Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
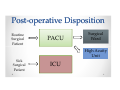
The Intensive PACU: Caring for Complex Patients Beyond the OR Kevin Froehlich MD FRCPC Anesthesiology, Vancouver Acute Clinical Assistant Professor UBC Faculty of Medicine Post--operative Disposition Post Routine Surgical Patient PACU Surgical Ward High Acuity Unit Sick Surgical Patient ICU Case #1 • 50 year-old male booked for an 8 hour anterior-posterior cervical spine decompression, instrumentation and fusion for cervical myelopathy. He has neurologic symptoms in his upper extremities and chronic neuropathic pain on multi-modal analgesic therapy including Oxycodone 50 mg three times a day. Case #2 • 75 year-old man booked for a radical cystectomy and ileal conduit for bladder cancer. He has a past medical history for morbid obesity (BMI 45), IHD with prior CABG, DM2 on insulin, renal impairment (Cr 160), and COPD. He was also diagnosed with severe OSA 1 year prior but is not compliant with CPAP therapy. What is the anticipated postpostoperative trajectory for these patients? Goals and Objectives • At the end of this lecture, I hope to establish: o Why we developed the IPACU at VGH o How we were able to start the IPACU o Which patients are suitable for the IPACU and when do we involve the ICU o Which department members work in the IPACU o What are the benefits and downsides to our IPACU model o How we hope to use our IPACU care model for development and training Case #3 • 65 year-old man undergoing left hepatectomy for HCC from hepatitis C. • PMHx: HTN, smoker and high cholesterol • Intraoperative- brisk 2L blood loss requiring 4 units RBC, noradrenaline infusion with transient ST depression when SBP 55 mmHg • Case is coming to an end, still on small amount of vasopressor, with ABG: 7.18/35/145/18, Hb 88 TUBE, PRESSORS, INTENSIVE CARE. OPTION: REACTIVE APPROACH Extubate in the OR… and hope for the best Treat hypotension with IV fluid Hold off on starting any analgesia Take to PACU, return to the OR, start the next case, manage care over the phone • If they fail- ICU has to take them! • • • • OPTION: PROACTIVE APPROACH • Take ventilated and sedated on vasopressor to PACU • Investigate: o o o o Serial ABGs for acid base status and ventilation titration Complete blood count for Hb, Plt, coagulation markers, renal function Troponin and ECG for markers of myocardial ischaemia Bedside Point of Care Ultrasound Assessment (POCUS) for: • Volume status • Basic cardiac function • Evidence of bleeding 1. We had the real estate…. 2. We had the nursing knowknow-how… 3. As a department we had the desire to do the work… 4. We had support from critical care colleagues… 5. We had a way to fund our work… “The Critical Care Payment Schedule is intended to be used by physicians providing direct bedside care to critically ill and unstable patients who are in need of intensive treatment, such as ventilatory support, haemodynamic support including vasoactive medications, or prolonged resuscitation.” What patients are appropriate for our IPACU and when should we involve our ICU colleagues? IPACU-- Definition IPACU • a specialized high acuity unit • goal of optimizing management of postoperative surgical patients prior to discharge to either a high dependency unit or a ward bed IPACU-- Patient Criteria IPACU • IPACU patients generally have no more than 2 systemic medical issues requiring management beyond the scope of routine PACU care • Expectation that all IPACU patients will be well enough for safe transfer out within 24 hours of admission When to consult ICU… One or more new organ dysfunction: • Hypoxemic respiratory failure with an Fi02 of >50% • New initiation of non-invasive ventilation for reasons other than OSA When to consult ICU… One or more new organ dysfunction: • Shock with persistent or increasing vasopressors requirements • Progressive acute renal failure with persistent oliguria • Severe delirium or agitation compromising medical management Typical IPACU Patients Patient Comorbidities Surgical Complexity • Severe cardiac disease • Severe respiratory disease • Major Pain Problem • Morbid obesity • Sleep disordered breathing • Thoracic- Pneumonectomy • Vascular- Open AAA • Urology- Radical Cystectomy • HPB- Liver Resection • Spine- Major Reconstruction • Surgical Oncology- HIPEC Do all members of department manage patients in the IPACU? Night Call Anaesthetist Day Call Anaesthetist 19:00 7:00 • Initially had 2 anaesthetists responsible for IPACU care • Care was suboptimal o o too many other responsibilities non-uniform level of interest • Perioperative Anaesthetist (POA) position created o o o Consistency Individuals with an interest in perioperative medicine Foundation to build on 7:00 Day Call Anaesthetist 7:00 Perioperative Anaesthetist 13:00 Night Call Anaesthetist 21:00 • POA shift is M-F, 13:00-21:00 • Clinical responsibilities fall outside the OR • Position provides consistency for nurses and department members, establish plans for all complex patients to guide overnight care 7:00 What are the benefits and downsides to the IPACU model? IPACU Care Model Benefits • Efficiency Off-load the ICU Short-term ventilation, vasopressor support • Analgesia We are the experts • Airway management Difficult extubations • Professional Development Training/teaching opportunities Downsides • Failure in IPACU- Transfer to ICU • Anaesthetist ≠ Intensivist Diagnosticians Routine ICU care • Nursing/resource Intensive • Non-uniform care Not all anaesthetists enjoy this work Multiple handover Case #1 • 50 year-old male, all day anteriorposterior cervical spine decompression, instrumentation and fusion. Chronic neuropathic pain on opioids… o 3L positive fluid balance o Opioid/ketamine infusion for whole case o Plan: • Emerge to evaluate neurologic status, then sedate • Ventilate overnight given airway oedema • Optimize analgesia • Controlled difficult extubation in 24 hours IPACU-- the place for ‘Difficult IPACU ‘Difficult Extubations’’ Extubations Case #2 • 75 year-old man booked for a radical cystectomy and ileal conduit for bladder cancer. • PMHx: o o o o o morbid obesity (BMI 45) IHD with prior CABG DM2 on insulin renal impairment (Cr 160) COPD o severe OSA but no CPAP OSA--the postOSA post-operative conundrum • Dr. Swart developed a PACU order-based OSA protocol to provide a practical approach to the post-op management of patients with OSA (diagnosed or suspected) Dr. Pieter Swart • Postoperative Risk Score = 6 • Provides objective numerical score to a challenging problem • PLAN = Overnight IPACU Case #3 • 65 year-old man undergoing left hepatectomy o 2L blood loss intra-op o Hemodynamic instability with transient ST depression o Metabolic acidosis • Proactive Care in IPACU planned o Take ventilated and sedated on vasopressor to IPACU • 2 hours after PACU admission: o o o o o Metabolic acidosis improved with correction of hypovolemia (serial POCUS exam) No evidence of on-going ischemia, first troponin negative, Hb stable Wean down noradrenaline and commence epidural analgesia Wean down sedation for PS ventilation with anticipated extubation in the coming hour Overnight in IPACU following extubation for on-going monitoring/care How we hope to use our IPACU care model for development and training… • Clinical Care o Post-operative OSA ward • Anaesthesia staff development o POCUS training • Workshops • Visiting Professors • Image acquisition • Image interpretation • Database • Anaesthesia training opportunities o o Perioperative Anaesthesia rotation for the residents Perioerative Anaesthesia fellowship Is the IPACU model a fit for your institution? PATIENT AND SURGICAL COMPLEXITY CRITICAL CARE RESOURCES CASC • Clinical Academic Services Contract- developed in 2000 • Agreement between VGH Department of Anaesthesia and the Vancouver Coastal Health Authority • Health authority collects: o Fee-for-service billings earned by the department o Fees earned from the University of British Columbia Faculty of Medicine for the provision of medical education • Health Authority pays a set fee for every daily anaesthesia position- we are accountable to provide the service