Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Behçet's disease wikipedia , lookup
Signs and symptoms of Graves' disease wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
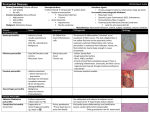
JACC Vol. 22, No . 6 November 05, 1993- 1 66 1 -5 1661 PERICARLUIS Purulent Perl'=~_l ~ IN: Review of a General Flosph'' Y Experience *111 ia JAUME SAGRISTA-SAULEDA, MD, JOSE A . BARRABIftS, MD, GAIETA PERMANYER-MIRALDA, MD, JORDI SOLER-SOLER, MD, FACC Barcelona, Spain Objectives . The purpose of this study was to review the features of purulent pericarditis in patients from a general hospital during a recent 20-year period. fiaekgmund. Although studies published from 1974 to 1977 suggested a changing spectrum for purulent pericarditis, this view has not been proved . Methods. We retrospectively evaluated the records of 33 patients from one general hospital who had a diagnosis of purulent pericarditis during the period 1972 to 1993 . All autopsy protocols from the sate period were also reviewed . In 19 patients (group 1), the condition was diagnosed during life; in 14 (group 11), it was identified at autopsy . Results . In group I, the possible sources of pericardial infection were identified in 17 patients ; pneumonia (6 patients) was the most common source . Empyema was present in 10 patients; 15 had cardiac tomponade . The most common microorganisms were streptococci, pneumococci and staphyloc&-cl . Six patients developed constrictive perkitis and rep' peri,ardiectonly. TOM patients died, 1 patient was lost to follow up and 15 patients hw a favorable outcome at a mean follow-up interval of 35 months . In group 11, the clinical diagnoses included pneumonia (five patients) among other infections, with enipyema in six patients . Purulent pericarditis was probably the direct cause of death in two patients. Conclusions . In our experience, the spectrum of purulent pericarditis has not changed in recent years . Many patients do not have the classical findings of pericarditis, and diagnosis is made only at autopsy or after tamponade has developed. Empyema remains a common predisposing condition . Purulent perie2rditis is still a severe disease, but its prognosis is excellent in patients who can be discharged from the hospital . Although purulent pericarditis has been known for many years (1), its features have been reported to have changed over the past decades (2-5) . Despite medical progress, this disease still carries a high mortality rate (2-4,6,7) . The diagnosis is missed in a high proportion of patients and is often identified only at autopsy . Because no major review of purulent pericarditis has been published in the past 15 years, the present report was based on a review of experience with the disease in patients admitted to the Hospital General Universitari Vail d'Hebron over the past 2 decades (1972 to 1991) . patients fulfilling the following criteria were included in the study : 1) purulent or cloudy pericardial exudate with a predominance of polymorphonuclear neutrophils ; or 2) growth of bacteriri ;-, the culture of pericardial fluid . In addition, one patient with extensive polymorphonuclear infiltrate in pericardial tissue and acute constrictive pericarditis in the context of an intrathoracic infection was included . Pericardial exudate was investigated in the microbiology laboratory. Smears for microscopic examination (Gram stain) were prepared as were cultures for aerobic and anaerobic organisms . Patients were assigned to two groups . Group I included those whose diagnosis of purulent pericarditis was made during life . Group 11 comprised patients whose disease was first identified at autopsy . Methods Patients. The clinical records were reviewed of all patients who had a clinical diagnosis of purulent pericarditis in the Hospital General Universitari Vail d'Hebron between January 1972 and December 1991 . The protocols of all autopsies performed during that period were also reviewed. All From the Servei de Cardiologia, Hospital General Universitari Vail d'Hebron, Barcelona, Spain . Manuscript received December 31, 1992 ; revised manuscript received May 26, 1993, accepted June 2, 1993 . Address for correspondence : Dr. Jaume Sagrista-Sauleda, Servei de Cardiologia, Hospital General Universitari Vail d'Hebron, Pg . Vail d'Hebron, s/n, 08035 Barcelona, Spain . ©1993 by the American College of Cardiology (J Am Coll Cardiol 1993,22:1661-5) Results During the 20-year period, 33 patients with purulent pericarditis were identified in a hospital population of 593,601 patients . The diagnosis was made during life in 19 of the 33 patients and at autopsy in the remaining 14 . No patient had features of acquired immunodeficiency syndrome (AIDS) . Group I . Group I comprised 19 patients (12 male, 7 female patients) aged 7 to 72 years . Only nine were admitted to the cardiology service . Five patients had an underlying 07311097/913100 1662 JACC Vol . 92, No . 6 November 15 .1993 : 1 66 1 -5 PURULENT PEICARDITIS L Table 1 . Possible Source of Infection and Clinical Background in the 19 Group I Patients Patients (no.) Pneumonia* Periodontal infection, floor of mouth abscess, mediastinitis Peritonsillar abscess, cervical abscess, mediastinitis Sepsis (originating from skin, oral cavity, parenteral nutrition, colon cancer) Peritonitis of bile origin Subphrenic abscess after traumatic rupture of the colon Possible urinary tract infection Unknown 6 (4 with empyema) 3 (2 with empyema) I (with empyema) 4 (3 with empyema) I I I 2 * left lung was affected in two patients, the right lung in three and both lungs in one . Group I - patients whose diagnosis of purulent pericarditis was made during life . chronic debilitating disease (alcohol abuse, rheumatoid arthritis and ulcerative colitis) . The possible source of infection and clinical background in the patients in group I are reported in Table 1 . Empyema was found in the vast majority . Clinical features of pericarditis developed between 2 and 30 days (mean 10) after onset of the infectious disease . The symptoms and signs in the 19 patients are shown in Table 2 . All patients had leukocytosis . The electrocardiogram (ECG) showed diffuse ST segment elevation in 10 patients ; 3 had diffusely negative T waves ; 7 had a low QRS complex amplitude . 4 had paroxysmal atrial fibrillation and 2 had normal ECG findings . No patient had electrical alternans . In all patients the cardiac silhouette on the chest radiograph was mildly or moderately enlarged . In addition, 6 patients had pneumonia and 12 had pleural effusion, An echocardiogram, recorded in 13 patients, showed moderate to severe pericardial effusion in 12 . The patient without effusion had constrictive pericarditis that had developed suddenly during a pyopneumothorax of 19 days' duration . The six patients without an echocardiogram had clinical evidence of cardiac tamponade. The diagnosis was confirmed through the removal of Tie 2 . Clinical Manifestations of Pericarditis in the 19 Group I Patients Patients No . Fever 19 Peticardial chest pain 7 Dy17 PeticarM friction rub 7 Ptrkardial effusion 18* t 15 o 12(: 100 37 89 37 94 79 63 *One patient had already developed constriction when he was seen in our center. tClinicai diagnosis . tTen patients had empyema. Group I = patients whose diagnosis of purulent pericarditis was made during life . purulent pericardial effusion . The indications for this procedure were cardiac tamponade (15 patients) ; no tamponade but the presence of mediastinitis and empyema and echocardiographic evidence of pericardial effusion (2 patients) ; no tamponade but a recent urinary tract infection and pericardial effusion with marked toxicity and leukocytosis (I patient), and pyopneumothorax with subsequent acute constrictive pericarditis requiring pericardiectomy (I patient) . Pericardiocentesis was carried out in 14 patients . In all instances, purulent fluid (150 to 1,150 ml) was obtained . In 16 patients the pericardium was surgically drained (in 4 as a first therapeutic procedure and in 12 after pericardiocentesis had demonstrated purulent pericardial effusion [6 had again developed tamponadel) . Microbiology . Table 3 shows the results of the cultures . Culture of pericardial fluid yielded negative findings in 10 patients, but 6 had received antibiotic agents before the culture was obtained . Clinical outcome and complications . Six patients developed severe constrictive pericarditis during their initial hospital admission and required pericardiectomy . Five of the six recovered uneventfully, and one died of heart failure 7 days after operation . Three other patients developed features of cardiac constriction that disappeared spontaneously . In two of the three, constriction was mild (xY pattern in jugular venous pulse and early septal diastolic notch) . The third patient had severe constriction with overt venous congestion, but progressive clinical improvement occurred, with normalization of the echocardiogram and external pulse recordings after 4 months . Three patients died : one because of renal failure and two of causes primarily related to the pericardial disease . Sixteen patients (84%) were discharged from the hospital . One was lost to follow-up ; the remaining 15 patients were followed up for I to 156 months (mean 35) . None of the 15 developed constrictive pericarditis . Group II . Among 3,419 necropsy studies, purulent pericarditis was identified in 14 patients (9 men, 5 women, aged 43 to 80 years [mean 61]) . Nine patients had an underlying chronic disease (neoplasia, chronic renal failure, hepatic cirrhosis, alcohol abuse and liver transplantation) . Thirteen patients were admitted because of an acute infectious disease ; the remaining patient had a temporary pacemaker . The clinical diagnoses and microbiologic findings are enumerated in Table 4 . No patients in group II were admitted to the cardiology service . In only two patients was a clinical diagnosis of pericardial disease made, but tamponade was not present and pericardiocentesis was not performed . In two patients neck vein distension was noted before death, but pericardiocentesis was not carried out . In another patient, ST segment elevation had been present on the ECG . An echocardiogram had been recorded in only one patient in group II . Death occurred I to 25 days after the onset of the disease . At autopsy, purulent pericardial exudate, 50 to 200 ml, was JACC Vol. 22, No . 6 SAGRIS PURE" November 15,1993 :1661-5 'LEDA ET AL . ARDITts Table 3 . Results of Microbiologic Studies in the 19 Patients With Purulent Pericarditis in Group I Pt No. I ro Origin of Fericarditis 3 Unknown Pneumonia Pneumonia 4 5 6 1 Urinary tract Pneumonia Unknown Periodontal 8 9 10 11 12 Pneumonia Skin sepsis Peritonitis Pneumonia Periodontal 13 14 15 16 17 18 19 Pericardial Fluid Negative Negative Peptococctes sp., G- anaerobes Negative Negative Negative Negative Pleural Fluid Cervical Exudate Blood Culture Negative Negative Proteus mirabilis Protests sp . Streptococcus viridans. Fusobacterium sp„ Peprococcus sp . Streptococcus pneramoniae Staphylococcus aureu., PN sepsis Periodontal Petitonsillar abscess Negative Negative Sr eptococcus miller! S . pneumonic Streptococcus anitis, llacteroides sp ., G -- anncrobes S . aureus Negative Negative Oral sepsis Pneumonia Colon cancer Subphrenic abscess ® S. pneumoaiae Clostridium septictan P . aeruginosa S . attilleri Negative S . ntitis, llacteroldes sp ., U- anaerobes lfaenaopltilus influenzcae S . aureas Bacteroides sp ., ti- anaerobes Enterococcaas faecahs S . vindwts, Streptococcus sp . Pseudoanoaws aeruginosa, Enterobacter cloacae H . influenzae S . milleri G- = gram-negative ; Group I = patients whose diagnosis of purulent pericarditis was made during life ; PN = parenteral n, .trition ; Pt = patient . present in all cases . Pericarditis was considered the immediate cause of death in two patients ; the others probably died of underlying diseases because the amount of pericardial fluid found was considered insufficient to impair hemodynamic function . Discuss o The present series is the largest series of patit fits with purulent pericarditis to Rae ieput Icd front a single tertidr~ hospital during the past 15 years . Our experience indicates Table 4 . Clinical Diagnoses and Microbiologic Findings in the 14 Group 11 Patients Pt No . Clinical Diagnosis I 2 3 4 5 II Pneumonia, empyema Pneumonia, empyema Purulent cltolecystitis Pneumonia, empyema AMI, right ventricular perforation by temporary pacemaker, sepsis Meningitis, sepsis Mastoiditis, pleuritis Empyema Sepsis by catheter Floor of mouth abscess, mediastinitis, empyema Bile tract infection, sepsis 12 13 14 Urinary tract infection, sepsis Liver transplantation, sepsis Pneumonia 6 7 8 9 10 Pericardial Fluid Other Cultures* Escherichia coil Staphylococcus aureus Negative Negative Pseudomonas aeruginosa S . aureus, Streptococcus mills, P . aeruginosa Klebsiella sp ., Enteracoccus faccalis, Proteus sp . E . coli, Klebsiella sp . P. aeruginosa E . coli, anaerobes S. aureus Streptococcus sp . P . aeruginosa *Extrapericardial cultures : pleural fluid (Patients 4 and 10) ; mastoidal exudate (Patient 7) ; blood (Patient 9) ; urine (Patient 13) . AMI = acute myocardial infarction ; Group Ill = patients whose diagnosis of purulent pericarditis was made at autopsy ; Pt = patient . 1664 JACC Vol . 22. No. 6 November 15, 1933 ;1661-5 SAGRISTA-SAULEDA ET AL . PURULENT PERICARDITIS that the features of the disease have not substantially changed during that period . Purulent pericarditis is still a critical disease, potentially lethal and frequently marked by severe complications, either from the pericarditis itself or from the underlying disease . The diagnosis was missed in 14 of the 33 pai .icnts, a problem that has been documented in other series (3-5,8) . There are two basic reasons for this low index of suspicion . 1) Purulent pericarditis is usually not associated with the characteristic features of acute pericarditis (4,9,10) . Thus, only 37% of our group I patients reported characteristic chest pain, and a friction rub was heard in only 37% . In group II, characteristic chest pain was not recorded in any patient, and a rub was auscultated in only one, 2) Other clinical features, such as fever, dyspnea or tachycardia, may be attributed to the underlying infectious disease . A third contributing factor may be that patients with purulent pericarditis are rarely admitted to a cardiology service (11) but are admitted to other services where the index of suspicion is lower . Purulent pericarditis almost invariably develops in the context of a severe infectious disease . In the present series of 33 patients, the most common source of infection was pneumonia, followed by generalized sepsis from several sources and by mediastinitis due to downward propagation of a mouth abscess. In only three patients (all in group I) was a source of infection not identified on admission . Remarkably, empyema was still a commonly associated finding in our series (15 of 33 patients) . In contrast to other series (4), we did not find cases secondary to thoracic or cardiac surgery . Purulent pericarditis was not diagnosed in any of the 458 patients with AIDS admitted to our hospital during the review period . In addition to the clinical context of the infection, clinical data suggested either purulent pericarditis or the need to drain the pericardium in almost all group I patients . Most important, 15 (79%) of the 19 patients developed clinical cardiac tampo e. Purulent pericarditis was not clinically suspected in any of the 14 patients from group II, and only 2 had a diagnosis of pericardial disease . Remarkably, however, it is probable that only 2 of the 14 patients died of pericardial disease itself . It is therefore obvious that in most group I patients the diagnosis was made at a time when pericarditis had already resulted in severe hemodynamic compromise . However, it may be that in group II patients the diagnosis went unnoticed because there were few findings suggesting severe pericarditis in most . In any case, the present series confirms that the d' osis of purulent pericarditis is rarely made before hemodynamic compromise develops (4,9). A wide variety of bacterial organisms have been reported as causative agents (12,13) . Although some reports (5) suggest an inc incidence of gram-negative organisms, in the present series the most commonly isolated organisms were gram-positive cocci . and co . It should be emphasized that 9 of the 19 patients in group I developed constrictive pericarditis . Constriction developed suddenly, early in relation to the onset of pericardial disease . Seven patients had severe constriction, and six required emergency pericardiectomy . Evolution to acute cardiac constriction has been observed in some series (4) but not in others (5,9) . Three patients in our series developed cardiac constriction that later disappeared spontaneously . This type of evolution is similar to the transient cardiac constriction reported previously by our group (14) in patients with acute idiopathic pericarditis, but it has not been reported in purulent pericarditis . Death was the consequence of pericarditis in only 2 of 3 patients in group I and in 2 of 14 in group II . The other patients died of underlying disease . This fact illustrates that purulent pericarditis usually develops in the context of a severe infectious disease, which in many cases is a determinant of the poor prognosis . The patients who were discharged from the hospital had a good late outcome . Thus, the complications of acute pericarditis appeared early in the clinical course, but no sequelae or late constriction was obscrved in any patient dining a mean follow-up period of 35 months . Conclusions Purulent pericarditis is still a severe disease that is recognized in most patients only at necropsy or after severe hemodynamic compromise has developed . Empyema remains a common underlying condition and pncumococcus a not exceptional offender . In virtually all cases, purulent pericarditis develops in the context of intrathoracic or subphrenic infection or generalized sepsis . In these situations, any suspicion of pericardial effusion or hemodynamic compromise makes echocardiography mandatory . If the echocardiogram suggests moderate or severe effusion, appropriate measures for pericardial drainage should be undertaken. The possibility of constrictive pericarditis, usually acute, should be kept in mind for the surveillance of the patients. The severity of the disease depends both on the pericarditis itself and on the underlying infectious disease . However, the prognosis is .xcellent for patients who can be discharged from the hospital . References 1 . Galen C . De Anatomicus Administrationibus (Singer C, translator) . New York: Oxford University Press, 1956 :192 . 2. Boyle JD, Pearce ML, Guze LB . Purulent pericarditis : review of literature and report of eleven cases . Medicine 1961 ;40:119-44. 3 . Gould K, Barnett JA, Sanford JP . Purulent pericarditis in the antibiotic era . Arch Intern Med 1974;134:923-7 . 4. Rubin RH, Moellering RC Jr . Clinical, microbiologic and therapeutic aspects of purulent pericarditis . Am J Med 1975 ;59:68-78 . 5 . Klacsmann PG, Bulkley BH, Hutchins GM . The changed spectrum of purulent pericarditis. An 86 year autopsy experience in 200 patients . Am J Med 1977;63:666-73 . 6. Israel L, Cavaillds J, Kovrilsky E . Bernard E. Pdricardite suppurde a streptocoques gudrie aprds drainage chinirgical . Coeur Med Interne 1%3 ;4 :477-82. JACC Vol. 22, No . 6 November 15,1993 :1661-1 7. k1orand PEI, Tadei A, Baba Arneur A . Les p6denrdhes purulentes . Sea' Hop Paris 1966 ,.45 :821-37, 8 . Bark SL, Rice PA, Reynolds CA, Finland M . Pneumococcai pl;oicarditis : a persisting problem in contemporary diagnosis . Am J Med 19M70 : 247-51 . 9 . Majid AA, Omai A . Diagnosis and management of purulent pericarditis . Exp-n-icnce with pericardiectomy, J Thorac Cardiovasc Surg 1991 :102 : 413-7, 10 . KaulTman CA, Walanakunakorn C, Phair JP, Purulent pneumococcal pericarditis . A continuing problem in the antibiotic era. Am J Med 1973 ;54:743-50 . SAG myA-SAULEDA ET AL . 1665 PURULENT PERICARDIT IS IL Permanyer-Miralda G, Sagrist .1-Sauleda J, Solvc-SukT 3 . Primary acute pericardial disease : a prospective series of 231 consecutive patients . Am J Cardiol 190 ;5b :623-3012 . Lorell BIt, BraunwaW E . Pericardial disease . in : Braunwa?d E, editor heart Disease . A Textbook of Cardiovascular Medicine . Philadelphia : Saunders, 1992 ;1465-516. 13 . Hall IP . Purulent pericarditis . Postgrad Med J 1989 -,65 :444-8 . 14. SagFisW-Sauleda J, Frrmanyer-Nlirdida G, Candell-Riera J, Ao&A J . Soler-Soler J . Transient cardiac constriction : an unrecognized pattern of evolution in effusive acute idiophatic pericarditis . Am 3 Cardiol 1987 -,59 : 9646 .