Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
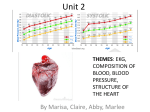
Influence of Inpatient Service Specialty on Care Processes and Outcomes for Patients With Non–ST-Segment Elevation Acute Coronary Syndromes Matthew T. Roe, MD, MHS; Anita Y. Chen, MS; Rajendra H. Mehta, MD; Yun Li, MS; Ralph G. Brindis, MD, MPH; Sidney C. Smith, Jr, MD; John S. Rumsfeld, MD, PhD; W. Brian Gibler, MD; E. Magnus Ohman, MD; Eric D. Peterson, MD, MPH Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Background—Since the broad dissemination of practice guidelines, the association of specialty care with the treatment of patients with acute coronary syndromes has not been studied. Methods and Results—We evaluated 55 994 patients with non–ST-segment elevation acute coronary syndromes (ischemic ST-segment changes and/or positive cardiac markers) included in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines) Quality Improvement Initiative from January 2001 through September 2003 at 301 tertiary US hospitals with full revascularization capabilities. We compared baseline characteristics, the use of American College of Cardiology/ American Heart Association guidelines class I recommendations, and in-hospital outcomes by the specialty of the primary in-patient service (cardiology versus noncardiology). A total of 35 374 patients (63.2%) were primarily cared for by a cardiology service, and these patients had lower-risk clinical characteristics, but they more commonly received acute (ⱕ24 hours) medications, invasive cardiac procedures, and discharge medications and lifestyle interventions. Acute care processes were improved when care was provided by a cardiology service regardless of the propensity to receive cardiology care. The adjusted risk of in-hospital mortality was lower with care provided by a cardiology service (adjusted odds ratio 0.80, 95% confidence interval 0.73 to 0.88), and adjustment for differences in the use of acute medications and invasive procedures partially attenuated this mortality difference (adjusted odds ratio 0.92, 95% confidence interval 0.83 to 1.02). Conclusions—Non–ST-segment elevation acute coronary syndrome patients primarily cared for by a cardiology inpatient service more commonly received evidence-based treatments and had a lower risk of mortality, but these patients had lower-risk clinical characteristics. Results from the present analysis highlight the difficulties with accurately determining how specialty care is associated with treatment patterns and clinical outcomes for patients with acute coronary syndromes. Novel methodologies for evaluating the influence of specialty care for these patients need to be developed and applied to future studies. (Circulation. 2007;116:1153-1161.) Key Words: coronary disease 䡲 patients 䡲 patient care 䡲 medical specialties 䡲 guidelines R andomized clinical trials have produced valuable insights into the treatment of patients with non–STsegment elevation (NSTE) acute coronary syndromes (ACS), insights that have been summarized into practice guidelines by the American College of Cardiology (ACC) and American Heart Association (AHA).1,2 Studies from the last decade demonstrated that patients with acute myocardial infarction (MI) cared for by a cardiology inpatient service were more likely to receive guidelines- Clinical Perspective p 1161 based treatment.3,4 Since these studies were performed, however, multiple parties, including the government, insurance companies, managed care organizations, academic organizations, and professional societies, have contributed to regional and national quality improvement programs designed to promote guidelines-based care for patients with ACS.5– 8 Whether these efforts have reduced or eliminated Received February 15, 2007; accepted June 15, 2007. From Duke University Medical Center and Duke Clinical Research Institute (M.T.R., A.Y.C., R.H.M., E.M.O., E.D.P.), Durham, NC; Department of Biostatistics, University of Michigan (Y.L.), Ann Arbor; Kaiser-Permanente Health System (R.G.B.), San Francisco Medical Center, San Francisco, Calif; University of North Carolina School of Medicine (S.C.S.), Chapel Hill, NC; Section of Cardiology (J.S.R.), Denver Veterans Affairs Medical Center/Division of Cardiology, University of Colorado Health Sciences Center, Denver, Colo; and the University of Cincinnati College of Medicine (W.B.G.), Cincinnati, Ohio. The online-only Data Supplement, consisting of 2 appendices, is available with this article at http://circ.ahajournals.org/cgi/content/full/ CIRCULATIONAHA.107.697003/DC1. Correspondence to Matthew T. Roe, MD, MHS, Duke Clinical Research Institute, 2400 Pratt St, Durham, NC 27705. E-mail [email protected]. © 2007 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.107.697003 1153 1154 Circulation September 4, 2007 differences in treatment patterns for ACS by physician specialty remains unknown. We sought to determine the contemporary relationship between the specialty of the inpatient service and processes of care and outcomes in patients with NSTE ACS included in the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) Quality Improvement Initiative. Our specific goals were to (1) describe differences in patient characteristics according to whether care was provided by a cardiology or a noncardiology service, (2) evaluate differences in guidelines-recommended treatments and clinical outcomes among patients cared for by a cardiology service versus those cared for by a noncardiology service, and (3) delineate how differences in processes of care by the specialty of the inpatient service are associated with clinical outcomes. Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Methods Patient Inclusion Criteria Patients included in the CRUSADE initiative presented with ischemic symptoms (ⱖ10 minutes) at rest within 24 hours of hospital presentation and had at least 1 of the following diagnostic features recommended by the ACC/AHA guidelines to distinguish patients with an increased risk of adverse outcomes: ST-segment depression ⱖ0.5 mm, transient ST-segment elevation 0.5 to 1.0 mm (which lasted for ⬍10 minutes), and/or positive cardiac markers (elevated troponin I or T and/or creatine kinase [CK]-MB greater than the upper limit of normal for the local laboratory assay used at each institution).1 Transfer-in patients were included if they were transferred in within 24 hours of the time of presentation to the outside hospital. Data Collection and Quality Hospitals participating in CRUSADE collect detailed process-ofcare and in-hospital outcomes data through retrospective chart review. Data are collected anonymously during the initial hospitalization, and because no patient identifiers are collected, patient informed consent is not required. The institutional review board of each institution approves participation in CRUSADE. Participating institutions are instructed to submit consecutive eligible patients to the CRUSADE database. Data are abstracted by a trained data collector using standardized definitions. Data collected include patient characteristics, the use of acute medications (within 24 hours of presentation), use and timing of invasive cardiac procedures, laboratory results, physician and hospital characteristics, and discharge therapies and interventions. Data collectors at participating sites were trained before commencing participation in CRUSADE with regard to the definitions of all variables and medication contraindications listed on the data collection form (see Appendices I and II in the online Data Supplement). For patients who were transferred into a CRUSADE hospital and who met the inclusion criteria, data collectors were instructed to utilize medical records from the outside hospital to account for data relating to the initial hospital presentation and for data concerning the administration of acute (ⱕ24 hours) medications before transfer in. The specialty of the primary inpatient service was defined by the sites on the basis of the admitting service and the specialty of the physician who had the most frequent and consistent notations in the medical record. Data collectors were instructed to choose 1 of the following 2 options for the specialty of the primary inpatient service: cardiology or the composite of family practice/internal medicine/ other. Data collectors were also instructed to record whether a formal cardiology consultation was performed (beyond the mere performance of a cardiac procedure) for patients primarily cared for by a noncardiology service. Various procedures have been established to maintain and monitor the quality of data submitted to the CRUSADE database. At data entry and during quarterly quality control analyses, values that exceed expected ranges are flagged and excluded from analyses. Additionally, sites receive a quarterly report summarizing data quality problems. Data quality was also verified with a random sampling of 5% of the patients included in CRUSADE (n⫽220) within the first 6 months of data collection. The overall accuracy of audited records was 94.8%. The overall degree of missing data averaged ⬇5% across all collected data elements, but variables such as age and gender were missing in ⬍0.5% of all audited cases. Chart Abstraction We performed a detailed abstraction of 85 patient charts that were randomly selected from a larger group of charts that were collected from sites participating in CRUSADE for an ongoing chart abstraction project. A single reviewer (MTR) independently reviewed each chart and confirmed that the specialty of the inpatient service denoted on the data collection form was accurate in all cases (100%). Data on the characteristics of the presenting symptoms, comorbidities, timing of the first documentation of a positive cardiac marker, and the primary clinical condition on presentation that were not collected on the data collection form were abstracted to provide a more in-depth characterization of patients primarily cared for by a cardiology versus a noncardiology service. Processes of Care We examined guidelines recommendations for acute care (ⱕ24 hours from admission) designated as class IA or class IB by the ACC/AHA guidelines, including the administration of aspirin or clopidogrel (if aspirin was contraindicated), -blockers, lowmolecular-weight or unfractionated heparin, and platelet glycoprotein IIb/IIIa inhibitors.1,2 We also evaluated the use and timing of cardiac catheterization and revascularization procedures given the class IA designation for early invasive management in the most recent version of the ACC/AHA guidelines.2 Class IA or IB recommendations for discharge care included aspirin; clopidogrel; -blockers; ACE inhibitors for patients with heart failure (ejection fraction ⬍40%), diabetes mellitus, or hypertension; and lipidlowering agents (for patients with hyperlipidemia or low-density lipoprotein cholesterol ⬎100 mg/dL).1 Contraindications were collected for each medication class and are listed in Appendix II. Analysis Cohort We chose to evaluate only those patients admitted to tertiary hospitals with full revascularization capabilities (percutaneous coronary intervention and coronary artery bypass grafting) because we could not collect patient information after interhospital transfer and to eliminate confounding related to the availability of invasive cardiac procedures. From January 2001 (beginning of data collection for CRUSADE) through September 2003, 57 800 NSTE ACS patients were included in the CRUSADE database from 301 hospitals with full revascularization capabilities in 45 states across the United States. We excluded 1334 patients (2.3%) who were transferred to other hospitals because complete in-hospital outcomes were not available and 472 patients (⬍1%) with missing data on the primary inpatient service, which left 55 994 patients in the final analysis population. The transfer-out rates were 2.9% for patients who received care from a noncardiology service and 2.0% for patients who received care from a cardiology service. Statistical Methods Patient demographics, clinical characteristics, care patterns, and in-hospital outcomes were compared among patients cared for by a cardiology service versus those cared for by a noncardiology service (internal medicine, family practice, or other). To test for independence of care by a cardiology service and patient characteristic, care patterns, and outcomes, Mantel-Haenszel 2 test was used with control for hospital site. Roe et al Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Because care provided by a cardiology service is not assigned randomly in clinical practice, we used 2 separate statistical methods to adjust for potential confounding in the treatment and outcome comparisons in the present study. In our primary analyses, we used a generalized estimating equation (GEE) method to adjust for patient and hospital characteristics, including patient age, female sex, body mass index, white race, insurance status, family history of premature coronary artery disease, hypertension, diabetes mellitus, current/ recent smoker, hypercholesterolemia, prior MI, prior percutaneous coronary intervention, prior coronary artery bypass grafting, prior heart failure, prior stroke, renal insufficiency, ST-segment depression, transient ST-segment elevation, positive cardiac markers, clinical signs of heart failure on presentation, presenting heart rate and systolic blood pressure, academic/teaching institution, total number of hospital beds, and geographic region within the United States.9 The GEE method was used because patients admitted in the same hospital tend to be more similar to each other than those in different hospitals (ie, within-hospital clustering of responses). Odds ratios and 95% confidence intervals were presented for care provided by a cardiology service to examine the variation of the strength of its influence on treatment patterns and clinical outcomes. In addition, we reported the standardized mortality rates to compare the absolute differences in mortality rates between patients cared for by a cardiology service and those cared for by a noncardiology service. From the mortality model that adjusted for patient and hospital characteristics, we obtained the probabilities of inhospital mortality. We then calculated a standardized mortality rate by dividing the sum of observed mortality (observed) by the sum of predicted probabilities of mortality (expected) among patients cared for by a cardiology service and those cared for by a noncardiology service and multiplied each observed-to-expected ratio by the mortality rate from the overall population. Our secondary analyses used propensity methodology to compare patient subgroups with similar likelihood for care by a cardiology service.10 Specifically, a multivariable model was developed to determine patient and hospital factors significantly associated with care by a cardiology service. We categorized patients into 5 equal groups that ranged from those with the lowest propensity for care by a cardiology service (group 1) to those with the greatest propensity for care by a cardiology service (group 5). We then explored acute (ⱕ24 hours) treatment patterns and use of catheterization ⱕ48 hours after presentation across the 5 propensity groups and displayed rates of unadjusted in-hospital mortality according to care by a cardiology service versus care by a noncardiology service within each of these 5 groups. Finally, to examine whether treatment-related differences accounted for differences in mortality according to whether or not care was provided by a cardiology service, we performed stepwise adjustment modeling with the following covariates: (1) patient characteristics, (2) patient and hospital characteristics, (3) patient and hospital characteristics plus use of acute (ⱕ24 hours) medications (aspirin, clopidogrel, -blocker, unfractionated/low-molecularweight heparin, and glycoprotein IIb/IIIa inhibitors) and individual contraindications for acute medications, and (4) patient and hospital characteristics, acute medications, medication contraindications, and catheterization ⱕ48 hours after presentation. A probability value ⬍0.05 was considered significant for all tests. All analyses were performed with SAS software (version 8.2, SAS Institute, Cary, NC). The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written. Results Specialty of Inpatient Service A total of 35 374 (63.1%) of 55 994 patients were primarily cared for by a cardiology inpatient service. During the study time period, the overall percentage of patients cared for by a cardiology service did not vary significantly by quarter and Physician Specialty and ACS Treatment 1155 Distribution of the percentage of patients primarily cared for by a noncardiology service across the participating hospitals. X-axis denotes the percentage of patients cared for by a noncardiology service in relation to the total number of patients submitted from each hospital, and y-axis denotes the percentage of hospitals for each category on the x-axis. was consistently between 61% and 65%. At the hospital level, the percentage of patients primarily cared for by a noncardiology inpatient service varied widely (Figure 1). A total of 12 685 patients (22.7%) were transferred in from an outside hospital. Patient Features by Primary Inpatient Service Patient and hospital characteristics according to the specialty of the primary inpatient service in the overall sample of 55 994 patients are shown in Table 1. Data from the chart abstraction project obtained from 85 patient charts demonstrate that the characteristics of the presenting symptoms and the timing of documentation of the first positive cardiac marker were similar regardless of the primary inpatient service (Table 2). Patients primarily cared for by a noncardiology service were more likely to have a documented “do-not-resuscitate” status. The primary clinical condition on hospital presentation was not related to ACS in ⬇15% of the patients regardless of the primary inpatient service. In the multivariable model generated from the overall sample of 55 994 patients, factors most strongly associated with care by a cardiology inpatient service included slower presenting heart rate, younger age, male sex, prior revascularization procedures, ischemic ST-segment changes, and lack of renal insufficiency, prior heart failure, diabetes mellitus, or prior stroke (Table 3). Medication and Procedural Utilization Patients cared for by a cardiology inpatient service were more likely to receive short-term (ⱕ24 hours) and discharge medications and to undergo invasive cardiac procedures (Table 4). Similar findings were demonstrated when the population was restricted to the 49 700 patients with NSTE MI (positive cardiac markers). Effect of Cardiology Consultation on Care Processes Among the 20 620 patients primarily cared for by a noncardiology service, 18 733 (90.9%) had a cardiology consulta- 1156 Circulation TABLE 1. September 4, 2007 Patient and Hospital Characteristics by Primary Inpatient Service Variable Overall (n⫽55 994) Cardiology (n⫽35 374) Noncardiology (n⫽20 620) 71 (59, 80) P Demographics Age, y* ⬍0.0001 67 (56, 78) 65 (55, 76) Female sex 39.1 35.7 45.1 ⬍0.0001 Black race 11.0 9.7 13.3 ⬍0.0001 HMO/private 46.6 47.9 44.4 Medicare/Medicaid 45.7 43.4 49.7 6.7 7.8 4.9 Family history of CAD 37.0 39.6 32.6 ⬍0.0001 Hypertension 68.9 67.2 72.0 ⬍0.0001 Diabetes mellitus 32.2 29.9 36.0 ⬍0.0001 Hyperlipidemia 48.5 50.7 44.7 ⬍0.0001 Current/recent smoking 28.3 31.0 23.8 ⬍0.0001 Renal insufficiency† 13.0 10.1 18.0 ⬍0.0001 Prior MI 30.6 31.0 29.9 0.0126 Prior CHF 17.2 13.6 13.4 ⬍0.0001 Prior PCI 22.7 25.3 18.2 ⬍0.0001 Prior CABG 20.7 21.6 19.2 ⬍0.0001 Prior stroke 10.3 8.5 13.4 ⬍0.0001 ⬍0.0001 Insurance status Self/none Medical history Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Presenting features Time from symptom onset to presentation, h* 2.8 (1.3, 7.2) 2.9 (1.3, 7.3) 2.8 (1.3, 7.0) 0.002 ST depression 39.8 40.8 38.1 ⬍0.0001 Transient ST elevation 10.0 11.3 7.9 ⬍0.0001 Positive cardiac markers 88.8 88.8 88.7 0.53 Signs of CHF 20.8 16.9 27.5 ⬍0.0001 81 (69, 97) 79 (68, 93) 86 (72, 101) ⬍0.0001 144 (124, 165) 143 (124, 164) 146 (124, 167) ⬍0.0001 Total hospital beds* 419 (297, 549) 420 (297, 552) 410 (296, 532) ⬍0.0001 Teaching hospital‡ 32.3 33.7 29.9 ⬍0.0001 Length of stay, d* 4 (3, 7) 4 (2, 6) 5 (3, 8) ⬍0.0001 Heart rate, bpm* Systolic BP, mm Hg* Hospital features Data are expressed as percentages except where indicated. HMO indicates health maintenance organization; CAD, coronary artery disease; CHF, congestive heart failure; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; and BP, blood pressure. *Expressed as median (25th, 75th percentile). †Creatinine ⬎2.0 mg/dL, calculated creatinine clearance ⬍30 mL/min, or need for chronic renal dialysis. ‡Member of the Council of Teaching Hospitals. tion performed during the hospitalization, 1430 (6.9%) did not have a consultation, and 457 (2.2%) had missing data on cardiology consultation. The short-term use (ⱕ24 hours) of aspirin (92.2% versus 82.4%), heparin (80.2% versus 52.7%), glycoprotein IIb/IIIa inhibitors (25.5% versus 3.7%), clopidogrel (34.7% versus 15.0%), and early catheterization ⱕ48 hours after presentation (37.4% versus 4.1%) was higher among those patients with than those without a consultation. In-Hospital Outcomes The frequency of adjusted in-hospital death, reinfarction, and transfusion was lower in patients who received care from a cardiology inpatient service (Table 5). Similar findings were demonstrated when the population was restricted to the 49 700 patients with NSTE MI (positive cardiac markers). The in-hospital mortality rate for the 472 patients who were excluded due to missing data on the specialty of the primary inpatient service was 8.7%. Propensity Analysis and Care Processes Among the 5 propensity groups, the average percentage of patients cared for by a cardiology inpatient service ranged from 47% in group 1% to 83% in group 5. Within each propensity group, patients cared for by a cardiology inpatient service were more likely to receive acute (ⱕ24 hours) medications and cardiac catheterization within 48 hours, but Roe et al TABLE 2. Physician Specialty and ACS Treatment 1157 Patient Characteristics From Chart Abstraction by Primary Inpatient Service Overall (n⫽85) Cardiology (n⫽46) Ischemic symptoms documented on ED arrival 82.2 76.1 87.2 0.56 Typical chest pain 82.6 82.6 82.1 0.99 Variable Noncardiology (n⫽39) P Symptoms Timing of first cardiac marker elevation 0.78 ⱕ12 h after arrival 87.1 89.1 84.6 䡠䡠䡠 ⬎12 h after arrival 5.9 4.4 7.7 䡠䡠䡠 No positive markers 7.0 6.5 7.7 䡠䡠䡠 Comorbidities Severe lung disease* 2.4 2.2 2.6 0.91 End-stage renal disease 3.5 2.2 5.1 0.46 Active malignancy 1.2 0 2.6 0.27 Severe cardiomyopathy† 2.4 4.4 0 0.19 Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Documented DNR status 4.7 0 10.3 0.03 ACS status: secondary ACS† 15.3 13.0 18.0 0.53 Data are expressed as percentages. ED indicates emergency department; DNR, do not resuscitate. *Chronic obstructive pulmonary disease or pulmonary hypertension requiring home oxygen use. †Dilated or ischemic cardiomyopathy (ejection fraction ⬍35%) with long-term treatment for heart failure. ‡Primary, presenting clinical condition not related to ACS. This includes patients who presented with an active infection or sepsis, heart failure exacerbation, or an acute neurological event. medication use decreased for both in-patient services as the propensity to receive cardiology care decreased (Table 6). Association of Care Processes With Mortality After adjustment for patient and hospital characteristics in the overall sample of 55 994 patients, the risk of mortality was significantly lower among patients cared for by a cardiology service (adjusted odds rato 0.80, 95% confidence interval 0.73 to 0.88; Table 4). After adjustment for differences in the use of acute (ⱕ 24 hours) medications, individual patient contraindications to acute medications, and the use of cardiac catheterization within 48 hours, the mortality difference was partially attenuated (adjusted odds ratio 0.92, 95% confidence interval 0.83 to 1.02). Discussion We have demonstrated that in contemporary practice, nearly 40% of patients with NSTE ACS were primarily cared for by a noncardiology service at tertiary hospitals with full revascularization capabilities. Patients cared for by a noncardiology service were older and had more comorbidities, were less likely to receive guidelines-recommended medications and invasive procedures, and had a higher risk of mortality. Explanations for Treatment Differences by Specialty Differences in treatment patterns by specialty demonstrated in the present analysis are likely related to multiple factors. First, patients who received care from a noncardiology service were older and had a greater burden of comorbid medical conditions than patients cared for by a cardiology service, so many of these patients may not have been ideal candidates for guidelines-recommended treatments and may have had undocumented medication contraindications that were not accounted for in the present analyses. Second, we demonstrated that the percentage of patients primarily cared for by a noncardiology service varied significantly across the participating hospitals, so hospitals likely did not have a standard approach for determining which patients were admitted to a noncardiology service. There may thus have been a selection bias for the disposition of “healthier” patients, who would be expected to be better candidates for evidencebased therapies, for care by an inpatient cardiology service. Finally, most (91%) of the patients in the present analysis who were treated by a noncardiology service received a cardiology consultation, but differences in treatment patterns were still demonstrated by specialty, which indicates that patient comorbidities and undocumented medication contraindications may have influenced treatment decisions to a greater degree than input from cardiologists.11 Therefore, evaluation of the association of specialty care with the disposition and treatment of NSTE ACS patients is very complicated. Methodology for Examining the Effect of Specialty Care on Outcomes Studies that have examined the influence of specialty care on the outcomes of patients with a variety of medical conditions have yielded conflicting results, most likely due to methodological shortcomings. In a recent meta-analysis of 49 studies, those studies that favored specialist care over generalist care frequently did not account for differences in case mix to adjust for selection biases, did not adjust for the effects of differences in practice environments, and did not consider case volume or physician experience to quantify the expertise of specialists.12 With regard to the influence of cardiology care on patients with ACS and acute MI, prior studies have shown that differences in case mix can bias treatment patterns 1158 Circulation September 4, 2007 TABLE 3. Patient and Hospital Factors Significantly Associated With Care Provided by a Cardiology Service 2 Adjusted OR 95% CI P Heart rate, per 10 bpm 191 0.93 0.92–0.94 ⬍0.0001 Renal insufficiency* 107 0.71 0.66–0.76 ⬍0.0001 Age, per 10 y 99 0.88 0.86–0.90 ⬍0.0001 Prior PCI 82 1.32 1.24–1.40 ⬍0.0001 ⬍0.0001 Variable Male sex 78 1.16 1.12–1.20 Signs of CHF 65 0.81 0.77–0.85 ⬍0.0001 Diabetes mellitus 51 0.87 0.84–0.91 ⬍0.0001 Prior stroke 49 0.80 0.75–0.85 ⬍0.0001 Transient ST elevation† 47 1.41 1.26–1.57 ⬍0.0001 ST depression† 1.16 1.10–1.22 Prior CABG 䡠䡠䡠 44 1.18 1.13–1.24 䡠䡠䡠 ⬍0.0001 Prior CHF 38 0.85 0.81–0.89 ⬍0.0001 Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Hyperlipidemia 36 1.14 1.09–1.19 ⬍0.0001 White race 36 1.23 1.14–1.33 ⬍0.0001 Positive cardiac markers 22 1.21 1.12–1.31 ⬍0.0001 Teaching hospital‡ 18 2.36 1.58–3.54 ⬍0.0001 Hypertension 9 0.95 0.91–0.98 0.003 Prior MI 7 1.06 1.02–1.10 0.008 Family history of CAD 5 1.05 1.01–1.10 0.02 Variables included in the model that were not significantly associated with cardiology care (P⬎0.05) included region, insurance status, body mass index, current/recent smoker, total number of hospital beds, and systolic blood pressure. OR indicates odds ratio; CI, confidence interval; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; CHF, congestive heart failure; and CAD, coronary artery disease. *Creatinine ⬎2.0 mg/dL, calculated creatinine clearance ⬍30 mL/min, or need for chronic renal dialysis. †Compared with neither transient ST elevation nor ST depression. ‡Member of the Council of Teaching Hospitals. and confound calculations for survival advantages for the type of patients cared for by cardiologists, because such patients usually have a lower burden of comorbidities.13,14 However, when measured and unmeasured confounding was accounted for with advanced statistical techniques, cardiology care was not associated with a mortality reduction for patients with acute MI but was associated with improved use of evidence-based therapies.15 Conversely, the present results and those from another study14 have shown that improved use of evidence-based therapies among ACS and acute MI patients partially explains differences in mortality by specialty. Furthermore, other studies have shown that higher composite quality scores for the treatment of patients with ACS and acute MI are associated with lower mortality rates, but the proportion of patients with acute MI considered to be ideal or eligible for guidelines-recommended therapies has decreased over the last decade with an aging population that has more comorbidities.16 –18 The challenge, therefore, is to develop research techniques that more accurately delineate how cardiology care and consultation between cardiologists and generalists influence the outcomes and treatment patterns of the increasingly complex population of patients with ACS and acute MI. Study Limitations Several limitations were present with this analysis. First, we did not collect detailed information regarding physician treatment decisions for individual patients, so we could not precisely determine how patient and hospital characteristics influenced care patterns and influenced the disposition of patients to cardiology and noncardiology services, even with a dedicated chart abstraction project within the context of this analysis. Second, documentation of medication contraindications may have varied by physician and hospital, which may have confounded our analyses of medication use in “ideal” candidates. Third, we did not collect contraindications to cardiac catheterization, because these are not well-specified in practice guidelines and often are dynamic as patients’ clinical characteristics change during the hospitalization. Fourth, we did not survey participating hospitals to determine whether differences existed in the quality improvement infrastructure or decision support systems for cardiology versus noncardiology inpatient services (such as use of critical treatment pathways, specialized nursing services, or electronic care prompts). Fifth, the mortality rate of the 472 patients excluded due to missing data on the specialty of the primary inpatient service was 2-fold higher than the overall Roe et al TABLE 4. Physician Specialty and ACS Treatment 1159 Treatment Patterns by Primary Inpatient Service* Overall (n⫽55 994) Cardiology (n⫽35 374) Noncardiology (n⫽20 620) Adjusted OR (95% CI)† Aspirin 91.8 (n⫽52 399) 93.0 (n⫽33 789) 89.7 (n⫽18 610) 1.28 (1.17–1.39) -Blocker 78.5 (n⫽51 128) 80.1 (n⫽32 713) 75.6 (n⫽18 415) 1.28 (1.20–1.36) Heparin 83.4 (n⫽53 159) 86.1 (n⫽34 224) 78.4 (n⫽18 935) 1.56 (1.43–1.70) Unfractionated 52.9 57.6 44.3 1.50 (1.42–1.60) Low–molecular weight 37.2 35.8 39.7 0.90 (0.84–0.95) GP IIb/IIIa inhibitor 37.7 (n⫽49 350) 45.0 (n⫽32 091) 24.1 (n⫽17 259) 2.11 (1.95–2.27) Clopidogrel 42.5 (n⫽55 428) 47.8 (n⫽35 187) 33.3 (n⫽20 241) 1.58 (1.49–1.69) Cardiac catheterization 72.7 81.4 57.8 2.55 (2.32–2.80) Catheterization ⱕ48 h 51.5 61.2 34.9 2.25 (2.08–2.43) PCI 41.7 49.2 28.9 1.86 (1.73–2.00) PCI ⱕ48 h 30.0 37.1 17.8 2.06 (1.91–2.23) CABG 13.3 14.0 12.1 1.13 (1.00–1.27) Acute (ⱕ24 h) medications Invasive procedures Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Discharge therapies and interventions Aspirin 90.8 (n⫽49 305) 92.5 (n⫽32 196) 87.5 (n⫽17 109) 1.37 (1.27–1.48) -Blocker 83.9 (n⫽48 195) 84.5 (n⫽31 198) 82.8 (n⫽16 997) 1.13 (1.06–1.21) ACE inhibitor‡ 60.7 (n⫽38 497) 61.0 (n⫽24 355) 60.1 (n⫽14 142) 1.06 (1.01–1.12) Lipid-lowering agent§ 80.7 (n⫽33 354) 82.1 (n⫽22 367) 77.9 (n⫽10 987) 1.12 (1.03–1.22) Clopidogrel 56.3 (n⫽51 966) 61.3 (n⫽33 446) 47.2 (n⫽18 520) 1.49 (1.40–1.59) Smoking cessation counseling储 66.0 (n⫽15 454) 67.9 (n⫽10 724) 61.8 (n⫽4730) 1.20 (1.08–1.33) Dietary recommendations 74.3 (n⫽53 695) 76.7 (n⫽34 249) 70.0 (n⫽19 446) 1.34 (1.24–1.45) Cardiac rehabilitation referral 43.5 (n⫽47 534) 48.0 (n⫽30 368) 35.7 (n⫽17 166) 1.39 (1.28–1.50) Nested percentages are not conditional, and percentages reported are in relation to the overall sample. GP indicates glycoprotein; PCI, percutaneous coronary intervention. *Among patients without documented contraindications. Data are expressed as percentages. Number of eligible patients for each medication or intervention is listed in parentheses. †Comparing cardiology with noncardiology care. ‡ACE inhibitor use reported only for patients with specific guidelines recommendations (ejection fraction ⬍40%, heart failure, diabetes mellitus, or hypertension). §Lipid-lowering agent use reported only for patients with documented hyperlipidemia and/or measured LDL ⬎100 mg/dL. 储Among current/recent smokers. have been long enough to fully evaluate the dissemination of these new recommendations to all specialties.2 Another general limitation of large observational databases such as CRUSADE is that data are frequently incomplete. When certain covariates are not captured on all individuals, it cannot be assumed that the pattern of missing data is completely at random. In fact, we usually make an assump- mortality rate of the analysis cohort, so exclusion of these patients may have biased the results. Sixth, only tertiary hospitals with full revascularization capabilities were included in the present analysis, so our results may not be generalizable to nontertiary hospitals. Also, the timeline of the present study spanned the release of the revisions to the NSTE ACS guidelines (March 2002), so our analysis may not TABLE 5. In-Hospital Outcomes by Primary Inpatient Service Death† Overall (n⫽55 994) Cardiology (n⫽35 374) Noncardiology (n⫽20 620) Adjusted OR* (95% CI) 4.1 3.2 5.7 0.80 (0.73–0.88) Reinfarction 3.0 2.8 3.4 0.74 (0.65–0.84) Congestive heart failure 8.7 7.1 11.5 0.96 (0.87–1.06) Cardiogenic shock 2.7 2.5 3.0 1.08 (0.95–1.23) Non-CABG RBC transfusion 8.8 7.0 11.8 0.75 (0.69–0.82) Data are expressed as percentages. RBC indicates red blood cell. *Comparing cardiology with noncardiology care. †Standardized mortality rates were 3.8% for cardiology vs 4.5% for noncardiology. Predicted mortality rates were 3.4% for cardiology vs 5.2% noncardiology. 1160 Circulation September 4, 2007 TABLE 6. Acute Treatment Patterns by Propensity for Care to Be Provided by a Cardiology Inpatient Service* Cardiology Care, Yes or No Group 1 (n⫽11 194) Group 2 (n⫽11 199) Group 3 (n⫽11 199) Group 4 (n⫽11 199) Group 5 (n⫽11 197) Yes (n⫽4907) No (n⫽6287) Yes (n⫽6491) No (n⫽4708) Yes (n⫽7343) No (n⫽3856) Yes (n⫽7993) No (n⫽3206) Yes (n⫽8639) No (n⫽2558) Aspirin 89.9 86.2 92.5 89.5 93.2 91.7 93.6 90.9 94.5 93.5 -Blocker 76.7 72.4 80.1 74.9 79.9 77.1 80.0 77.7 82.3 79.3 Heparin‡ 81.1 72.9 84.4 77.4 86.1 80.5 87.2 82.2 89.1 85.2 GP IIb/IIIa inhibitor 27.2 12.5 38.7 21.0 45.8 28.5 48.9 30.6 53.8 38.4 Clopidogrel 37.6 26.1 44.6 32.1 47.5 36.3 52.0 36.5 52.5 44.0 Catheterization ⱕ48 h 39.3 18.2 56.6 33.4 64.4 42.7 67.0 44.6 68.9 54.5 Treatments† All values are percentages. GP indicates glycoprotein. *Patients categorized based on the propensity to receive care from a cardiology service into 5 equal groups ranging from those least likely to receive care from a cardiology service (group 1) to those most likely to receive care from a cardiology service (group 5). †Medications administered ⱕ24 h to patients without contraindications. ‡Includes unfractionated and low–molecular weight heparin. Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 tion that a variable is “missing at random,” meaning that a variable’s absence is not a consequence of what would have been observed for that variable, but it may be related to other observed variables in the database. Although the GEE analysis we used has the capability of efficiently accounting for clustering in a very large database, it cannot be guaranteed to be unbiased. A weighted GEE analysis is sometimes recommended for data that have a missing-at-random pattern, but this modification is technically not feasible in such a large, complex database as CRUSADE with hundreds of possible missing value patterns and a mixture of binary and continuous variables. However, in addition to the GEE analysis presented in the present report, we performed a number of sensitivity analyses to provide assurance that our results were robust to the missing data. Conclusions We have demonstrated that patients with NSTE ACS primarily cared for by a cardiology service were younger and had fewer comorbidities than those primarily cared for by a noncardiology service, were more likely to receive evidencebased therapies, and had a lower risk of mortality. However, our findings from contemporary US practice highlight the difficulties of accurately determining the association of cardiology care with the treatment and outcomes of NSTE ACS patients and suggest that studies with real-time, prospective data collection are needed to further delineate the impact of specialty care. Sources of Funding CRUSADE is funded by Schering-Plough Corporation. BristolMyers Squibb/Sanofi Pharmaceuticals Partnership provides additional funding support. Millennium Pharmaceuticals, Inc, Cambridge, Mass, also provided funding for this research. Disclosures Drs Roe and Smith serve as speakers for Millennium Pharmaceuticals, Inc, Schering Corp, and Bristol-Myers Squibb/Sanofi-Aventis Pharmaceuticals Partnership. Drs Gibler, Ohman, Peterson, Roe, and Smith have received research grants from Millennium Pharmaceuticals, Inc, Schering Corp, and Bristol-Myers Squibb/Sanofi-Aventis Pharmaceuticals Partnership. The remaining authors report no conflicts. References 1. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE III, Steward DE, Theroux P, Gibbons RJ, Alpert JS, Eagle KA, Faxon DP, Fuster V, Gardner TJ, Gregoratos G, Russell RO, Smith SC Jr. ACC/AHA guidelines for the management of patients with unstable angina and non–ST-segment elevation myocardial infarction: executive summary and recommendations: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients With Unstable Angina). Circulation. 2000;102:1193–1209. 2. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE III, Steward DE, Theroux P, Gibbons RJ, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Smith SC Jr; American College of Cardiology/American Heart Association Committee on the Management of Patients With Unstable Angina. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: summary article: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol. 2002;40:1366 –1374. 3. Jollis JG, DeLong ER, Peterson ED, Muhlbaier LH, Fortin DF, Califf RM, Mark DB. Outcome of acute myocardial infarction according to the specialty of the admitting physician. N Engl J Med. 1996;335: 1880 –1887. 4. Ayanian JZ, Guadagnoli E, McNeil BJ, Cleary PD. Treatment and outcomes of acute myocardial infarction among patients of cardiologists and generalist physicians. Arch Intern Med. 1997;157:2570 –2576. 5. LaBresh KA, Ellrodt AG, Glicklich R, Liljestrand J, Peto R. Get with the guidelines for cardiovascular secondary prevention: pilot results. Arch Intern Med. 2004;164:203–209. 6. Mehta RH, Montoye CK, Gallogly M, Baker P, Blount A, Faul J, Roychoudhury C, Borzak S, Fox S, Franklin M, Freundl M, Kline-Rogers E, LaLonde T, Orza M, Parrish R, Satwicz M, Smith MJ, Sobotka P, Winston S, Riba AA, Eagle KA; GAP Steering Committee of the American College of Cardiology. Improving quality of care for acute myocardial infarction: the Guidelines Applied in Practice (GAP) initiative. JAMA. 2002;287:1269 –1276. 7. Zhang H, Alexander JA, Luttrell J, O’Connor GT, Daley J, Paris M. Data feedback and clinical process improvement in acute myocardial infarction. Am Heart J. 2005;149:856 – 861. 8. Roe MT, Ohman EM, Pollack CV Jr, Peterson ED, Brindis RG, Harrington RA, Christenson RH, Smith SC Jr, Califf RM, Gibler WB. Changing the model of care for patients with acute coronary syndromes. Am Heart J. 2003;146:605– 623. 9. Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13–22. Roe et al 10. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal events. Biometrika. 1983;70:41–55. 11. Willison DJ, Soumerai SB, McLaughlin TJ, Gurwitz JH, Gao X, Guadagnoli E, Pearson S, Hauptman P, McLaughlin B. Consultation between cardiologists and generalists in the management of acute myocardial infarction: implications for quality of care. Arch Intern Med. 1998;158: 1778 –1783. 12. Smetana SW, Landon BE, Bindman AB, Burstin H, Davis RB, Tija J, Rich EC. A comparison of outcomes resulting from generalist vs. specialist care for a single discrete medical condition: a systematic review and methodologic critique. Arch Intern Med. 2007;167:10 —-20. 13. Frances CD, Go AS, Dauterman KW, Deosaransingh K, Jung DL, Gettner S, Newman JM, Massie BM, Browner WS. Outcome following acute myocardial infarction: are differences among physician specialties the result of quality of care or case mix? Arch Intern Med. 1999;159: 1429 –1436. 14. Chen J, Radford MJ, Wang Y, Krumholz HM. Care and outcomes of elderly patients with acute myocardial infarction by physician specialty: Physician Specialty and ACS Treatment 15. 16. 17. 18. 1161 the effects of comorbidity and functional limitations. Am J Med. 2000; 108:460 – 469. Frances CD, Shlipak MG, Noguchi H, Heidenreich PA, McClellan M. Does physician specialty affect the survival of elderly patients with myocardial infarction? Health Serv Res. 2000;35:1093–1116. Peterson ED, Roe MT, Mulgund J, DeLong ER, Lytle BL, Brindis RG, Smith SC Jr, Pollack CV Jr, Newby LK, Harrington RA, Gibler WB, Ohman EM. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA. 2006; 295:1912–1920. Bradley EH, Herrin J, Elbel J, McNamara RL, Magid DL, Nallamothu BK, Wang Y, Normand SLT, Spertus JA, Krumholz HM. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006;296:72–78. Masoudi FA, Foody JM, Havranek EP, Wang Y, Radford MJ, Allman RM, Gold J, Wiblin RT, Krumholz HM. Trends in acute myocardial infarction in 4 U.S. states between 1992 and 2001: clinical characteristics, quality of care, and outcomes. Circulation. 2006;114:2806 –2814. CLINICAL PERSPECTIVE Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Previous studies have demonstrated differences in the treatment of patients with acute coronary syndromes by physician specialty, but the impact of cardiology specialty care on contemporary treatment patterns has not been studied. We evaluated 55 994 patients with non–ST-segment elevation acute coronary syndromes (ischemic ST-segment changes and/or positive cardiac markers) included in the CRUSADE Quality Improvement Initiative from January 2001 through September 2003 at 301 tertiary US hospitals with full revascularization capabilities. Approximately two thirds of patients were primarily cared for by a cardiology service, and these patients had lower-risk clinical characteristics and more commonly received guidelines-recommended acute (ⱕ24 hours) medications, invasive cardiac procedures, and discharge medications and lifestyle interventions than patients primarily cared for on a noncardiology service. Although the adjusted risk of in-hospital mortality was lower with care provided by a cardiology service, accounting for differences in the use of acute medications and invasive procedures partially attenuated this adjusted mortality difference. The present analysis highlights the difficulties in accurately determining how specialty care is associated with clinical outcomes for patients with acute coronary syndromes and suggests that novel methodologies for evaluating the influence of specialty care on the treatment and outcomes of acute coronary syndrome patients need to be developed. Influence of Inpatient Service Specialty on Care Processes and Outcomes for Patients With Non−ST-Segment Elevation Acute Coronary Syndromes Matthew T. Roe, Anita Y. Chen, Rajendra H. Mehta, Yun Li, Ralph G. Brindis, Sidney C. Smith, Jr, John S. Rumsfeld, W. Brian Gibler, E. Magnus Ohman and Eric D. Peterson Downloaded from http://circ.ahajournals.org/ by guest on August 10, 2017 Circulation. 2007;116:1153-1161; originally published online August 20, 2007; doi: 10.1161/CIRCULATIONAHA.107.697003 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2007 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/116/10/1153 Data Supplement (unedited) at: http://circ.ahajournals.org/content/suppl/2007/08/20/CIRCULATIONAHA.107.697003.DC1 http://circ.ahajournals.org/content/suppl/2007/08/20/CIRCULATIONAHA.107.697003.DC2 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/