Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Marburg virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Hepatitis C wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Herpes simplex wikipedia , lookup
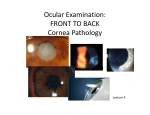
Cornea in Disguise: Atypical Presentation of Recurrent Corneal Erosion Katherine B. Lynch, OD VA Connecticut, 950 Campbell Ave, West Haven, CT Kimberly R. Rosati, OD VA Connecticut, 950 Campbell Ave, West Haven, CT Nancy Shenouda-Awad, OD, FAAO VA Connecticut, 950 Campbell Ave, West Haven, CT Charles Haskes, OD, MS, FAAO VA Connecticut, 950 Campbell Ave, West Haven, CT Abstract Recurrent Corneal Erosion (RCE) can be complicated by unexpected manifestations similar to that of an infectious or inflammatory etiology, making its initial diagnosis challenging. This poster highlights an atypical case of RCE and its management. I. Case History 61 year old white male Chief complaint: o Presented as an emergency o Red eyes with irritation OD>OS for two weeks o Associated clear discharge, foreign body sensation, light sensitivity, sensitivity to the touch and stabbing pain when eyes are initially opened, especially in the morning o Decreased acuity both eyes o Felt as if symptoms were worsening but denied precipitating event Ocular History o Entropion surgery OS o Resolved abrasion OS of unknown cause, treated on the outside o Corneal Ulcer OS of unknown cause, treated on the outside Medical History o Chronic Bronchitis o Essential hypertension o Hyperlipidemia o Sleep apnea o Schizoaffective disorder o Morbid obesity Medications o Albuterol o o o o o o o o Aripiprazole Budesonide Hydrochlorothiazide Lisinopril Lorazepam Simvastatin Tiotropium 18MCG Aspirin II. Pertinent Findings Clinical o Best corrected distance acuity: 1. 20/100 PH NI OD 2. 20/50-2 PH 20/40- OS o Hypersensitivity of Cornea OD o Slit Lamp Exam 1. 2+ Edematous lid without erythema OD 2. Meibomian Gland Dysfunction OU 3. 4+ injection OD, mild diffuse injection OS 4. Cornea a. OD: White blood cell infiltration inferiorly in a dense band with intact epithelium immediately above infiltration and patches of white blood cell infiltration superiorly also with an intact overlying epithelium, folds in descemet’s membrane, central and inferior geographic sloughing of the epithelium, and stromal edema. Map dystrophy apparent in the intact epithelium. b. OS: Map dystrophy with central whorl pattern of the epithelium, and pigmented guttatae 5. Anterior Chamber OD: 1+ Cell and flare, OS: trace cell and flare Laboratory studies o Viral swab cultures of the conjunctiva 1. Cytomegalovirus not detected 2. Herpes Simplex Virus not detected 3. Varicella-Zoster Virus not 4. No other viruses were detected o Bacterial swab cultures of the conjunctiva 1. Gram stain a. <1+ WBCs b. <1+gram positive rods/organisms 2. 2+ Corynbacterium SP a. No further workup of susceptibility was needed Imaging o Anterior Segment photographs were taken to monitor for changes III. Differential Diagnoses Primary: o RCE due to Map Dystrophy and complicated by Floppy Eyelid Syndrome Others: o Epidemic Keratoconjunctivitis (EKC) o Herpes Simplex Virus (HSV) with Neurotrophic Ulcer o Fuch’s Endothelial Dystrophy o Bacterial Keratitis due to infiltrate and anterior chamber reaction IV. Diagnosis and discussion EKC was an unlikely diagnosis due to the significant epithelial loss OD, the absence of a follicular reaction, and lack of immediate history of illness. HSV with Neurotrophic Ulcer was ruled out due to the appearance of an epithelial defect not consistent with a neurotrophic cornea, corneal hypersensitivity, and corneal infiltration. Fuch’s Endothelial Dystrophy was ruled out due to mild guttatae noted OS only with focal versus diffuse edema. Bacterial Keratitis was ruled out due to the lack of epithelial defects overlying the infiltrates, and lack of mucopurulent discharge. o The positive bacterial cultures with Corynbacterium were of the conjunctiva and were deemed to be due to meibomian gland dysfunction not the cause of the corneal presentation. RCE with Map Dystrophy was the final diagnosis especially due to worsening symptoms with mechanical lid opening in the morning. o The history of corneal maps OU, the past unexplained corneal abrasion, and the significant epithelial defect noted, all suggested RCE. Floppy eyelid syndrome was also a factor considered due to the asymmetry in presentation between the eyes and the fact the patient sleeps mostly on his right side, which may have worsened the exposure of the cornea OD. o In addition, the patient has sleep apnea and is obese. V. Treatment and Management Based on the above reasons, the patient was initially started on: o Vigamox, every hour with loading dose for first 4 hours, both eyes o Polysporin, twice per day both eyes o Homatropine, night time only both eyes o Non-preserved artificial tears, four times per day both eyes Treatment with topical antibiotics in this case was also used to treat and prevent any bacterial infection that may be associated with the chronic lid disease and meibomian gland dysfunction. He was later started on oral Doxycycline for more extensive treatment. The patient was presented to a cornea specialist and we followed him multiple times weekly to monitor improvement. Clinical findings showed improved acuity, improved symptoms and a healed epithelial defect. Once the corneal epithelium was intact, Pred Forte twice per day was added OU to reduce the anterior chamber inflammation. Within two weeks, the epithelial defect and stromal edema had resolved and the vision had significantly improved to: o 20/25-2 OD, 20/30-2 OS The patient continues to be followed for resolution of condition. He is expected to be on chronic hypertonic treatment and lid disease management. VI. Conclusion RCE is an easily overlooked diagnosis when associated with other unexpected factors, such as a significant and/or bilateral epithelial loss, infiltration, and anterior chamber reaction. With that said, atypical or more severe cases of RCE can be easily mistaken for a more aggressive pathology. It is essential to carefully examine the cornea of both eyes and the intact epithelium of the involved eye, especially in cases of asymmetric presentation, for other factors such as dystrophies that may put the patient at higher risk of developing corneal edema and RCE. With careful monitoring, topical antibiotics to prevent secondary infection and aggressive lubrication to heal the epithelium, patients can expect a favorable outcome and full recovery. Chronic treatment after resolution is critical.