Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
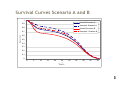
HTA OF TRASTUZUMAB IN ADJUVANT TREATMENT FOR HER2 POSITIVE BREAST CANCER Karianne Johansen, PhD, Senior Advisor, Torbjørn Wisløff , Researcher Inger Natvig Norderhaug , Research Director Norwegian Health Service Research Centre Expert Group Professor dr.med. Per Eystein Lønning, University of Bergen, Haukeland University hospital, Bergen Professor dr.med. Ivar Sønbø Kristiansen, HERO, University of Oslo Overlege dr.med. Bjørn Naume, The National hospital, Oslo Professor dr. med. Jan Norum, Cancer Unit, University hospital Northen Norway, Tromsø Professor dr.philos. Jan Abel Olsen, HERO, Universitetet i Tromsø Professor dr. med. Erik Wist, Cancer department, Ullevaal University Hospital, Oslo Background and Issues Promising interim data from large trials of Herceptin in treatment of HER2 positive adjuvant breast cancer published Q4 2005 /Q1 2006 Manufacturing authorization expected in Norway soon HER2 amplification recognized in 20-30% of breast cancers Associated with an aggressive form of the disease and shortened diseasefree survival and overall survival Pressure was put on an HTA of the new treatment prior to regulatory approval Part 1. A systematic review of the existing data to evaluate the effect and safety was performed Part 2. A cost-effectiveness model for Norway was developed Search for literature All relevant databases were searched according to a predefined protocol (Medline, Embase,the Cochrane Database of Systematic Reviews (CDSR), the Cochrane Controlled Trials Register (CCTR), the Science Citation index og the NHS Centre for Reviews and Dissemination databases (DARE, NHS EED, HTA)and OHE HEED) Web sites for conferences and international clinical trial databases Manufacturer's were asked to submit relevant documentation according to the protocol Results from the systematic review Search result 5 trials included - rated to medium quality Event driven interim analysis focusing on disease-free survival (DFS) Direction of effect Disease Free Survival A highly significant effect compared with the control group were found in all trials A meta-analysis of the hazard ratio for a risk of an event in the trastuzumab group compared with the control group were 0.5 (95% CI, 0.4 to 0.6) The absolute differences – 7.5 % to 8.4 % at 2 years – 11.0 % to 19.0 % at 4 years Overall Survival All reported results were in favor of trastuzumab Only one analysis (JOINT) of two trials showed statistical significant effect We concluded There is not enough data available to draw certain conclusions regarding overall survival due to short follow-up *HERA, NSABP B-31, NCCTG- N9831, BCIRG 006 , FinHER Results from the systematic review Direction of adverse events Trastuzumab was associated with increased risk of cardio toxicity, despite very strict cardiovascular exclusion criteria in the protocols NYHA Class III or IV congestive heart failure or death from cardiac causes – Trastuzumab group: 0.5 % to 4.1 % – Control group: 0.0 % to 1.0 % Decrease in LVEF – Trastuzumab group: – Control group: 7.1 % to 17.3 % 2.2 % to 9.0 % Discontinuations of trastuzumab : 8.5 % - 31.4 %. We concluded Long term follow-up of patients is needed, with a special focus on cardio toxicity Further need for evaluation – Issues ? A Hazard Ratio of 0.5 for a risk of a disease-free event in the trastuzumab group compared with the control group is a relative number How effective is today's adjuvant treatment of breast cancer in Norway? What is the incremental risk of death for HER2 positive patients? Treatment with trastuzumab is costly with potentially serious adverse event – whom are eligible for treatment? Is the incremental effect of trastuzumab reasonable relative to the incremental cost? How sustainable is the effect beyond the interim data? Patients eligible for treatment Mean age 50 years - less patients above 55 - none above 70 Incidence of Breast Cancer Age Eligible for adjuvant chemotherapy HER2 positive and eligible for trastuzumab 20 - 54 845 676 203 1078 344 103 771 0 0 2694 1021 306 55 - 69 70 + Total *Age 55-70 years, eligibility for adjuvant chemotherapy depend on hormone receptor status Not women who have an LVEF of 55% or less, or any of the following: • • • • • • a history of documented congestive heart failure high-risk uncontrolled arrhythmias angina pectoris requiring medication clinically significant valvular disease evidence of transmural infarction on electrocardiograph (ECG) poorly controlled hypertension. Health Economic evaluation Standard treatment: FEC100 + observation New treatment: FEC100 + 1 year trastuzumab every 3 weeks A markow model, one year cycles was constructed Inputs were based on The results from the clinical trials (Event rates and Hazard ratios) Data from the Norwegian Cancer Registry used for breast cancer survival Different assumptions were made together with the expert group to show different variations on extending the effect beyond the clinical trials Both cost and LYG were discounted at 3 % In the base case costs are presented from a health care perspective Average age in the model, 50 years, time horizon - life time perspective *FEC100 = 5-flurouracil, epirubicin-og cyklofosfamid (locoregional radiotheraoy and systemic hormonal therapy is used were appropriate) Model Structure 1. Disease free 2. Local recurrence 3. Distant recurrence 4. Death* *Dead from metastatic breast cancer or from non-cancer causes while in any of the first 3 disease states. Patient die from breast cancer only after distant recurrence Base case Scenarios A and B Scenario A Stadium I and II from the Cancer Registry as a total sum of survival Events – Years 0 - 4: – Years 5 – 10: – Years 11 + : Probability of death from breast cancer Comparator arm – Years 0 – 10: Survival taken from the Norwegian Cancer Registry – HER2 additional risk factor of 1.3 was applied for the first 10 years Trastuzumab – Years 0 to 4: – Years 5 – 10 : – Years 11 + : Results from clinical trials Results gradually decline =0 HR from the JOINT analysis used (0.67) The cancer registry with equal risk Patients alive follow normal survival in the population Probability of death from other causes than breast cancer – Survival rates from Norwegian Statistics Scenario B Stadium IV from the Cancer Registry used for risk of death from metastatic phase In all other stages risk of dying follow normal survival in the population) Survival Curves Scenario A and B 1 Kontroll Scenario A 0,9 Overlevelse Survival Herceptin Scenario A 0,8 Kontroll Scenario B 0,7 Herceptin Scenario B 0,6 0,5 0,4 0,3 0,2 0,1 0 0 5 10 15 20 25 År Years 30 35 40 45 50 Results (discounted 3%) Scenario A Strategy Cost (EUR) Trastuzumab 59 000 Standard 29 625 Incremental Cost (EUR) Effectiveness (LY) Incremental Effectiveness (LYG) ICER 18,7 29 375 17,2 1,5 19 580 EUR/LYG Scenario B Strategy Cost (EUR) Trastuzumab 54 875 Standard 21 500 Incremental Cost (EUR) Effectiveness (LY) Incremental Effectiveness (LYG) ICER 17,7 33 375 15,5 Cost-effectiveness in favor of trastzumab 2,2 15 170 EUR/LYG Results (undiscounted) Scenario A Strategy Cost (EUR) Trastuzumab 72 625 Standard 48 000 Incremental Cost (EUR) Effectiveness (LY) Incremental Cost-Effectiveness Ratio (ICER) Incremental Effectiveness (LYG) 30,2 24 625 27,5 2,7 9120 EUR/LYG Scenario B Strategy Cost (EUR) Trastuzumab 65 125 Standard 34 000 Incremental Cost (EUR) Effectiveness (LY) Incremental Effectiveness (LYG) Incremental Cost-Effectiveness Ratio (ICER) 28,5 31 125 24,5 Cost-effectiveness in favor of trastzumab 3,9 7980 NOK/LYG Conclusion ICER presented below most common thresholds Treatment with trastuzumab per patient is estimated at 40 600 EUR the first year in the model In a cohort of 300 females there will be 11 less local recurrence and 44 less metastatic events in the trastuzumab arm The largest uncertainty is the extrapolation of long term benefit from the interim results, with a short follow-up Careful follow-up of patients focusing on recurrence, survival and long term adverse events needed A special focus should be put on long term follow up of cardio toxicity.