Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
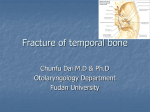
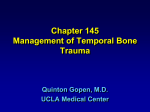
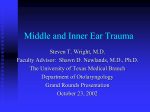
May 2010 A Shattered Face: Radiologic and Surgical Reconstruction of Complex Craniofacial Trauma Kapil Verma, Harvard Medical School Year IV Gillian Lieberman, MD Beth Israel Deaconess Medical Center Harvard Medical School Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Background: Epidemiology of craniofacial trauma • Approximately 50% of the 12 million annual traumatic wounds treated in emergency rooms across the United States involve the head and neck • Common causes of craniofacial trauma include: - Motor vehicle accidents (community setting) - Assault (urban setting) - Sports injuries and falls - Domestic violence • Among level-1 trauma centers, facial trauma is managed by: - Plastic surgeons (40%) - Oral and maxillofacial surgeons (36%) - Otolaryngologists/head and neck surgeons (23%) - General surgery and Oculoplastics (~0.5%) Singer, Hollander, Quinn Aksoy, Unlu, Sensoz Bagheri et al Holmes Background: Why recognition and management of craniofacial trauma is crucial • The face contains crucial specialized systems needed to see, hear, smell, breathe, eat, and speak • Vital structures within the head and neck are intimately associated • Several facial injuries may be life threatening: - Hemorrhage - Airway obstruction - Aspiration • The psychological impact of facial disfigurement can be devastating Manson et al Lee et al Background: Clinical exam findings in the recognition of craniofacial trauma • • • • • • • Facial asymmetry Pain upon palpation Facial instability Cortical step-offs Periorbital edema Periorbital crepitus Infraorbital numbness Epistaxis Epiphora Exopthalmus Enopthalmus Telecanthus Orbital muscle/nerve entrapment • Many more … • • • • • • Manson et al Background: Limitations of the clinical exam in the recognition of craniofacial trauma Clinical evaluation of the facial skeleton in trauma patients is difficult: - Facial features are often obscured and distorted by endotracheal and gastric tubes and tapes that hold them in place. Thus, evaluation of facial instability is difficult - Response to painful stimuli is blunted. Thus, evaluation of localized pain secondary to fractures is difficult Rehm, Rhos Background: The crucial role of radiologic imaging in the recognition of craniofacial trauma • Up to 60% of facial fractures may be missed clinically (lack of step-offs, instability, orbital entrapment, telecanthus, etc) and are later detected by CT • Of those 60% of clinically unsuspected facial fractures later detected on CT, approximately 50% require subsequent surgical repair • As a result, though plastic surgeons and maxillofacial surgeons primarily manage craniofacial trauma, the radiologist plays a crucial role in diagnosis to guide management Rehm, Rhos Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Normal craniofacial skeletal anatomy: The skull consists of cranial and facial bones http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Normal craniofacial skeletal anatomy: Components of both cranial and facial bones form the orbit - colloquially known as the ‘eye socket’ http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Normal craniofacial skeletal anatomy: Lateral view of the 22 bones of the skull, 8 cranial bones and 14 facial bones 8 cranial bones: 1 2 1 2 1 x x x x x Frontal Parietals Sphenoid Temporals Ethmoid 14 facial bones 2 2 1 2 2 2 2 1 x Occipital x x x x x x x Lacrimals Inferior Nasal Conchae Vomer Nasals Zygomatics Palatines Maxillae 1 x Mandible http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Normal craniofacial skeletal anatomy: Anterior view of the facial bones and orbit 7 orbital bones Frontal Sphenoid Ethmoid Palatine Lacrimal Zygomatic Maxillary Cranial Facial 14 facial bones 2 2 1 2 2 2 2 x x x x x x x Lacrimals Nasals Vomer Inferior Nasal Conchae Maxillae Palatines Zygomatics 1 x Mandible http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Normal craniofacial skeletal anatomy: Skeletal anatomy of the orbit 7 orbital bones Frontal Sphenoid Cranial Ethmoid Palatine Lacrimal Zygomatic Maxillary Facial http://www.ophthobook.com/wp-content/uploads/2007/12/an-orbitbone.jpg http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Normal craniofacial skeletal anatomy: Anatomy of the mandible Coronoid process Condylar process Ramus http://www.face-and-emotion.com/dataface/anatomy/facialbones.jsp Angle Body Symphysis http://www.arthursclipart.org/medical/skeletal/skull%20front%20side.gif Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Shattered Anatomy: Intro to Patient AA History • 37M unhelmeted bicycle rider struck by a car, propelled head first through windshield • Widely opened multiple cranial and facial fractures with visible brain material, otherwise (remarkably) no other no traumatic injury to the chest, abdomen, or pelvis • Intubation initially difficult secondary to multiple facial fractures • Unable to immediately assess for clinical signs of orbital entrapment secondary to patient’s waning mental status Shattered Anatomy: Intro to Patient AA Initial 3D Facial CT Reconstruction Anterior View NORMAL OUR PATIENT, AA Anterior 3D-reformatted CT reconstructions of the face Normal patient on the left. Our patient AA on the right GE Vitrea 3D Workstation, MGH Shattered Anatomy: Intro to Patient AA Initial 3D Facial CT Reconstruction Oblique view NORMAL OUR PATIENT, AA Oblique 3D-reformatted CT reconstructions of the face Normal patient on the left. Our patient AA on the right. GE Vitrea 3D Workstation, MGH Shattered Anatomy: Intro to Patient AA List of craniofacial injuries (to be revisited) OUR PATIENT, AA Severely comminuted, complex frontal bone fractures R. superior lateral orbital rim fracture L. lateral orbital wall fracture Bilateral orbital floor fractures Bilateral LeFort II fractures Anterior 3D-reformatted CT reconstruction of the face Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures GE Vitrea 3D Workstation, MGH Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Menu of radiologic tests: Traditional facial radiograph series- outdated in the evaluation of facial trauma • Traditional facial radiographic series include those such as the ‘Waters view,’ ‘Caldwell view,’ ‘Towne view’ and submentovertex view • Such views are outdated in evaluation of facial trauma: difficulty of interpretation amongst non-radiologist physicians inability to assess soft tissues in detail advent of CT and 3D CT reformatting http://www.ispub.com/journal/the_internet_journal_of_otorhi nolaryngology/volume_5_number_2_21/article/inter_observ er_and_intra_observer_variability_in_the_assessment_of_t he_paranasal_sinuses_radiographs.html Chen, Ng, Whaites Menu of radiologic tests: Facial Multidetector CT - the imaging gold standard • Facial Multidetector CT without contrast with axial and coronal sections is the gold standard in the evaluation of facial trauma – Fast – Bone windows may evaluate for fractures – Soft tissue windows may simultaneously evaluate for secondary soft tissue swelling (including extra-ocular muscles, nerves, and globe) and hematomas – Coronal sections are superior to radiographs in showing orbital floor fractures – Subsequent 3D CT reformatting is possible Tanrikulu, Erol Menu of radiologic tests: CT with 3D reformatting - Background • Contiguous 2D CT slices are obtained via normal CT protocol • These series of tomographs are analyzed by a 3D software program • The computer essentially uses one of two rendered techniques to obtain a 3D image: 1- Threshold/Surface Rendering 2- Volume Rendering Kung, Fung Menu of radiologic tests: CT with 3D reformatting – Surface rendering and volume rendering • Principle behind threshold/surface rendering is based on the Hounsfield scale (quantitative scale for radiodensity in CT using Hounsfield Units = HU) -1000 HU: Air -100Æ-30 HU: Fat 0 HU: Water +30Æ+100 HU: Soft tissue +1000 HU: Cortical Bone • Can select CT attenuation value of +150 HU as threshold, and thus all soft tissues (below +150 HU) excluded in final 3D CT image, and only bone (and other structures with HU > +150) included • Volume rendering performs a similar algorithm using summation Kung, Fung Menu of radiologic tests: CT with 3D reformatting - Conceptually simplified Combine with coronal sections Apply rendering algorithms using HU thresholds to subtract soft tissues Axial CT sections obtained from PACS BIDMC; stacked graphic created independently 3D CT Face reconstruction image obtained from GE Vitrea 3D Workstation, MGH Menu of radiologic tests: CT with 3D reformatting - useful for the surgeon • Surgeons generally ‘think in 3D’ vs. radiologists with specialized training in 3D interpretation of 2D imaging • 3D reformatting may aid in pre-surgical planning • 3D reformatting may aid in the design of custom facial prosthetics Reuben, Watt-Smith, Dobson, et al Alder, Deahl, Matteson Menu of radiologic tests: Panorex • 2D panoramic x-ray (radiograph) of the upper and lower teeth and mandible • Displays the mandible as a flat structure • Combined with CT, picks up virtually all fractures of the mandible • When used alone, often misses parasymphysial fractures of the mandible Romeo, Pinto, Cappabianca, et al Menu of radiologic tests: Panorex – may miss mandibular fractures if used alone -This patient was initially noted to only have 1 left nondisplaced fracture at the junction of the mandibular ramus and condylar process from this Panorex Panorex film of the mandible, upper and lower teeth AGFA, MGH Menu of radiologic tests: Panorex – may miss mandibular fractures if used alone -This patient was initially noted to only have 1 left nondisplaced fracture at the junction of the mandibular ramus and condylar process from this Panorex Panorex film of the mandible, upper and lower teeth AGFA, MGH Menu of radiologic tests: Panorex – should be used in conjunction with CT for the evaluation of mandibular fractures - On subsequent CT, however, in addition to known left mandibular fracture, she was found to have 2 additional mandibular fractures: a right condylar process fracture, and a parasymphysial fracture Coronal C- CT sections through mandible AGFA, MGH Menu of radiologic tests: Panorex – should be used in conjunction with CT for the evaluation of mandibular fractures - On re-evaluation of original Panorex, the 2 additional fractures seen on CT became apparent, though still difficult to assess on Panorex alone Panorex film of the mandible, upper and lower teeth AGFA, MGH The patient subsequently had arch bar placement and wire fixation of her maxillary and mandibular teeth Panorex film of the mandible, upper and lower teeth; post arch bar placement and wire fixation of upper and lower teeth AGFA, MGH Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Patient AA revisited: Frontal bone fractures OUR PATIENT, AA Severely comminuted, complex frontal bone fractures Anterior 3D-reformatted CT reconstruction of the face GE Vitrea 3D Workstation, MGH Patient AA revisited: Frontal bone fractures on CT Axial C- CT through the level of the frontal bone; bone window AGFA, MGH Patient AA revisited: Frontal bone fractures on CT, Findings Axial C- CT through the level of the frontal bone; bone window • Numerous severely comminuted fractures of the frontal bone • Low attenuation areas of subcutaneous emphysema • High attenuation foreign objects, likely leadcontaining glass fragments (as patient was projected head first through windshield) AGFA, MGH Patient AA revisited: Orbital rim, wall, and floor fractures OUR PATIENT, AA R. superior lateral orbital rim fracture L. lateral orbital wall fracture Bilateral orbital floor fractures Anterior 3D-reformatted CT reconstruction of the face GE Vitrea 3D Workstation, MGH Patient AA revisited: Orbital fractures on CT Coronal C- CT through the level of the orbits; bone window Sagittal C- CT through the level of left orbit; bone window AGFA, MGH Patient AA revisited Orbital fractures on CT, Findings • Non-orbital fracture seen: Depressed skull fragment of frontal bone (on soft tissue window seen to cause cerebral edema, necessitating subsequent craniectomies and ventriculostomy) Coronal C- CT through the level of the orbits; bone window • Complex displaced fracture of the right superior lateral orbital rim • Non-displaced fracture of the left lateral orbital wall • Bilateral comminuted orbital floor fractures • Depressed orbital floor fracture on the right AGFA, MGH Sagittal C- CT through the level of left orbit; bone window Patient AA revisited: Orbital injury on CT, soft tissue window Coronal C- CT through the level of the orbits; soft tissue window AGFA, MGH Patient AA revisited: Orbital injury on CT, soft tissue window findings * * Coronal C- CT through the level of the orbits; soft tissue window • Extra-ocular muscles within orbit • Downward herniation of perioribital fat (HU: -60) into right maxillary sinus • Blood in bilateral maxillary sinuses • No evidence of optic nerve or extraocular muscle entrapment seen on subsequent clinic exam (PERRL; negative forced duction test) AGFA, MGH Patient AA revisited: Bilateral LeFort II fractures OUR PATIENT, AA Bilateral LeFort II fractures Anterior 3D-reformatted CT reconstruction of the face GE Vitrea 3D Workstation, MGH Patient AA revisited: Bilateral LeFort II fractures on CT Axial C- CT through the level of sphenoid; bone window Coronal C- CT through the level of the maxilla; bone window AGFA, MGH Patient AA revisited: Bilateral LeFort II fractures on CT, Findings • Bilateral fractures of the pterygoid processes of the sphenoid (defines all LeFort maxillary fractures) Axial C- CT through the level of sphenoid • Bilateral medial orbital wall fractures resulting in pyramidal pattern of the LeFort II fracture AGFA, MGH Coronal C- CT through the level of the maxilla Patient AA revisited: Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures OUR PATIENT, AA Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures Anterior 3D-reformatted CT reconstruction of the face GE Vitrea 3D Workstation, MGH Patient AA revisited: Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures on CT Axial C- CT through the level of the ethmoid and sphenoid sinuses Bone window Axial C- CT through the level of the nasal bones Bone window Patient AA revisited: Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures on CT, Findings (with blood in both sinuses) * * Axial C- CT through the level of the ethmoid and sphenoid sinuses Bone window Axial C- CT through the level of the nasal bones Bone window AGFA, MGH Patient AA revisited: Summary of all fractures OUR PATIENT, AA Severely comminuted, complex frontal bone fractures R. superior lateral orbital rim fracture L. lateral orbital wall fracture Bilateral orbital floor fractures Bilateral LeFort II fractures Anterior 3D-reformatted CT reconstruction of the face Comminuted fractures of the ethmoid and sphenoid sinuses, nasal bone fractures GE Vitrea 3D Workstation, MGH Patient AA revisited: Follow-up OUR PATIENT, AA POST-OP • Due to elevated intracranial pressure, underwent bifrontal craniectomies • Left ventriculostomy tube was placed • ORIF of frontal sinus fracture Anterior 3D-reformatted CT reconstruction of the face post bifrontal craniectomies with ventriculostomy tube placement, and ORIF of comminuted frontal sinus fractures GE Vitrea 3D Workstation, MGH Patient AA revisited: Post craniectomies and ventriculostomy tube imaging Oblique 3D-reformatted CT reconstruction of the face post bifrontal craniectomies with ventriculostomy tube placement Sagittal C- CT Head post bifrontal craniectomies with ventriculostomy tube placement GE Vitrea 3D Workstation, MGH AGFA, MGH Patient AA revisited: List of subsequent craniofacial reconstructive procedures • Bilateral arch bar placement with intermaxillary fixation • ORIF of right zygomaticofrontal suture • ORIF of right orbital floor fracture with reconstruction of the floor with alloplastic implant • ORIF of bilateral LeFort II fractures • Closed reduction of the nasal fractures Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Agenda ` Background ` Normal craniofacial skeletal anatomy ` Shattered anatomy: Intro to patient AA ` Menu of radiologic tests ` Patient AA revisited ` Conclusions Conclusions • Craniofacial trauma can be devastating if not acutely recognized and managed • The recognition of craniofacial trauma depends heavily on radiologic imaging since the clinical exam is unreliable (60% of facial fractures are missed clinically) • Facial CT is the gold standard in the evaluation of facial trauma: facial radiographs are outdated, except for Panorex which still has utility when used in conjunction with CT in the evaluation of mandibular fractures • 3D CT reconstructions provide useful information in surgical planning Acknowledgments • • • • • • • Gillian Lieberman, MD Yoon S. Chun, MD Hillary Kelly, MD Gregory Czuczman, MD David Li, MD Maria Levantakis Linda Burke References 1- Singer AJ, Hollander JE, Quinn JV: Evaluation and management of traumatic lacerations. N Engl J Med. 1997; 337:1142 2- Bagheri SC, Dimassi M, Shahriari A, et al. Facial Trauma Coverage Among Level-1 Trauma Centers of the United States. J Oral Maxillofac Surg. 2008; 66(5):963-7 3- Holmes S. Facial Trauma – who should provide care? Br J Oral Maxillofac Surg. 2009; 47:179-81 4- Aksoy E, Unlu E, Sensoz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J Craniofac Surg. 2002; 13(6):772-5 5- Manson P, Clark N, Robertson B, Crawly W. Comprehensive management of pan facial fractures. J Craniomaxillofac Trauma. 1995; 11:43-56 6- Lee SS, Huang SH, Wu SH, et al. A Review of Intraoperative Airway Management for Midface Facial Bone Fracture Patients. Ann Plast Surg. 2009;63(2):162-166 7- Rehm CG, Ross SE. Diagnosis of Unsuspected Facial Fractures on Routine Head Computerized Tomographic Scans in the Unconscious Multiply Injured Patient. J Oral Maxillofac Surg.1995;53:522-54 8- Chen TW, Ng SY, Whaites EJ. Interpretation of skull radiographs for facial fractures by medical staff working in UK emergency departments: a pilot study. Dentomaxillofac Radiol. 2003;32(3):166-72 9- Tanrikulu R and Erol B. Comparison of computed tomography with conventional radiography for midfacial fractures. Dentomaxillofac Rad. 2001; 30:141-146 10- Reuben AD, Watt-Smith R, Dobson D, et al. A comparative study of evaluation of radiographs, CT and 3D reformatted CT in facial trauma: what is the role of 3D? Br J Radiol 2005; 78:198–201 11- Alder ME, Deahl ST, Matteson SR. Clinical Usefulness of Two-Dimensional Reformatted and ThreeDimensionally Rendered Computerized Tomographic Images: Literature Review and a Survey of Surgeons' Opinions. J Oral Maxillofac Surg. 1995; 53(4):375-86 12- Romeo A, Pinto A, Cappabianca S, et al. Role of multidetector row computed tomography in the management of mandible traumatic lesions. Semin Ultrasound CT MRI. 2009; 30:174-180 13- Wolfe SA, Ghurani R, Podda S, et al. An examination of posttraumatic, postsurgical orbital deformities: conclusions drawn for improvement of primary treatment. Plast Reconst Surg. 2008; 122(6):1874