Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
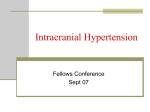
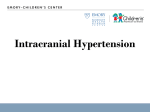
HIGHER SUBCORTICAL AND WHITE MATTER CEREBRAL BLOOD FLOW IN PERINATALLY HIV-INFECTED CHILDREN C. BLOKHUIS MD1, H.J.M.M. MUTSAERTS MD PhD2,3, S. COHEN MD PhD1, H.J. SCHERPBIER MD PhD1, M.W.A. CAAN PhD2, C.B.L.M. MAJOIE MD PhD2, T.W. KUIJPERS MD PhD1, P REISS MD PhD4,5,6, F.W.N.M. WIT MD PhD4,5,6, D. PAJKRT MD PhD1 KEY POINTS Perinatally HIV-infected children in our cohort have slightly higher cerebral blood flow in subcortical and An association between lower gray matter flow Subcortical or white matter cerebral blood flow did not relate to cerebral injury or poorer cognitive and white matter lesions may indicate a vascular performance. contribution to pediatric HIV-related white matter injury. white matter brain regions. OBJECTIVE The pathogenesis of cerebral injury and cognitive deficits in perinatally HIV-infected children is poorly understood. Chronic pediatric HIV infection and several components of cART have been associated with vasculopathy, coagulopathy, metabolic comorbidities, and an increased risk of cerebrovascular events, all potentially influencing cerebral blood flow (CBF).1,2 This study aimed to evaluate CBF in pediatric HIV-infection, and its role in HIV-related cerebral injury and cognitive impairment. METHODS This cross-sectional observational study included 28 perinatally HIV-infected children aged 8-18 years and 36 healthy controls matched for age, sex, ethnicity and socio-economic status (Table 1). Figure 1. Using arterial spin labeling to measure regional cerebral blood flow. All participants underwent 3-Tesla MRI, using arterial spin labeling to assess CBF in gray matter First row: obtaining ASL-measured CBF in gray matter (GM): (a) 3D T1-scan; (b) GM probability map; (c) GM mask, obtained by WM thresholding the probability map at p>0.8; (d) CBF map; (e) masked GM CBF map. The basal ganglia and thalamus regions, as defined using the Harvard Oxford atlas, are displayed in panel (b): caudate nucleus (orange), putamen (green), nucleus accumbens (blue), and thalamus (red). (GM), white matter (WM), basal ganglia, and thalamus (Figure 1). We used linear regression analysis to evaluate group differences and associations with HIV disease and treatment characteristics, macrostructural (volume loss, WM lesions) and microstructural injury (increased WM diffusivity, neurometabolite alterations), or poorer cognitive performance. RESULTS Cerebral blood flow in HIV-infected children and healthy controls HIV-infected children had higher CBF in WM (+10.2%; P=.042), caudate nucleus (+4.8%; P=.002), putamen (+3.6%; P =.017), nucleus accumbens (+3.9%; P=.031) and thalamus (+5.5%; P=.032) (Figure 2). Associations with HIV disease and treatment history Second row: the same process for white matter (WM) CBF: (f) 3D T1-scan; (g) WM probability map; (h) WM mask, obtained by thresholding the WM probability map at p>0.8 and eroding with a 7.5mm disk to avoid GM contamination; (i) CBF map; (j) masked WM CBF map. TABLE 1 STUDY PARTICIPANTS 34 healthy controls median age of 12.0 years 50% male 28 HIV-infected children median age of 13.5 years 54% male 29% CDC-C diagnosis nadir CD4+ T-cell count Z-score -0.7 Thalamus CBF was highest in children with a CDC stage B (coef=6.45; P=.005) or C (coef=8.52; P=.001) diagnosis. Longer duration of viral suppression was associated with lower caudate nucleus CBF (coef=-0.510; P=.009). Higher peak HIV VL was associated with higher GM CBF (coef=7.61; P=.025) and lower caudate nucleus CBF (coef=-2.66; P=.041). Longer immune suppression (CD4+ T-cell count <500*106/L) was associated with lower nucleus accumbens CBF (coef=-10.06; P=.027). 89% on cART since median age 1.6 years 89% virologically surpressed CD4+ T-cell count Z-score 0.8 Associations with cerebral injury and cognitive performance Lower GM CBF was associated with higher WM lesion volume in HIV-infected children ((coef=0.05; P=.039). No further associations with HIV-related cognitive impairment or cerebral injury were found. CONCLUSIONS CBF was higher in WM, basal ganglia and thalamus in cART-treated perinatally HIV-infected children, but this was not associated with cerebral injury or cognitive impairment. HIV-infected children with lower GM CBF had a higher volume of WM lesions, which could reflect vascular disease as potential contributing factor to white matter injury. Lifelong exposure to HIV and cART in this population warrants longitudinal assessment of CBF and how it relates to (neuro)inflammation, vascular dysfunction, and cerebral injury in pediatric HIV. Figure 2. HIV-infected children have higher cerebral blood flow in white matter, basal ganglia and thalamus. We compared arterial spin labeling (ASL)-measured cerebral blood flow (CBF) between HIV-infected children and healthy controls using linear regression analysis adjusted for age (years above 16 years), sex and hematocrit. Prior to analysis, CBF values for caudate nucleus, putamen, nucleus accumbens, and thalamus were normalized subject-wise using the overall mean gray matter CBF. The error bars represent standard deviations. REFERENCES: 1 Hammond et al, Dev Med Child Neurol 2016;58(5):452-460. 2Barlow-Mosha et al, J Int AIDS Soc 2013;16(1):18600. AUTHOR AFFILIATIONS: 1Department of Pediatric Hematology, Immunology and Infectious Diseases, Emma Children’s Hospital, Amsterdam 2Department of Radiology, Academic Medical Center, Amsterdam 3Cognitive Neurology Research Unit, Sunnybrook Health Sciences Centre, Toronto, Canada 4Department of Global Health, Academic Medical Center/Amsterdam Institute for Global Health and Development, Amsterdam 5Department of Internal Medicine, Division of Infectious Diseases, Center for Infection and Immunity Amsterdam (CINIMA), Academic Medical Center, Amsterdam 6HIV Monitoring Foundation, Amsterdam Corresponding author: Charlotte Blokhuis ([email protected]) Pediatric Infectious Diseases, Emma Children’s Hospital, Amsterdam