Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
3 - Physics of the Respiration Animals require energy to function. This energy is provided by food which is oxidized by the
body. The simplest way to obtain the required oxygen is by diffusion through the skin. This
method however, cannot supply the needs of large animals. It has been determined that in a
person only 2% of oxygen consumed at rest is obtained by diffusion through the skin. The rest
of the oxygen is obtained through the lungs.
The goals of respiration are to provide the oxygen to the tissues and to remove carbon
dioxide.
To achieve this goals respiration can be divided into four main functional events:
1) Pulmonary ventilation, which means the inflow and outflow of air between the
atmosphere and lung alveoli;
2) Diffusion of oxygen and carbon dioxide between the alveoli and the blood;
3) Transport of oxygen and carbon dioxide in the blood and body fluids to and from the
cells;
4) Regulation of ventilation.
3.1. The respiratory system
The respiratory system consists of the two lungs, conducting airways, pulmonary circulation,
diaphragm and chest wall (pleura), and the associated blood vessels, muscles, and nerves.
The respiratory system starts at the
nose and mouth and continues through
the airways and the lungs. Each lung is
divided into sections (lobes): three in
the right lung and two in the left lung.
The left lung is a little smaller than the
right lung because it shares space in the
left side of the chest with the heart. The
pleura is a slippery membrane that
covers the lungs as well as the inside of
the chest wall. It allows the lungs to
move smoothly during breathing and as
the person moves. Normally, the two
layers of the pleura have only a small
amount of lubricating fluid between
them. The two layers glide smoothly
over each other as the lungs change
size and shape.
3-1
The lungs can be thought of as an
elastic bag suspended in the chest
cavity. When the diaphragm descends
the volume of the lungs increases
causing a reduction of gas pressure
inside the lungs.
To equalize pressure air enters the
lung through the superior airways: the
nose and mouth and passes down the
pharynx, larynx and trachea. When the
diaphragm relaxes and moves back up,
the elasticity of the lungs and chest
wall pushes air out of the lungs.
The largest airway is the trachea, which branches into two smaller airways: the left and right
bronchi, which lead to the two lungs. The bronchi themselves branch many times into smaller
airways, ending in the narrowest airways (bronchioles), which are as small as one half of a
millimeter across. Large airways are held open by semi-flexible, fibrous connective tissue
called cartilage. Small airways are supported by the lung tissue, which surrounds and is
attached to them. Circular airway smooth muscle can dilate or constrict, thus changing airway
size.
Each bronchiole terminates at tiny a cavity called alveolus. Together, the millions of alveoli
of the lungs (an adult has about 300 million alveoli with diameters between 0.1 and 0.3 mm)
form a surface of more than 100 m2, which is about 50 times the total surface area of the skin.
It is here that gas is exchanged by diffusion between the blood and the air in the lungs.
Within the alveolar walls is a dense network of tiny blood vessels called capillaries. The
barrier between air and capillaries is extremely thin of about 4x10-5 cm. Therefore the gas
exchange of O2 into the blood and CO2 out of the blood is very fast.
The pressure of the fluid in the narrow space between the lung pleura and the chest wall
pleura exerts a slightly negative pressure (suction). The pressure varies between the
beginning of inspiration and a normal inspiration, which causes an expansion of the chest
cage pulling outward. The variation in pleural pressure is also accompanied by variations in
the alveolar pressures and lung volume changes. In order to understand how respiratory
system works from a mechanical point of view, it is helpful to conceptualize it as two
structures, the lungs and the chest wall, each with elastic properties: the lungs have a
tendency to recoil inwards and the chest wall a tendency to recoil outwards. If the lungs are
removed from the thoracic cavity and no longer have the influences of the chest wall and
pleural space acting on them, they would be almost completely air less, at a volume [minimal
volume] substantially lower than they have in situ, within the thoracic cavity.
Under static conditions, the trans-pulmonary pressure is equal to the elastic recoil pressure
of the compartment and refers to the pressure inside relative to outside compartment. This is a
3-2
!"#$%&#$'(#)*+,-*,+&.#$%+&&#/(012+*0&3*#4(5&6#
#
"#$"%&'(&")%"*$'(&+),$'"-%."&(+/0&,)%&1"+1+)(2".%&3+"4&%2","2(5-,$05,6"/%0$)"%4"70(.8"0)"0+"-(6/4*6")%"5%$5(/)*,609("0)",+").%"
+)&*5)*&(+8")-("6*$:+",$'")-("5-(+)".,668"(,5-".0)-"(6,+)05"/&%/(&)0(+;"<)"=>?8")-("6*$:+"-,7(",")($'($51")%"&(5%06"0$.,&'+@"
)-("5-(+)".,66",")($'($51")%"&(5%06"%*).,&'+;""#4")-("6*$:+",&("&(2%7('"4&%2")-(")-%&,505"5,70)1",$'"$%"6%$:(&"-,7(")-("
0$46*($5(+"%4")-("5-(+)".,66",$'"/6(*&,6"+/,5(",5)0$:"%$")-(28")-(1".%*6'"A(",62%+)"5%2/6()(61",0&"6(++8",)","7%6*2("
measure
of the elastic forces in the lungs that tend to collapse the lungs at each instant of
B20$02,6"7%6*2(C"+*A+),$)0,661"6%.(&")-,$")-(1"-,7("!"#$!%&8".0)-0$")-(")-%&,505"5,70)1"789:"2;;""
"
respiration, called the recoil pressure.
$+23<0,+26# 1+&<<,+&# +&=&+<# *(# *%&# 1+&<<,+&# 93<95&# +&62*9>&# *(#
(,*<95&#
(=# 2# -(012+*0&3*""pressure
D$'(&" +),)05"
)&,$+2*&,6" between pleural and alveolar pressures:
The
transpulmonary
is5%$'0)0%$+8"
then the)-("differential
/&(++*&("0+"(E*,6")%")-("(6,+)05"&(5%06"/&(++*&("%4")-("5%2/,&)2($);"F-("
*+23<0,+26# 1+&<<,+&# (=# *%&# 6,3:<" 0+" ,6+%" 5,66('" *+23<1,60(32+?#
1+&<<,+&#"#
""
P(L) = P(A) – P(pl)
eq. 3.1
G0$5(" )-(" 6*$:+" -,7(" ," )($'($51" )%" &(5%06" 0$.,&'+8" 0$46,)0$:" )-(2"
&(E*0&(+" ,$"
0$5&(,+("
0$" )&,$+/*62%$,&1" /&(++*&(;"
F&,$+/*62%$,&1"
Where
P(L)
is trans-pulmonary
pressure,
P(A) is alveolar pressure, and P(pl) is pleural
/&(++*&(" 5,$" A(" 0$5&(,+('" A1" (0)-(&" HI" 0$5&(,+0$:" )-(" /&(++*&(" 0$+0'("
pressure.
&(6,)07(" )%" )-(" /&(++*&(" %*)+0'(" )-(" 6*$:+" %&" !I" A1" '(5&(,+0$:" )-("
/&(++*&("%*)+0'("&(6,)07(")%")-("/&(++*&("0$+0'(")-("6*$:+;"""
If" the lungs were removed from the thoracic cavity, the chest wall would recoil or spring
#4")-("6*$:+".(&("&(2%7('"4&%2")-(")-%&,505"5,70)18")-("5-(+)".,66".%*6'"
outward
and expand to a larger size. To increase or decrease the size (volume) of the chest
&(5%06"%&"+/&0$:"%*).,&'",$'"(J/,$'")%","6,&:(&"+09("789:"@;;""F%"
wall
from this resting position requires an alteration of the external or internal pressures
0$5&(,+("%&"'(5&(,+(")-("+09("K7%6*2(I"%4")-("5-(+)".,66"4&%2")-0+"
&(+)0$:"/%+0)0%$"&(E*0&(+",$",6)(&,)0%$"%4")-("(J)(&$,6"%&"0$)(&$,6"
acting on it. Contraction of inspiratory muscles expands the chest wall from its resting state
/&(++*&(+",5)0$:"%$"0);""?%$)&,5)0%$"%4"0$+/0&,)%&1"2*+56(+"(J/,$'+")-("
and
increased its transpulmonary pressure. Contraction of the expiratory muscles compresses
5-(+)".,66"4&%2"0)+"&(+)0$:"+),)(",$'"0$5&(,+('"0)+")&,$+2*&,6"/&(++*&(;"
?%$)&,5)0%$"%4")-("(J/0&,)%&1"2*+56(+"5%2/&(++(+")-("5-(+)".,66",$'"
the
chest wall and decreases its transpulmonary pressure.
'(5&(,+(+"0)+")&,$+2*&,6"/&(++*&(;"
"
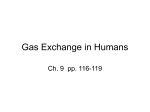
The figure on the left shows the pressures
"
surrounding the lungs and chest wall at resting
###########################################################A2*0#B#C""""
position of the respiratory system [Prs=0]. All
89:,+&#-"&(/&(+($)+")-("6*$:+"0$"+0)*",)"=>?;"F-("40:*&("
"""""""""""6*$:""
#######################"
%$"
)-(" 6(4)" +-%.+" )-(" /&(++*&(+" +*&&%*$'0$:" )-(" 6*$:+"
##########-%&<*#'266########!
pressures
are measured in units of cmH20 *
,$'"5-(+)".,66",)"=>?;""<66"/&(++*&(+",&("2(,+*&('"0$"
"
"
"
"
"
"""""A+<BAD#EA2*0" *$0)+"
and%4"considered
in relative
terms
52L!M" ,$'" 5%$+0'(&('"
0$" &(6,)07("
)(&2+"as,+"compared
#########A-'#BA16EA2*0#
5%2/,&('"
)%" ,)2%+/-(&05"
/&(++*&(;"
<)2%+/-(&05" pressure
to
atmospheric
pressure.
Atmospheric
!!!!!!!!
/&(++*&(" 0+" 5%$7($)0%$,661" 5%$+0'(&('" )%" A(" 9(&%;" F-("
is conventionally considered to be O"zero. The
##################
)&,$+2*&,6"/&(++*&(+"%4")-("6*$:+",$'"5-(+)".,66",&("N
AFBADEA16##################ADBC""""""""""""""""""""""""""""""""###################
transpulmonary
lungs and
,$'"
N5." &(+/(5)07(61;" Npressures
N/6" the
0$'05,)("
,)28" N<8" ,$'" of
# ###############################################
,)2%+/-(&(058"
,67(%6,&"
,$'"
0$)&,/6(*&,6"
/&(++*&("
chest wall are PL and Pcw respectively. Patm,
####################################################################
&(+/(5)07(61;" =>?" 0+" )-(" &(+)0$:" /%+0)0%$" %4" )-("
####################################################################A16#B#E#G!
PA, and Ppl indicate atmospheric, alveolar and
&(+/0&,)%&1" +1+)(2" BN&+PMC;" <)" =>?8" )-(" &(+/0&,)%&1"
#
intrapleural pressure respectively.
2*+56(+",&("&(6,J('",$'")-("(6,+)05"&(5%06"%4")-("6*$:+"0+"
(E*,6" 0$" 2,:$0)*'(" A*)" %//%+0)(" 0$" '0&(5)0%$" )%" )-("
(6,+)05"&(5%06"%4")-("5-(+)".,66",$'"0$)&,/6(*&,6"/&(++*&("0+"+*A,)2%+/-(&058",)",A%*)""Q"R"52L
Alveolar
pressure is the pressure of the air inside the lung alveoli.!M;""<)")-("($'"%4","$%&2,6"
When no air is flowing into
A&(,)-8",)"=>?8")-(&("0+"$%",0&46%."0$"%&"%*)"%4")-("6*$:+",$'"$%"/&(++*&(":&,'0($)"A().(($")-(",)2%+/-(&(",$'",67(%60")%"
or'&07("
out,0&46%."
of the
lungs, the pressures in all parts of the respiratory tree, all the way to the alveoli,
)-(" 46%." %4" ,0&" 0$)%" )-(" 6*$:+;" #$" %&'(&" )%" '&,." ,0&" 0$)%" )-(" 6*$:+8" ," '044(&($5(" 0$" ,67(%6,&" ,$'" ,)2%+/-(&05"
are
equal to atmospheric pressure, which is considered to be zero reference pressure in the
/&(++*&("2*+)"A("5&(,)('"A1")-("5%$)&,5)0%$"%4"0$+/0&,)%&1"2*+56(+;"
"
airways-that is, 0 centimeters water pressure. To cause inward flow of air into the alveoli
S" $%)(T" 0$)&,/6(*&,6" /&(++*&(" ,)" =>?" 0+" 2%+)" )(J)A%%3+" 0+" 0$'05,)('" ,+" QR" 52" L!M;" #)" 0+" 02/%&),$)" )%" $%)(" )-,)" 0$" )-(" */&0:-)" 6*$:8"
0$)&,/6(*&,6"/&(++*&(",)"=>?"7,&0(+"'(/($'0$:"%$".-(&("0)"0+"2(,+*&('@"0)"0+"QU",)")-("A,+(",$'"QV"52"L!M",)")-(",/(J"%4")-("6*$:+;"
during
inspiration, the pressure in the alveoli must fall to a value slightly below atmospheric
pressure
(below 0).
!"
The Figure below demonstrates that during normal inspiration, alveolar pressure decreases to
about -1 cmH2O). This slight negative pressure is enough to pull 0.5 liter of air into the lungs
in the 2 seconds required for normal quiet inspiration. During expiration, opposite pressures
occur: The alveolar pressure rises to about +1 cmH2O, and this forces the 0.5 liter of inspired
air out of the lungs during the 2 to 3 seconds of expiration.
*
The measurement of pressure in the respiratory system are often expressed in cmH2O. The
relationship of cmH2O with other pressure units is: 1mmHg = 1.36 cmH2O = 0.133 kPa 3-3
%):.$%)0"+,3+"&-$%)##2%)-5%&6!)"'-7)'8))"-'4)-&'/(#$4)%)-&"6-'4)-&09)(0!-;)")0+3;'$0,)/8""9,$0"/%$2$54"6%)00.%)"
4%3/$)5+"$0"3<<*16'$0,)/";="+,)"<*5+%3<+$*5"*-"+,)"$506$%3+*%="1.0<')08"">*5+%3<+$*5"*-"+,)"$506$%3+*%="1.0<')0")?635/0"+,)"
<,)0+"73''&"'*7)%$54"+,)"6%)00.%)0"$5"+,)"+,*%3<$<"<32$+="@;*+,"$5+%36').%3'"35/"3'2)*'3%"6%)00.%)0"/)<%)30)A"B"<*50$/)%"
C*=')D0"'37E8""F+"$0"$16*%+35+"+*"366%)<$3+)"+,)-#):2)";)-(<-)9)"'#=-1.0<')"<*5+%3<+$*5-%)0.'+0"$5";4&"5)-!"-'4(%&;!;9(02/)-')3/$54"+*"3";4&"5)-!"-&09)(0&%-$%)##2%)-+,3+"$5"+.%5"6%*2$/)0"+,)"/%$2$54"6%)00.%)"-*%-&!%-<0(8"$5+*"+,)"'.540">!,)=/2#;0)-;("'%&;'!("-→
→-∆
∆-?→
→-∆
∆-@→
→-&!%-<0(8A,"
9,)"-*''*7$54"-$4.%)"0,*70"2*'.1)&"6%)00.%)"35/"3$%-'*7"<,354)0"/.%$54"3"0$54')"$/)3'$G)/"%)06$%3+*%="<=<')8"
"
• #+" +,)" 0+3%+" *-" $506$%3+$*5&" +,)" /$36,%341" <*5+%3<+0" 35/" /)0<)5/0&" )?635/$54" +,)"
+,*%3<$<" 2*'.1)8" " 9,)" /)0<)5+" *-" +,)" /$36,%341" <*16%)00)0" +,)" 3;/*1$53'"
<*5+)5+0"35/"/)<*16%)00)0"+,)"<*5+)5+0"*-"+,)"+,*%3<$<"<32$+=8"H$+,")?6350$*5"*-"
Therefore,
at rest the respiratory muscles are relaxed and
+,)"+,*%3<$<"<32$+="35/"$+0"/)<*16%)00$*5&";*+,"$5+%36').%3'"6%)00.%)"35/"3'2)*'3%"
the elastic recoil of the lungs is equal in magnitude but
6%)00.%)" /)<%)30)8" #'2)*'3%" 6%)00.%)" /)<%)30)0" +*" 3" 0.;B3+1*06,)%$<" ')2)'" 35/"
opposite
in direction to the elastic recoil of the chest wall
+,)"6%)00.%)"4%3/$)5+"-*%"+,)"-'*7"*-"3$%"$5+*"+,)"'.540"$0")0+3;'$0,)/8""#$%"-'*70"$5+*"
and+,)"
intrapleural
is sub-atmospheric,
at about
- 5 %$0)0" +*" +,)"
'.540" 35/" pressure
'.54" 2*'.1)"
$5<%)30)0" .5+$'" +,)" 3'2)*'3%"
6%)00.%)"
cmH20.
At the
ofKLMN"
a normal
breath, 4%3/$)5+"
there is
3+1*06,)%$<"
')2)'"end
IJ" <1"
7,)5" +,)" 6%)00.%)"
-*%" no
-'*7" *-" 3$%" $5+*" +,)"
'.540"<)30)0"+*")?$0+8"
airflow in or out of the lungs and no pressure gradient
"
between
the atmosphere and alveoli to drive airflow the
• #+"+,)")5/"*-":.$)+"$506$%3+$*5&"$5+%36').%3'"6%)00.%)"%)3<,)0"3;*.+"B"O"<1"KLJ&"35/"
flow+,)"+%3506.'1*53%="6%)00.%)"/$0+)5/$54"+,)"'.540"$5<%)30)0"+*"O"<1"K
of air into the lungs. In order to draw air into the LM""IPQ"R""P#""
lungs,
difference in alveolar
! Pa6'""R""J"!"@-O"A"R"O"<1"K
LMN8"" and atmospheric pressure
"
must
be created by the contraction of inspiratory
•muscles.
S.%$54":.$)+")?6$%3+$*5&"+,)"<=<')"$0"%)2)%0)/&"+,)"$506$%3+*%="1.0<')0"%)'3?"35/"+,)"
$573%/")'30+$<"%)<*$'"*-"+,)"'.540"%)0.'+0"$5"/)-'3+$*5"*-"+,)"'.5408"S.%$54"/)-'3+$*5&"
At the
end of quiet inspiration, intrapleural pressure
+,)"'.540"35/"<,)0+"73''"1*2)"30"*5)".5$+8""#$%-'*7"*.+"*-"+,)"'.540"<)30)0"7,)5"
3'2)*'3%"6%)00.%)"):.3'0"3+1*06,)%$<"6%)00.%)"@J"<1"K
LMA8"
reaches about - 8 cm H20, and the transpulmonary
"
pressure
distending the lungs increases to 8 cm H2O
BC("#!6)%-3(D0)E#-0&8="F5"3"<'*0)/"0=0+)1"7,)%)"+,)"5.1;)%"*-"430"1*')<.')0"$0"
[PL
= PA - Ppl = 0-(-8) = 8cmH2O].
<*50+35+&"3+"35="<*50+35+"+)16)%3+.%)&"+,)"6%)00.%)")?)%+)/";="3"430"23%$)0"$52)%0)'="
7$+,"+,)"2*'.1)"*-"+,)"4308"9,)%)-*%)"30"+,)"2*'.1)"*-"430"$5<%)30)0&"+,)"6%)00.%)"
During
quiet expiration, the cycle is reversed, the
)?)%+)/";="+,)"430"/)<%)30)08">*52)%0)'=&"+,)"6%)00.%)"$5<%)30)0"30"+,)"2*'.1)"
inspiratory muscles relax and the inward elastic recoil of
/)<%)30)08"
the lungs results in deflation of the lungs. During
"
deflation,
the lungs and chest wall move as one unit.
12)#'!("#=-"TA"H,3+"$0"+,)"/%$2$54"6%)00.%)"-*%"3$%"+*"-'*7"$5+*"+,)"'.540U"
Airflow
out of the lungs ceases when alveolar pressure
LA"H,3+"<%)3+)/"+,$0"/%$2$54"6%)00.%)U"!A"K*7"<*1)"+,)"3'2)*'3%"6%)00.%)"/)<%)30)"
07$540";.+"6').%3'"6%)00.%)"/)<%)30)"$0"<*5+$5.*.0"+,%*.4,*.+"$506$%3+$*5U"
equals atmospheric pressure (0 cm H2O).
!"#$!%&'!("""""""""""")*$!%&'!(""
"
"
"
The extent
to which the lungs will expand for each unit increase in transpulmonary pressure
"
"
(if enough time is allowed to reach equilibrium) is called the lung compliance. Therefore lung
F5"*%/)%"+*")?635/"+,)"'.540&"+,)"$506$%3+*%="1.0<')0"1.0+"*2)%<*1)"+7*"()="-3<+*%0V"TA";(/$0!&";)-(<-'4)-02"5#"35/"LA"
compliance
is the change in volume for any given pressure.
&!%8&D#-%)#!#'&";)"13$5'="$5"+,)"-*%1"*-"-%$<+$*53'"%)0$0+35<)"+*"-'*7"*-"3$%"+,%*.4,"+,)"3$%73=0"@0))".6<*1$54"')<+.%)"*5"
3$%73="%)0$0+35<)A8"9,)"-*%<)"%):.$%)/"+*"*2)%<*1)"+,)"<*16'$35<)"*-"+,)"'.540"$0"$5/$<3+)/";="+,)"$5+%36').%3'"6%)00.%)"6'*+"
,3+<,)/"'$5)"TBW8"9,)"0*'$/"'$5)"TDWD&"$5/$<3+)0"+,)"-*%<)"%):.$%)/"+*"*2)%<*1)";*+,"+,)"<*16'$35<)"*-"+,)"'.540"35/"3$%73="
3.2. %)0$0+35<)8"9,)"3%)3";)+7))5"+,)"+7*"'$5)0"$5/$<3+)0"+,)"-*%<)"%):.$%)/"+*"*2)%<*1)"3$%73="%)0$0+35<)8"
Pulmonary compliance
"
Compliance is the measure of stretching
capability of matter. Then, compliance is the
inverse of elastic recoil. The compliance of the
lung is the relationship between lung volume
changes and changes in transpulmonary pressure
and usually given by a compliance diagram
(Figure on the right). As can be depicted in the
Figure, the relation is different for inspiration and
expiration. Each curve is recorded by changing
the transpulmonary pressure in small steps and
allowing the lung volume to come to a steady
!"
3-4
level between successive steps. The two curves are called, respectively, the inspiratory
compliance curve and the expiratory compliance curve, and the entire diagram is called the
compliance diagram of the lungs.
The pressure-volume curve shows when a positive pressure is delivered to the airways during
inspiration (inflation) from zero volume that the pressure increases until the opening pressure
of the lungs is reached, at which point the small airways and alveoli begin to open. Once
opening pressure is reached, lung volume increases as pressure is increased until total lung
capacity is reached. During expiration (deflation), as airway pressure falls, lung volume
decreases. But the pressure-volume relationship during inspiration is different from that
during expiration.
The lung volume change per unit pressure is known as pulmonary compliance (C) and is
calculated using the following equation, where ΔV is the change in volume, and ΔP is the
change in pleural pressure:
C = ΔV / ΔP
eq. 3.2
For example if a patient inhales 500 mL of air and has an intrapleural pressure before
inspiration of – 5 cm H2O and -8 cm H2O at the end of inspiration. Then:
C= (0.5L)/ (-5cmH2O – (-8 cmH2O)) = 0.5/3 = 0.17 L/cmH2O
This means that the total compliance of both lungs together in the normal adult human being
averages about 200 milliliters of air per centimeter of water transpulmonary pressure. That is,
every time the transpulmonary pressure increases 1 cmH2O, the lung volume, after 1 to 2
seconds, will expand 200 ml.
The elastic forces of the lungs determine the characteristics of the compliance diagram. These
can be divided into two parts:
1) elastic forces of the lung tissue itself and
2) elastic forces caused by surface tension of the fluid that lines the inside walls of the
alveoli and other lung air spaces.
Mainly elastin and collagen fibres interwoven among the lung parenchyma determine the
elastic forces of the lung tissue. In deflated lungs, these fibres are in an elastically contracted
and kinked state; then, when the lungs expand, the fibres become stretched and unkinked,
thereby elongating and exerting even more elastic
force.
The elastic forces caused by surface tension are much
more complex. The significance of surface tension is
shown in Figure (left curve), which compares the
compliance diagram of the lungs when filled with
saline solution and when filled with air. When the
lungs are filled with air, there is an interface between
the alveolar fluid and the air in the alveoli. In the case
of the saline solution - filled lungs, there is no air-fluid
3-5
interface; therefore, the surface tension effect is not present - only tissue elastic forces are
operative in the saline solution-filled lung.
Note that transpleural pressures required to expand air-filled lungs are about three times as
great as those required to expand saline solution-filled lungs. Thus, one can conclude that the
tissue elastic forces tending to cause collapse of the air-filled lung represent only about one
third of the total lung elasticity, whereas the fluid-air surface tension forces in the alveoli
represent about two thirds.
The fluid-air surface tension elastic forces of the lungs also increase tremendously when the
substance called surfactant is not present in the alveolar fluid.
Review Surface Tension Principles (see Section 2):
When water forms a surface with air, the water molecules on the surface of the water have an
especially strong attraction for one another. As a result, the water surface is always
attempting to contract, meaning that the force of surface tension acts in the plane of the airliquid boundary to shrink or minimize the liquid-air interface. This is what holds raindrops
together: that is, there is a tight contractile membrane of water molecules around the entire
surface of the raindrop.
Now let us reverse these principles and see what happens on the inner surfaces of the alveoli.
Here, the water molecules are attracted to one another forcing the air out of the alveoli
through the bronchi and, in doing so, the alveoli tend to collapse. The net effect is to cause an
elastic contractile force of the entire lungs, which is called the surface tension elastic force.
However, alveoli do not collapse during expiration because the alveoli surface is covered
with surfactant, which diminish the effect of the surface tension elastic force.
Surfactant is a surface active agent in water, which means that it greatly reduces the surface
tension of water. It is secreted by special surfactant-secreting epithelial cells called type II
alveolar epithelial cells, which constitute about 10 per cent of the surface area of the alveoli.
These cells are granular, containing lipid inclusions that are secreted in the surfactant into the
alveoli.
Surfactant is a complex mixture of several phospholipids, proteins, and ions. The most
important components are the phospholipid dipalmitoylphosphatidylcholine, surfactant
apoproteins, and calcium ions. The dipalmitoylphosphatidylcholine, along with several less
important phospholipids, is responsible for reducing the surface tension. It does this by not
dissolving uniformly in the fluid lining the alveolar surface. Instead, part of the molecule
dissolves, while the remainder spreads over the surface of the water in the alveoli. This
surface has from one twelfth to one half the surface tension of a pure water surface.
3-6
The surface tension of different water fluids is approximately the following:
pure water
80 dynes/cm *
normal fluids lining the alveoli, without surfactant
50 dynes/cm
normal fluids lining the alveoli with normal amounts of surfactant
5 - 30 dynes/cm
* 1 dyne/cm = 0.001 N/m
The pressure to collapse generated by the alveoli can be calculated by Laplace Law (section
2, eq. 2.11), thus is inversely affected by the radius of the alveoli. If the radius of the alveoli
increases, then the pressure to collapse diminishes. If the alveoli were lined with water the
pressure would increase 3.5-fold.
Effect of alveolar radius (R) and surfactant in the alveolar pressure (P) * needed to keep the
alveoli in an open state:
Alveolar radius (µm)
50 - small alveoli
100 - average normal size
200 - large alveoli
Alveoli
with
Pure
water Alveoli lined with normal
surfactant
T = 70 dynes/cm
T = 20 dynes /cm
P = 28x103 dynes/cm2
P = 8 x103 dynes/cm2
P = 28 cmH2O
P = 8 cmH2O
P = 14x103 dynes/cm2
P = 4x103 dynes/cm2
T = 14 cmH2O
P = 4 cmH2O
P = 7x103 dynes/cm2
P = 2 x103 dynes/cm2
P = 7 cmH2O
P = 2 cmH2O
* P (pressure) = 2 x surface tension (T) / Radius (R) ; 1 dyne/cm2 = 0.00102 cmH2O
The smaller the alveoli the higher the pressure acting on it, meaning that smaller alveoli have
greater tendency to collapse and to empty into larger alveoli.
If some alveoli were smaller and other large, smaller alveoli would tend to collapse and cause
expansion of larger alveoli. This does not happen because normally larger alveoli do not exist
adjacent to small alveoli.
Alveoli share the same septum wall and all alveoli are surrounded by fibrous tissue septa that
act as additional splints. This creates a radial traction that increases as the alveoli becomes
smaller, resisting further collapse, implying that it is the tension of the adjacent tissue that
prevents different sized alveoli from collapsing into each other, rather than the ability of
surfactant to counteract the Laplace law.
3-7
During spontaneous breathing the lungs are inflated by negative pressure. The transmission
of force throughout lung tissues causes volume expansion. At low lung volumes, the lung
expansion is also resisted by the surface tension of the thin layer of lining fluid of alveoli and
airways.
Surfactant reduces surface tension. When alveoli of
different sizes are connected, the surfactant creates a
steady-state and equalizes the pressure by conforming
the surface tension. As alveolus becomes smaller
surfactant molecules are squeezed together increasing
their concentration, which reduces surface tension even
more.
3.3. “Work” of breathing
The compliance work is the force needed to expand lung against its elastic properties. Almost
all muscle contractions occur during inspiration, whereas expiration is practically a passive
process caused by elastic recoil of the lung and chest cage structures. That is to say, all work
is stored as potential energy, and no work is dissipated as heat. The factors influencing elastic
recoil are:
-
-
the intrinsic elasticity of fibres, dependent on age and pathology (emphysema reduces
elastic recoil);
surface tension, being the surfactant responsible for 70% of elastic recoil, in a way
that increased surface tension increases elastic recoil and larger alveoli reduced
surface tension;
lung volume (the higher the volume the more stretch fibres are inducing a greater
recoil);
and respiratory rate (increased respiratory rate decrease work due to recoil).
In respiration work of breathing can be calculated by multiplying the volume of expansion
times the average pressure required to cause the expansion (interpleural pressure):
Work = volume x pleural pressure.
3-8
The work of inspiration can be divided into 3 fractions:
1) that required to expand the lungs against the lung and chest elastic forces compliance work or elastic work
work against non-elastic resistance, which is mainly frictional and represents an
additional pressure that is required to overcome:
2) the viscosity of the lung and chest wall structures, – tissue resistance work
3) airway resistance against the movement of air into lungs, frictional resistance to gas
flow – airway resistance work.
The compliance work has been discussed above (sub-section 3.2 eq. 3.1). It measures the
ability of the lung to stretch. In the compliance diagram the inspiration curve shows that a
progressive change in pleural pressure and lung volume during inspiration occurs. Note that
in the compliance diagram the curves are not linear.
The figure exemplifies how compliance value of
an healthy adult can be calculated. The slope of
the line is compliance
The meaning of the coordinates used to evaluate
the values of volume and pressure will be
discussed further.
It can be easily calculated that:
C= 1.8L/0.65 cm H2O = 0.28 L/cm H2O
The tissue resistance work expresses the work expenditure required to overcome the
viscosity of the lungs, such as viscous forces within tissues as they slide over each other.
Tissue resistance is about 20% of total resistance.
The airways resistance work is the work required to overcome the resistance to airflow
through the respiratory ways. Meaning that is the work required to move air in &out the
lungs.
Mucous provides a physical barrier to the passage of air. Also the diameter of the airways
produces resistance.
Airway resistance (AWR) is affected by:
-
lung volume, the greater the lung volume the lower the AWR, which is opposite to
elastic recoil;
3-9
-
bronchial smooth muscle tone - increased tone increases AWR;
density and viscosity of gas
respiratory rate – increased respiratory rate given the same minute volume, increases
work due to airflow resistance.
The airway resistance (R (awr)) is related to the pressure drop of the inspiratory flow Q in the
airway duct or pipe relative to the flow rate. Thus:
R (awr) = (Palveolar – Patm) /Q
(F= ΔP x 1/R (awr))
eq. 3.3
In the airways like Poiseuille law, the product of the pressure drop and the area of the pipe is
the force required to overcome the frictional forces that tend to retard the flow in the pipe
segment. For a given flow rate Q along a length (l) of the pipe, the pressure drop required to
overcome frictional losses decreases as the fourth power of the pipe radius (r).
ΔP = Q 8 η l / π r4
eq. 3.4
Where η is the viscosity coefficient measured in units of dyn (sec/cm2) or poise
Thus :
&3/*+4-#*+5#63*0)*+4-#
R(awr) = 8 η l / π r4
eq. 3.5
/0)-+0/7/3/)8" ,-" ()%%'+" )./" $0'1#-#'$" %&'" ')$'" 2#%&" 2&" ()%%'+" 1)." 3'" $%+'%1&'/" ,+"
One might think that because the terminal bronchioles are very narrow they would represent
'",-"'6)$%).1'",+"'6)$%#1"+'1,#68"1,(06#).1'9:;'6)$%).1'4""63*0)*+4-"#$"0+,0'+%<",-"()%%'+"
/#$%,+%#,.")./"%&'"%'./'.1<",-"()%%'+"%,"+'%*+."%,"#%$"+'$%#.="$&)0'")-%'+"/'-,+()%#,."3<")."
very high resistance. However, because there are so many (>106) and because they are in
"%&'"6*.=$")+'",-%'."/'$1+#3'/"3<"'>)(#.#.="%&'"0+'$$*+'@7,6*('"1&)+)1%'+#$%#1$",-"%&'"
parallel they represent a relatively small portion of the total Raw.
."%&'+'"#$".,"-6,2",-")#+")./"%&'"+'$0#+)%,+<"(*$16'$")+'"+'6)>'/4"" ?&'"%+).$0*6(,.)+<"
-6'1%$"#."()=.#%*/'"%&'"'6)$%#1"+'1,#6"0+'$$*+'",-"%&'"6*.=$4"
""""""""""""""""""""""""""""""""""""&#=&"1,(06#).1'"B'(0&<$'()C"
""""""""""""""""""""""""""""""""""""""""""""
+>0#?2<@#
"
*6(,.)+<" 0+'$$*+'"
'/" -,+" )" +).='" ,-"
$" +'6)%#,.$�" #$"
B.,")#+-6,2C"/*+#.="
<2# )'# AB2"" " D$"
$'$8" 6*.=" 7,6*('"
$�"#$"1*+7#6#.')+4""
'" 6*.=$" )+'" &#=&6<"
"#."%+).$0*6(,.)+<"
" #.1+')$'$" #." 6*.="
#=&" 6*.=" 7,6*('$8"
.$#3#6#%<")./"-,+")."
)+<"0+'$$*+'8"%&'+'"
?&'" (')$*+'" ,-"
1)66'/" %&'" 0)*)/4#
)./" #$" /'%'+(#.'/"
6*('" 1*+7'" ,-" %&'"
IJKC".')+"LM54"""
"
.,+()6"
""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""∆S""""""""""
∆R
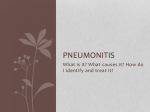
Compliance work and airway resistance
change in common chronic lung diseases
such as emphysema, asthma and fibrosis.
In fibrosis, lung tissues become very stiff,
thus the transpleural pressure increases
tremendously, decreasing compliance.
""""""""
"""""""H*.=
"""""""S,6*('""""""" "
""""""""""""5H"9"$6,0'"9"∆S";"∆R """"""""""""""""""""""""""
In turn in emphysema and asthma, which
"""""""""""""""""""""""""""""""""""""""""""""∆S""""""
are diseases that obstruct the airways, the
#
airway resistance work is especially
"""""""""""""""""""""""""""""""""""""""
""""""""""""""""""""""""""""""""""""∆R""""""""""""""""""""""""""""""""
increased.
""""""6,2"1,(06#).1'""""""""""""""
"""""""""""""""""""""""""" """"""""""""""""""""B0*6(,.)+<"-#3+,$#$C
""""""""""""""""""""""""
""""" ?+).$0*6(,.)+<"R+'$$*+'""
#
" /#--'+'.%" $#N'$8" 1,(06#).1'" #$" '>0+'$$'/" 0'+" *.#%" 6*.=" 7,6*('4" " ?&#$" (')$*+'('.%" #$"
-#2=(G-0#'.#):-#<=+>0#
06#).1'",-"%&'"6*.=$",."
,,.",."%&'"+#=&%4"
3-10
3.4. Distribution of ventilation
Ventilation is not uniformly distributed in the lung, in large part because of the effects of
gravity. In the upright position, alveoli near the apex of the lung are more expanded than
alveoli at the base.
Gravity pulls the lung downward and away from the chest wall.
-
-
-
As a result, pleural pressure is less at the apex than at the base of the lung, and static
translung pressure (PL = PA - Ppl) is increased and alveolar volume at the apex
increases.
Because of the difference in alveolar volume at the apex and at the base of the lung,
the alveoli at the lung base are located along the steep portion of the pressure-volume
curve (see previous figure), and they receive more of the ventilation (i.e., they have
greater compliance). In contrast, the alveoli at the apex are closer to the top of the
pressure-volume curve, therefore have lower compliance, receiving proportionately
less of the ventilation.
The effect of gravity is less pronounced when one is supine (lying on one’s back) than
upright, and it is less when one is supine than prone (having the front or ventral
surface downwards). This is because the diaphragm is pushed cephalad (head
direction) when one is supine, and it affects the size of all of the alveoli.
In addition to gravitational effects on the distribution of ventilation, the ventilation in the
alveoli is not uniform. This is caused by variable airway resistance (R) or compliance (C),
and can be described by the time constant (t):
t=RxC
Alveolar units with long time constants fill and empty
slowly.
Thus, an alveolar unit with increased airway resistance
or increased compliance will take longer to fill and
longer to empty.
In normal adults, the respiratory rate is about 12 breaths
per minute, the inspiratory time is about 2 seconds, and
the expiratory time is about 3 seconds. In normal
individuals this time is sufficient to approach
equilibrium (see Figure).
The figure shows the individual resistance and
compliance of three different lung units. In the lower
graph are shown the volume of these three lung units as
a function of time. In the upper schema, the normal lung
has a time constant (t) of 0.56 second. This unit reaches
3-11
97% of final equilibrium in 2 seconds (the normal inspiratory time) as can be depicted in the
lower graph. The unit at the right has a twofold increase in resistance; hence its time constant
is doubled. That unit fills more slowly and reaches only 80% equilibrium during a normal
breath (graph). The unit is underventilated. The unit on the left has reduced compliance
(stiff), which acts to reduce its time constant. This unit fills faster than the normal unit but
receives only half the ventilation of a normal unit.
Single-breath N2 test
The single-breath N2 test can be used to assess the uniformity of ventilation. The subject
takes a single maximal inspiration of 100% O2. During the subsequent exhalation, [N2] in the
exhaled air is measured. Air (100% O2, 0% N2) initially exits from the conducting airways;
then [N2] begins to rise as alveolar emptying occurs. Finally, there is a plateau [N2] as only
the alveoli that contain N2 empty.
3.5. Pulmonary volumes and capacities
The figure below list 4 lung volumes, which when added together equal the maximum
volume to which the lungs can be expanded.
VT - Tidal volume – is the volume of air inspired or expired with each normal breath; it
amounts to about 500 ml.
ICV - The inspiratory reserve volume: maximum extra volume of air that can be inspired
over and above the normal tidal volume; approximately 3000 ml.
ERV - The expiratory reserve volume: the maximum extra volume of air that can be
expired by forceful expiration after the end of the normal tidal expiration; approximately
1000 ml.
RV - The residual volume: the volume of air remaining in the lungs after the most forceful
inspiration; approximately 1200 ml.
3-12
The Figure also indicates 4 capacities, which correspond to combinations of two or more
volumes.
IC - The inspiratory capacity = VT + IRV. This is the amount of air (approx. 3500 ml) a
person can breathe in beginning at the normal expiratory level and distending the lungs to the
maximum amount.
FRC - The functional residual capacity = ERV + RV. This is the amount of air that
remains in the lungs at the end of normal expiration (approx. 2300 ml).
VC - The vital capacity = IRV + VT + ERV. This is the maximum amount of air a person
can expel from the lungs after first filling the lungs to their maximum extend and then
expiring to the maximum extend (about 4600 ml)
TLC - The total lung capacity = VC + RV. This is the maximum volume to which the lungs
can be expanded with the greatest possible effort (about 5800 ml)
All pulmonary volumes and capacities are about 20-25% less in women than in men.
Abbreviations and some important relationships:
VC = IRV + VT + ERV
VC = IC + ERV
IC = VT + IRV
FRC = ERV + RV
TLC = VC + RV
TLC = IC + FRC
Calculating TLC, FRC and RV – The helium dilution method
The FRC, which is the volume of air that remains in the lungs at the end of each normal
expiration, is important to lung functions. Its value changes in some types of pulmonary
diseases. However, this capacity can only be measured indirectly, as residual volume cannot
be measured directly by spirometry.
This can be measured using the He dilution method, as follows:
A spirometer of known vol is filled with air mixed with He at a known concentration. Before
breathing from the spirometer, the person expires normally. At the end of this expiration the
remaining vol in the lungs is equal to the FRC - functional residual capacity. At this point the
subject starts breathing from the spirometer and the mixture of air and He begin to mix with
gases in the lungs including the functional residual capacity gases.
3-13
The FRC can then be calculated using the formula:
FRC = ([He]i / [He]f -1) / Vi (spirometer)
Measurement of dead space and volumes
Dead space consist of the passages where no gas exchange takes place, such as nose,
pharynx and trachea; the volume of air that fills these passageways is not useful for gas
exchange process as is called the dead volume.
There are two types of dead space, anatomic dead space and physiological dead space.
Anatomic dead space ventilation
Anatomic dead space (VD) is composed of the volume of gas that fills the conducting
airways. Thus,
V(T) = V(D) + V(A)
where V refers to volume and the subscripts T, D, and A refer to tidal, dead space, and
alveolar.
Or if one considers volumes / unit of time (n):
V(T) x n = (V(D) x n) + (V(A) x n)
V* denotes a volume per unit of time (n). Thus,
V*(E) = V*(D) + V*(A)
where V*(E) is the exhaled minute volume, V*(D) is the dead space per minute, and V*(A) is
alveolar ventilation per minute.
Anatomical dead space measurement
Dead space can be measured likely FRC and RV, by Fowler’s method that consists of
inhaling in a single breath, pure oxygen (O2 100%). Some O2 also mixes with the alveolar air
but does not completely replace this air. Then the person expires through a rapidly recording
N2 meter, which makes a record as shown in the Figure below.
The first part of the exhaled air comes from the dead space regions where the air has been
completely replaced by O2. Therefore in the first part of the record only O2 appears. This
volume contains 100% O2 and 0% N2 because it has not participated in any gas exchange.
Then N2 starts to rise meaning that alveolar air begins to reach the N2 meter, and rapidly
rises, because alveolar air contains large amounts of N2 begins to mix with the dead space
air. After a while and more air expired all the dead space air has been expired from the
passageways and only alveolar air remains. The recorded N2 reaches a plateau level equals to
its concentration in alveoli.
3-14
!"#$%&#
9###############:99#################"99#############;99###############<99###############=99#
'()*+,-./(#/0#*1,2#3"#
4+,#25*+,26#$78&#
Thus, dead space (V(D) quantification can be obtained using the area delimited by the
recorded N2 curve, by the following relationship:
V(D) = (Gray area x V(E)) / (Pink area + Gray area)
Where V(E) is the total volume of exhaled air.
Assuming that
V(E) = 500 ml
gray area = 30 cm2
pink area = 70 cm2
V(D) = 30/(30+70) x 500 ml = 150 ml
The normal dead space air in a young adult is about 150 ml. This value increases slightly with
age.
Rate of alveolar ventilation
Alveolar ventilation per minute is the total volume entering the alveoli and adjacent gasexchange areas per minute. It is equal to the respiratory rate frequency/ minute times the
amount of new air entering per minute/each breath:
V(A) = frequency RR x (V(T) – V(D))
Thus with a normal tidal volume of 500 ml; normal dead space of 150 ml and RR of 12
breaths/min, alveolar ventilation is:
V(A) = 12 x (500 -150) = 4200 ml/min
Alveolar ventilation is the major factor determining the concentration of O2 and CO2 in the
alveoli.
3-15
Example:
If the dead space is 150 mL and tidal volume increases from 500 to 600 mL for the same
minute ventilation, what is the effect on dead space ventilation?
1) V(T) = 500 ml == V(D) = 150 ml / 500 ml x V*(E) == V(D) = 0.30 x V*(E)
2) V(T) = 600 ml == V(D) = 150 ml / 600 ml x V*(E) == V(D) = 0.25 x V*(E)
As tidal volume increases, dead space ventilation decreases for the same minute ventilation.
In a healthy adult, the volume of gas contained in the conducting airways at functional
residual capacity (FRC) is approximately 200 mL, as compared with the 3 L of gas in the
entire lung. The ratio of the volume of the conducting airways (dead space) to tidal volume
describes the fraction of each breath that is wasted in "filling" the conducting airways.
This volume is related to tidal volume (V(T)) and to minute ventilation (V*(E)) in the
following way:
V*(D) = V(D) / V(T) x V*(E)
Dead space ventilation (V(D)) thus varies inversely with tidal volume (V(T)).
The larger the tidal volume, the smaller the dead space ventilation.
Normally, V(D)/V(T) is 20% to 30% of minute ventilation.
Physiological Dead Space Ventilation
The total volume of gas in each breath that does not participate in gas exchange is called the
physiological dead space ventilation. The physiological dead space includes the alveoli,
which are partially functional or non-functional (not perfused*) because of absent or deficient
blood flow through adjacent pulmonary capillaries. In a normal person the anatomical and
physiological dead spaces are nearly equal.
Physiological dead space determination
Dead space in the lungs can be determined by measuring PCO2 in alveolar gas and in mixed
expired gas. Exhaled gas is collected in a bag over a period of time, and arterial PCO2 (which
is the same as alveolar PCO2) and the PCO2 in the collection bag (PECO2) are measured.
CO2 in mixed expired gas is diluted relative to that in alveolar gas, and the extent of the
dilution is a function of the wasted ventilation. Dead space volume as a function of tidal
volume (VD/VT) is described by the following equation:
V(D) = V(T) x (P(A)CO2 - P(E)CO2 ) / P(A)CO2
*
Perfusion is the process by which deoxygenated blood passes through the lung and becomes
oxygenated.
3-16
This is called the Bohr dead space equation, named after the physiologist Christian Bohr.
3.6. Pulmonary circulation
Deoxygenated blood from the right atrium enters the right ventricle and it is then pumped
under low pressure (9 to 24 mm Hg) into the pulmonary artery. The arteries of the pulmonary
circulation are the only arteries in the body that carry deoxygenated blood. The deoxygenated
blood in the pulmonary arteries >500 µm passes to arterioles, 10 to 200 µm; and to
capillaries, <10 µm that end in a complex network of capillaries. The sequential branching
pattern of the pulmonary arteries follows the pattern of airway branching. The functions of
the pulmonary circulatory system are to:
(1) reoxygenate the blood and dispense with CO2,
(2) aid in fluid balance in the lung, and
(3) distribute metabolic products to and from the lung.
Oxygenation of red blood cells occurs in the capillaries that surround the alveoli, where the
pulmonary capillary bed and the alveoli come together in the alveolar wall in a unique
configuration for optimal gas exchange (see next Figures). Gas exchange occurs through this
alveolar-capillary network.
The total blood volume of the pulmonary circulation is about 500 mL, which is about 10% of
the circulating blood volume. Approximately 75 mL of blood is present in the alveolarcapillary network of healthy adults at any one time. During exercise, this blood volume
increases to 150 to 200 mL because of the recruitment of new capillaries secondary to an
increase in pressure and flow. The oxygenated blood leaves the alveolus through a network of
small pulmonary venules (15 to 500 µm in diameter) and veins. These small vessels merge in
pulmonary veins (>500 µm in diameter) through which the oxygenated blood returns to the
left atrium of the heart.
Alveolar capillaries reside within the inter-alveolar septa, and they are very sensitive to
changes in alveolar pressure but not to changes in pleural or interstitial pressure.
Positive pressure ventilation increases alveolar pressure and compresses these capillaries and
thus blocks blood flow.
3-17
Electron micrograph of an alveolar
wall showing the path for diffusion of
O2 and CO2. The thin side of the
alveolar wall barrier (short arrows);
alveolar capillary (C), red blood cell
(EC). The thick side of the gas
exchange barrier has an accumulation
of fibrils and matrix (FB). The
alveolar epithelium (EP) is separate
from
the
alveolar
capillary
endothelium (EN) by interstitial space
(IN). As long as the red blood cells
are flowing, O2 and CO2 diffusion
probably occurs across both sides of
the air-blood barrier. Gas exchange
pathway: 2 -tissue barrier; 3 - blood
plasma; and 4 - erythrocyte. (8600
magnification).
Schematic showing the exchange surface of alveoli.
The path is very small < 1 µm.
3-18
Structure of the Alveolar-Capillary Network
The sequential branching of the pulmonary arteries culminates in a dense network of
capillaries that surround alveoli. This alveolar-capillary network has an alveolar surface area
of about 70 m2 (about the size of a tennis court). The structural matrix and the tissue
components of this alveolar-capillary network provide the only barrier between gas in the
airway and blood in the capillary. This barrier is 1 to 2 µm thick.
Surrounded mostly by air, this alveolar-capillary network creates an ideal environment for
gas exchange. Red blood cells pass through the capillary component of this network in single
file in less than 1 second, which is sufficient time for CO2 and O2 gas exchange.
In addition to gas exchange, the alveolar-capillary network regulates the amount of fluid
within the lung. At the pulmonary capillary level, the balance between hydrostatic and
osmotic pressure across the wall of the capillary results in a small net movement of fluid out
of the vessels into the interstitial space. The fluid is then removed from the lung interstitium
by the lymphatic system and enters the circulation via the vena cava in the area of the lung
hilus. In normal adults, an average of 30 mL of fluid per hour is returned to the circulation via
this route.
Starling's equation is used to calculate fluid movement across capillaries:
Flux (ml/min) = Kfc [(P(IV)-P(is)) – σd (πIV – πis)]
Kfc = capillary filtration coefficient of the total number of perfused capillaries
P(IV) = intravascular hydrostatic pressure
P(is) = interstitial hydrostatic pressure
σd = reflection coefficient (reflects the permeability of the membrane to protein)
πIV = intravascular colloid osmotic pressure
πis = interstitial colloid osmotic pressure
Starling's equation illustrates the forces that create the net flux of fluid out of the pulmonary
capillaries (See section 2).
3.7. Physical principles of gas exchange – diffusion of O2, CO2 through the respiratory
membrane
Air has about 0.04 % CO2, 20.9 % O2 and 79% N2. The remaining 0.06 % consists of other
gases. At sea level the total pressure of the mixture is 760 mmHg. Each gas contributes to the
total pressure in direct proportion to its concentration.
3-19
Therefore 79% of 760 mmHg is caused by N2 (600 mmHg) and 20.9 % by O2 (159 mmHg)
and 0.04 % CO2 (0.3 mmHg). The partial pressure of N2 (PN2) in the mixture is 600 mmHg
and the partial pressure of oxygen (PO2) is 159 mmHg. The total pressure is the sum of partial
pressures.
The pressure of a gas in a solution is determined by its concentration and by the coefficient of
solubility of the gas. If the gas molecules are attracted by water molecules then more of them
are dissolved without building up excess pressure within the solution. If the gas molecule is
repelled by water, excessive pressure will develop for many fewer dissolved molecules.
These relations can be expressed by Henry’s law:
Concentration of gas in solution = partial pressure of gas x solubility coefficient
e.g., [O2] moles/l : [O2] = PO2 x SO2
The solubility coefficients of important respiratory gases at 37 ºC are:
O2
0.024
CO2
0.57
CO
0.018
N2
0.012
He
0.008
S(CO2) is about 20 times higher than S(O2), that is CO2 is more than 20 times more soluble
than O2.
The partial pressure of each gas in the alveolar gas mixture tends to force molecules of that
gas into solution first in the alveolar membrane and then in the alveolar capillaries.
Opposite the molecules of the same gas that are already dissolved in the blood are moving
randomly in the fluid and some escape into the alveoli. The rate at which they escape is
directly proportional to its partial pressure in the blood.
In which direction will net diffusion of the gas occur?
The net diffusion is determined by the difference between the two partial pressures. If the
partial pressure is greater in the gas phase in the alveoli, as is normally true for O2, then more
molecules will go into the blood (liquid phase) than in other direction. Alternatively, if the
pressure of the gas is greater in the dissolved state in blood, which is normally true for CO2,
then net diffusion will occur towards the gas phase in the alveoli.
If the breathed air is non-humidified, in its way into the passageways, the water immediately
evaporates from the surfaces of the ducts and humidifies the air. This results from the fact
that water molecules are continuously escaping from the water surface into the gas phase (as
occurs with gases). The pressure that the water molecules exert to escape is called the vapour
3-20
pressure of the water. At normal body temperature this value is 47 mmHg and is designated
the partial pressure of water vapour P(H2O).
Calculating the P(O2) and P(CO2) in the air we breathe accounting for water vapour pressure
we will have:
Dry atm. air
Partial pressure
Accounting for
%
(mmHg)
P(H2O) = 47 mmHg
O2
21
160
149
N2
79
600
564
Total
100
760
713
In addition to the pressure difference several other facts affect the rate of diffusion of a gas in
a fluid:
1)
2)
3)
4)
5)
Solubility of the gas in the fluid
Cross-section area of the fluid
The distance through which the gas must diffuse
The molecular weight of the gas
The temperature of the fluid
In the body temperature remains relatively constant and usually need not to be considered.
All these factors can be expressed in a single formula:
D ∝ (ΔP x A x S) / (d x (MW)1/2)
eq. 3.5
Where D is the diffusion rate, ΔP is the pressure difference between the two ends of the
diffusion pathway, A is the cross sectional area of the pathway, S is the solubility of the gas,
d the distance of diffusion and MW the molecular weight of the gas.
The characteristics of the gas itself, S and MW, expressed by S/(MW)1/2 are proportional to
the diffusion coefficient of the gas.
If the diffusion coefficients of some gases (present in the lungs) are expressed in function of
O2 diffusion coefficient (=1), then CO2 = 20.3, CO =0.81, N2 =0.53 and He = 0.95.
The gases important for respiration are all highly soluble in lipids, therefore are highly
soluble in cell membranes.
Only 350 ml of new air is brought into alveoli at each inspiration. The FRC is about 2300 ml,
thus this value is about 1/7 of the total air remaining in the air at the end of normal expiration.
3-21
The removal of excess gas from the
alveoli can be represented graphically
(Figure on the left). It can be inferred
that for a normal rate of alveolar
ventilation, 50% of the gas is removed
in 17 seconds.
The importance of slow replacement of alveolar air is the prevention of sudden changes
in gas concentration in blood. This makes the respiratory mechanism stable as it prevents
excessive increases of tissue oxygenation, tissue CO2 concentration, tissue pH, when
respiration is temporarily interrupted.
PO2 and PCO2 in the alveoli
Oxygen is continuously being absorbed into the blood from the lungs and new O2 is
continuously being breathed into the alveoli from the atmosphere.
The more rapidly O2 is being absorbed the lower becomes its concentration in the alveoli.
The more rapidly O2 is breathed into the alveoli from the atmosphere the higher becomes its
concentration.
Therefore O2 and PO2 are controlled by the
1) rate of absorption into the blood and
2) the rate of entry of new O2 into the lungs by the ventilatory process.
Likely CO2 is continuously being formed in the body and then discharged into the alveoli. It
is also continuously being removed from the alveoli by ventilation.
3-22
!"#$%"&'()*+(,--./0(
The figures below show the alveolar ventilation and the rate of absorption into the blood on
the alveolar PO2 and excretion of PCO2. The figure also shows two rates of absorption and
excretion - solid and dashed curves.
At a normal ventilatory rate of 4200 ml/min
and an O2 consumption of 250 ml/min (solid
curve) the normal operating point of curve is
the point A corresponding to the normal PO2
in alveoli.
When 1000 ml O2 is being absorbed each
min (dashed curve) as occurs during
moderate exercise, the rate of alveolar
ventilation must increase 4x to maintain the
PO2 at normal value of 104 mmHg.
At normal rate of alveolar ventilation of
4200 ml/min and at 200 ml CO2 excretion
per min the normal operating point of the
curve – A, is 40 mmHg.
A higher rate of excretion of 800 mlCO2/min
is also represented (dashed curve).
It is clear that the rate of CO2 excretion is
proportional to the PCO2 increase, as
represented by the 4-fold elevation of the 800
ml/min curve.
It can be inferred from the graphic that even The alveolar PCO2 decreases in inverse
extreme increases in alveolar ventilation can proportion to the alveolar ventilation.
never increase the alveolar PO2 above 149
mmHg. The alveolar PO2 can approach this
value at high rates of ventilation.
Note: PO2 (humidified air) = 149 mmHg at sea level
Conclusion: The concentration and partial pressures of O2 and CO2 in the alveoli are
determined by the rates of absorption or excretion of the two gases and by the level of
alveolar ventilation.
Therefore increasing blood flow (perfusion) such as in exercise will increase movement of
O2 and CO2 into and out, respectively, of the system.
3-23