26) 85 (19) 0.002 222 (22) 64 (21) 0.863 Coronary artery y bypass graft surgery 585 (26) 192 (44) <0.0001 369 (36) 124 (42) 0.108 Percutaneous coronary c intervention 329 (15) 89 (20) 0.003 186 (18) 50 (17) 0.526 n (%) or mean (rSD) Age, years P value P value 0.122 Coronary artery disease-related history Current smoker e er 377 (17) 94 (21) 0.022 203 (20) 56 (19) 0.627 Smoking , pack-years k k-years 20 (r17) 29 (r18) <0.0001 25 (r17) 26 (r18) 0.921 1282 (57) 301 (68) <0.0001 635 (63) 191 (64) 0.678 Other medical history t tory Hypertension Diabetes mellitus 723 (32) 237 (54) <0.0001 442 (44) 142 (48) 0.228 Hyperlipidemia 909 (40) 255 (58) <0.0001 524 (52) 167 (56) 0.198 Atrial fibrillation 542 (24) 107 (24) 0.945 250 (25) 67 (22) 0.430 Medications Angiotensin-converting enzyme inhibitors 2175 (97) 416 (94) 0.013 983 (97) 290 (97) 0.901 Digitalis 2073 (92) 403 (91) 0.554 914 (90) 275 (92) 0.319 Diuretics 2084 (93) 422 (96) 0.023 957 (94) 284(95) 0.644 Vasodilators 925 (41) 249 (57) <0.0001 519 (51) 153 (51) 0.991 Anti-arrhythmic drugs Anti-coagulants 66 (3) 8 (2) 0.188 23 (2) 6 (2) 0.789 1274 (57) 283 (64) 0.004 631 (62) 184 (62) 0.844 37 (±8.5) 35 (±7.5) <0.0001 36 (±7.6) 35 (±8.0) 0.700 Clinical findings Body mass index, kg/m2 Heart rate, beats per minute 82 (±13) 81 (±13) 0.285 81 (±13) 81 (±13) 0.774 Systolic blood pressure, mm Hg 117 (±18) 120 (±18) <0.0001 119 (±18) 119 (±18) 0.988 Diastolic blood pressure, mm Hg 71 (±11) 70 (±11) 0.002 70 (±11) 70 (±11) 0.415 Jugular venous distension 1035 (46) 193 (44) 0.380 452 (45) 129 (43) 0.671 S3 gallop 986 (44) 181 (41) 0.275 428 (42) 121 (41) 0.601 Pulmonary râles 282 (13) 76 (17) 0.008 152 (15) 43 (14) 0.800 Lower extremity edema 590 (26) 136 (31) 0.047 287 (28) 83 (28) 0.861 Pulmonary edema by chest x-ray 238 (11) 68 (15) 0.003 125 (12) 39 (13) 0.738 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 20 of 24 Table 1 Baseline patient characteristics by history of peripheral artery disease (PAD) before and after propensity matching Before propensity matching No history of PAD (n=2248) History of PAD (n=441) Hemoglobin, g/dl 14.0 (±1.6) White blood cells, 103/μL 7.4 (±2.2) Creatinine, mg/dl Glucose, mg/dl n (%) or mean (rSD) After propensity matching P value No history of PAD (n=1015) History of PAD (n=299) 13.8 (±1.7) 0.050 13.9 (r1.7) 13.8 (r1.7) 0.885 7.8 (±2.1) 0.003 7.6 (r2.3) 7.7 (r2.1) 0.661 1.2 (±0.4) 1.4 (±0.5) <0.0001 1.3 (r0.4) 1.3 (r0.4) 0.239 129 (±69) 162 (±94) <0.0001 144 (r79) 151 (r86) 0.186 P value Laboratory findings Sodium, mEq/L 139 (r3) 138 (r4) 0.001 139 (r3) 138 (r4) 0.626 Potassium, mEq/L 4.3 (±0.5) 4.4 (±0.5) 0.052 4.3 (r0.5) 4.4 (r0.5) 0.338 Magnesium, mg/dl 1.7 (±0.3) 1.8 (±0.3) 0.021 1.8 (r0.3) 1.8 (r0.3) 0.135 Norepinephrine, pg/ml 510 (r308) 537 (r296) 0.101 525 (±327) 520 (±270) 0.837 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 21 of 24 Table 2. Peripheral artery disease (PAD) and outcomes in the matched cohort % events (total number of event / total duration of follow-up in years) Outcomes Hazard ratio (95% confidence interval) P value No history of PAD (n=1015) History of PAD (n=299) All-cause 33% (331/2020) 44% (130/568) 1.40 (1.14–1.72) 0.001 Cardiovascular 28% (287 / 2020) 35% (105 / 568) 1.31 (1.04–1.63) 0.019 Heart failure 10% (100 / 2020) 13% (39 / 568) 1.40 (0.97–2.02) 0.076 Sudden cardiac death 15% (155 / 2020) 16% (48 / 568) 1.10 (0.80–1.53) 0.552 Myocardial infarction 1% (11 / 2020) 2% (5 / 568) 1.62 1.62 (0.56–4.65) (0. 0 56 56–4 –4.665) 0.374 Other cardiovascular 2% (21 ( / 2020)) 4% (13 ( / 568)) 2.20 2 200 (1.10–4.39) (1 10 10–4 –4 39) 0.026 Non-cardiovascular u ular 3% (34 / 2020) 6% (17 / 568) 1.78 (0.99–3.20) 0.076 Unknown 1% (10 / 2020) 3% (8 / 568) 2.89 (1.14–7.32) 0.025 63% (640 / 1186) 39% (400 / 1563) 75% (223 / 294) 41% (121 / 444) 1.36 (1.16–1.58) <0.0001 1.05 (0.86–1.29) ( ) 0.635 Mortality Hospitalization All-cause Heart failure Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 22 of 24 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 23 of 24 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Page 24 of 24 Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016 Effects of Peripheral Arterial Disease on Outcomes in Advanced Chronic Systolic Heart Failure: A Propensity-Matched Study Mustafa I. Ahmed, Wilbert S. Aronow, Michael H. Criqui, Inmaculada Aban, Thomas E. Love, Eric J. Eichhorn and Ali Ahmed Circ Heart Fail. published online October 27, 2009; Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2009 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/early/2009/10/28/CIRCHEARTFAILURE.109.866558 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/ Downloaded from http://circheartfailure.ahajournals.org/ by guest on March 4, 2016