Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
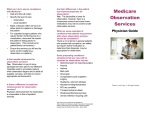
VOL 19, NO. 4, 1993 Who Should Receive High-Cost Mental Health Treatment and for How Long? by Robert Rosenheck, Louis Massari, and Linda Frisman Abstract tients to receive expensive treatment. During the past decade, experimental studies have suggested that a number of costly mental health interventions such as intensive case management (Stein and Test 1980; Olfson 1990) and clozapine pharmacotherapy (Honigfeld and Patin 1990; Meltzer et al. 1990) may offer substantial benefits to many chronically mentally ill patients. However, in view of both continuing pressure to reduce the nation's health care expenditures (Schroeder and Cantor 1991) and limited funding for public mental health programs in many parts of the country (Reid 1990; New York Times 1991), it seems likely that high-cost mental health services will have to be rationed, at least in the public sector. One criterion that has been used to select patients for costly services is a recent history of high service use (Olfson 1990; Revicki et al. 1990). If there is considerable variation in the cost of inpatient treatment of the mentally ill, it may be cost-efficient to use "high-cost" alternative treatments for those who use hospitals frequently but not for others. Despite the widespread recognition that targeting expensive services to high-cost patients is advantageous, systematic strategies for rationing have not been previously discussed. Such strategies would ideally identify patients for whom high-cost interventions are most likely to be cost-effective without excessively restricting the eligible Reprint requests should be sent to Dr. R. Rosenheck, NEPEC (182), VA Medical Center, 950 Campbell Ave., West Haven, CT 06516. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 The use of some recently developed and promising mental health treatments is likely to be restricted by their high cost. Cost-effectiveness studies, however, suggest that high treatment costs may be offset by associated reductions in inpatient service use. In view of the considerable variation in the cost of inpatient treatment for the mentally ill, it may be cost-efficient to use high-cost treatments for frequent hospital users but not for others. To illustrate this principle, we examine 9-year trends in inpatient costs incurred by schizophrenia patients discharged from Department of Veterans' Affairs medical centers across the country in fiscal year (FY) 1982. Even in the absence of specific intervention, average inpatient costs in this sample fell 49 percent, from $7,368 per patient in FY 1983 to $3,770 per patient in FY 1990, reducing the potential for inpatient cost offsets over time. Sensitivity analyses of potential inpatient cost offsets were conducted using a range estimate both for the cost of treatment and for resulting reductions in inpatient expense. Assuming effectiveness in a middle range, high-cost intervention was projected to be cost-neutral for the 25 percent of the sample with the highest rates of baseline hospital use for a duration of 1-3 years. Although our specific model had low predictive power, the projection of cost offsets in large mental health systems deserves further examination and may prove to be one useful criterion, in addition to clinical effectiveness, for selecting pa- 843 SCHIZOPHRENIA BULLETIN 844 This article presents national data from the Department of Veterans Affairs' (VA) health care system to illustrate this concept. Using these data we (1) trace long-term inpatient service usage and costs among schizophrenia pa- tients; (2) determine whether baseline usage is significantly related to future inpatient costs; (3) identify subgroups of patients for whom high-cost treatment may result in inpatient cost offsets sufficient to produce overall costneutrality; and (4) project the number of years during which inpatient costs may be offset. Methods Sources of Data. Data for this study were derived from four computerized VA data bases: (1) the Patient Treatment File (PTF), (2) the Census file, (3) the Outpatient file, and (4) the Compensation and Pension (C&P) file. The PTF contains discharge abstracts for all VA discharges occurring during each fiscal year (FY) (October 1-September 30). Each record includes a unique patient identifier (scrambled Social Security number) and patient-specific data on age, race, marital status, and current VA compensation and pension status. Also included are admission and discharge dates; codes identifying the discharging service (psychiatry, medicine, surgery, etc.); and both a primary discharge diagnosis (the diagnosis responsible for the length of stay) and up to eight secondary diagnoses, coded according to the International Classification of Diseases (ICD-9; World Health Organization 1978). The Census file includes the same data for patients remaining in VA facilities on the last day of each fiscal year. The Outpatient file (in use since 1987) documents each outpatient contact by date of contact and type of service delivered. Finally, the C&P file is a payment record that identifies all current recipients of VA benefits. Study Population. All patients discharged from VA psychiatric units with a primary diagnosis of schizophrenia (ICD-9 code 295.xx) during FY 1982 (n = 28,044) were identified, and a file was created containing all their VA hospital episodes of care from FY 1982 through FY 1990. To minimize the impact of entrenched institutional dependency on the findings, patients who had been continuously hospitalized for 1 full year or more during the 9-year period (n = 3,212) were dropped from the study.1 This exclusion left 24,832 veterans (89% of the original cohort) in the final sample. Data from all four service files show that 16,250 of these veterans (65%) used VA health services in FY 1990 and that an additional 2,058 (8%) were receiving VA compensation or pensions. Thus, 18,308 of these veterans (74%) were alive in FY 1990 and known to be eligible for VA health care services. Analyses were run on both the total study population and this subgroup. Since results were not substantially different for these two samples, we present data from the entire study sample, ensured that neither mortality nor loss of eligibility for VA services appears to have had a substantial impact on the findings. Estimating the Per Diem Cost of VA Inpatient Services. The mon'This exclusion is not meant to suggest that these patients should be excluded from high-cost treatment, but merely that they would add another complicating feature to the analysis of the data presented here. They are, of course, among the highest priority patients for such treatment. It is notable that in 82 percent of the excluded cases, the first year of the study was the year of full hospitalization. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 population or requiring costly additional data collection. Since inpatient care accounts for the largest portion of mental health costs, at least among the chronically mentally ill in the public sector (Weisbrod 1983; Dickey et al. 1986a, 1986b), a simple method for targeting high-cost treatment of these patients would be to examine factors that predict future inpatient costs. Past studies have shown that the strongest and most easily measured predictor of inpatient usage, and therefore cost, is past inpatient usage (Fontana and Dowds 1975; Gruber 1982). Although not based on an empirical predictive model, past hospitalization was used, for example, to set capitation categories for the Monroe-Livingston County capitation experiment (Lehman 1987). Similar approaches have also been tried, with varying success, in research studies of capitation in general medical domains (McClure 1984). If future inpatient expenditures could be predicted for specific patient subgroups, then it would be possible to identify prospectively those groups for whom costly interventions are most likely to yield savings large enough to offset the additional expense of high-cost treatment. Although this approach is significantly limited by the fact that it excludes the cost of community care and changes in productivity, as well as the clinical benefit of expensive treatment, it is useful as a conceptual approach that could be applied in future studies using more complete data. 845 VOL 19, NO. 4, 1993 Data Presentation and Analysis. Long-term trends in service use and costs. The total number of days of hospitalization for schizophrenia during the index year (FY 1982) was determined for each veteran. The study sample was then stratified into five baseline-year utilization groups (the three lowest quartiles, the next highest 15%, and the highest 10%). The mean days of hospital care in psychiatric and nonpsychiatric programs was then determined for each year from FY 1982 to FY 1990.2 2 A problem with data censoring may be entailed when stays cross from one fiscal year to another. To check the magnitude of this effect, we identified all patients with hospital stays crossing from one year to another (about 10% of the total) and ran the multivariate analyses with these The total cost of VA inpatient care for each veteran during each of these fiscal years was calculated using the number of days of each of the four types of inpatient care and the corresponding average per diem rates for each type of care. Trends in average VA inpatient cost over the 9 years were tabulated for each of the baseline utilization groups. One-way analysis of variance (ANOVA) was used to evaluate the significance of differences in average cost between the five groups for each year. Predictors of long-term inpatient cost. To evaluate the relationship between service use during the index year and subsequent costs, a series of bivariate correlation analyses was conducted between FY 1982 days of care and inpatient costs during each year from FY 1983 to FY 1990. To examine other factors influencing costs, multivariate analyses (ordinary least squares regression) were also conducted, in which the inpatient costs each year were again the dependent variables. In addition to baseline usage, independent variables included age, race, marital status, and compensation and pension status at the time of the index episode. Patients with either a secondary diagnosis of or a primary hospitalization for substance abuse during the index year were classified as mentally ill chemical abusers (MICAs) and dummy coded (1 = MICA, 0 = non-MICA) in the multivariate analysis. Potential cost neutrality of high-cost treatment. To identify utilization subgroups for whom high-cost interventions may be cost-neutral, the impact of these interventions was modeled using alternative projections for (1) the cost of the intervention and (2) associated savings in inpatient treatment costs. Current VA personnel and pharmacy data were used to estimate the average annual cost per patient of two high-cost services: intensive case management and clozapine pharmacotherapy. On the basis of the first author's experience implementing a VA demonstration project in intensive case management, the average annual VA cost per patient was estimated to be $4,000.3 The cost of clozapine treatment in the VA (assuming current commercial drug costs and use of the VA's own blood monitoring system) was estimated to be $5,500 per year for a patient receiving a 400-mg/day dose for 1 full year. Estimates were also made of the potential inpatient savings associated with these interventions. Data from cost studies of alternative psychosocial treatments (Weisbrod 1983; Bond 1984; Dickey et al. 1986a, 1986b) and of clozapine treatment (Meltzer et al. 1990; Revicki et al. 1990) suggest that high-cost interventions may result in inpatient savings ranging from 15 to 85 percent per patient per year, as compared with standard psychiatric treatment. The extremely wide range in effectiveness reflects differences in the quality of both the study methods and the interventions tested, and variation in the proportion of nonresponders in each study. This variation does 3 patients excluded. Since differences in results were negligible, we feel confident that this problem has a minimal effect on our findings. The case management model employed involved a mixture of direct community-based services and linkage with other providers, and it maintained a patient-staff ratio of 10:1. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 etary value of VA inpatient services was estimated using the VA's national Cost Distribution Report (CDR). The CDR is a facility-byfacility accounting system that identifies total expenditures and unit costs associated with specific types of VA inpatient and outpatient health care services. In addition to direct health care costs (e.g., personnel services, medications, and supplies), indirect costs (e.g., administration, building maintenance, engineering service, and building and equipment depreciation) are also distributed to specific health care programs using standardized accounting procedures. In this study, we used FY 1990 data from the national CDR summary to estimate average per diem costs for psychiatric care ($215.28), medical care ($496.57), surgical care ($627.30), and care in intermediate (longer term) medicine units ($294.68). SCHIZOPHRENIA BULLETIN 846 A series of logistic regression analyses was conducted to examine the relationship between baseline usage (FY 1982 hospital days) and the likelihood of meeting the cost offset threshold in each postindex year (a dichotomous outcome variable in which 1 = meeting or exceeding the cost offset threshold and 0 = being below the threshold). Results Study Sample. At the time of the index discharge, the mean age Table 1. Alternative high-cost treatment and inpatient usage conditions Condition A B C D E F 1 Estimated cost of intervention Projected inpatient cost reduction (%)' Cost offset threshold $4,000 5,500 4,000 5,500 4,000 5,500 85 85 50 50 15 15 $4,706 6,470 8,000 11,000 26,666 36,666 As compared with similar patients receiving standard psychiatric treatment. of the sample (w = 24,832) was 38 years (standard deviation [SD] = 12.3; median = 34). Sixty-three percent of the subjects were white, 28 percent were black, 8 percent were Hispanic, and 1 percent were another ethnicity. Only 22 percent were married, 46 percent had never married, 26 percent were divorced or separated, and 8 percent were widowed or of undetermined marital status. Two-thirds (66.1%) were receiving some VA benefits, including VA disability compensation for schizophrenia (46.6%), VA disability for another illness (8.5%), and VA pensions (11.0%). Eighteen percent were identified as MICAs. Inpatient Service Utilization. The sample had an average of 60 hospital days of psychiatric and 1.1 days of nonpsychiatric care during FY 1982. During the 8 years following the index 1982 discharge, 69 percent were readmitted at least once (mean = eight psychiatric readmissions). In the total sample, there was a substantial and progressive decline in mean psychiatric hospital days from 29.3 days per patient in FY 1983 to 13.4 days per patient in FY 1990, with a nearly constant and relatively small number of non- psychiatric hospital days (9% across all years). While the largest decline in psychiatric bed days of care (54%) occurred during the year following the index year, service usage continued to decline over the next 7 years at an average rate of 8 percent per year. This decline was consistently found across separate age cohorts, with the rate of decline somewhat higher among older patients (data available on request). When usage is examined for each of the baseline utilization groups (figure 1), it is notable that the FY 1982 rank order of days used by the groups is maintained across the years. However, the substantial initial differences between the groups attenuate over time. For example, the average Group V veteran used more than 15 times as many inpatient psychiatric days in FY 1982 as the average Group I veteran, 3 times as many in FY 1983, and only 1.7 times as many in FY 1990. Average Annual Inpatient Costs. As shown in figure 2, trends for average inpatient costs closely parallel usage trends. Averaging across groups, annual inpatient costs declined 48.8 percent, Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 not reduce the value of our presentation; the goal here is merely to demonstrate a conceptual approach, not to assess the specific effectiveness of these interventions. A sensitivity analysis was conducted using both the $4,000 and $5,500 estimates of treatment costs, and the high (85%) and low (15%) estimates of cost savings for specially treated patients compared with control patients, as reported in published studies. Because of the extreme range in cost savings estimates, an intermediate value (50%) was also applied to the sensitivity analysis. All six possible combinations of cost estimates and savings rates were used to determine the cost offset threshold associated with each set of treatment specifications (see table 1). A cost offset threshold is the minimum annual inpatient cost for which the expense of a high-cost intervention can be offset by resulting inpatient savings (compared with standard care controls). For example, a $4,000 intervention that results in a 50 percent inpatient savings has a cost offset threshold of $8,000. Only patients with an annual cost higher than the cost offset threshold can achieve cost-neutrality under these treatment specifications. 847 VOL 19, NO. 4, 1993 Figure 1. Inpatient usage, 1983-90 (n = 24,832) 1983 1984 1986 1985 1987 1988 1989 1990 Fiscal Year Use Grp (1982 Days) Grp I: 1-15 Days - Grp II: 16-34 Days Grp IV: 72-132 Days '— Grp V: > 132 Days Grp III: 35-71 Days Figure 2. Inpatient costs, 1983-90 (n = 24,832) Annual Inpatient Costs (Thousands) 1983 1984 1985 1986 1987 1988 1989 1990 Fiscal Year Use Grp (1982 Days) Grp I: 1-15 Days — Grp II: 16-34 Days Grp IV: 72-132 Days •- Grp V: > 132 Days from $7368 per patient in FY 1983 to $3,770 in FY 1990. (Recall that inpatient costs are not perfectly correlated with inpatient days since average costs in the four different types of bed sections are not the same.) One-way ANOVA reveals highly significant dif- Grp III: 35-71 Days ferences in average cost between baseline utilization groups in each postbaseline year (df = 4; 24,825; F = 270.2 [1983], 214.2 [1984], 160.1 [1985], 93.0 [1986], 89.0 [1987], 73.6 [1988], 49.1 [1989], and 39.4 [1990]; p < 0.0001 for each year). As with usage, the magnitude of the dif- Predictors of Long-Term Inpatient Costs Among Individual Patients. Bivariate analyses showed baseline-year usage to be significantly associated with costs in each of the subsequent years (table 2). Examination of correlation coefficients in table 2 shows that for every additional month (30 days) of FY 1982 hospitalization, FY 1983 costs increased by $1,246. The magnitude of these coefficients declines in the following years so that, by FY 1990, inpatient costs increased by only $370 for each month of FY 1982 hospitalization. Although the strongest predictor of inpatient cost remained the number of days hospitalized for schizophrenia during FY 1982, multivariate analysis showed several other factors also to be significantly associated with postindex-year inpatient costs (table 2). These factors include (1) receipt of VA disability payments for schizophrenia, (2) receipt of VA disability payments for an illness other than schizophrenia, (3) being unmarried, and (4) MICA status. Overall, however, the models' predictive ability was poor (R2 Assessing Potential Cost Off- Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 Inpatient Days ferences in inpatient cost between the groups attenuate over time. In FY 1982, Group V patients (10% of the sample) were responsible for 33 percent of all inpatient costs, but this figure dropped to 17 percent in FY 1983 and to 13 percent by FY 1990. The usage and cost data presented here thus suggest a convergence among all baseline utilization groups after 8 years around an average annual usage of 12-20 hospital days per year and an average annual cost of $3,000-$5,000. SCHIZOPHRENIA BULLETIN 848 Table 2. Muitivariate analysis of inpatient costs, FY 1983-90 1 FY 1983 FY 1984 FY 1985 FY 1986 1-Y 1987 FY 1988 FY 1989 FY 1990 Bivariate regression Intercept 1982 schizophrenia use (mos) Model r-squared (%) Multiple regression Intercept 1982 schizophrenia use (mos) Age (10-yr difference) Black Hispanic Married Service connected/ schizophrenia Service connected/other disease VA pension MICA2 Model r-squared (%) Percent of explained variance due to 1982 days 5034 1246 3.6 4322 1064 2.9 4046 867 2.2 4022 587 1.2 3740 567 1.1 3476 463 0.9 3356 379 0.6 3336 370 0.5 3349 1192 240 NS -692 -1221 2954 1023 154 NS -539 -1003 2734 834 NS NS NS -821 2784 570 NS 351 NS -557 3158 542 NS NS -595 -684 3041 445 -135 320 -642 -635 2322 354 NS 544 NS 825 2357 356 643 NS -632 1669 1731 1986 1784 1410 1434 1637 1390 1330 1496 1294 4.3 1161 896 926 3.5 1307 1366 709 2.9 1600 802 886 1.9 1729 1698 931 1.7 1238 1014 1160 1.6 1435 1041 826 1.3 1211 945 801 1.1 84.3 84.1 75.9 63.4 64.3 54.4 42.5 47.2 NS Note.—NS = nonsignificant coefficient; FY = fiscal year; MICA = mentally ill chemical abusers. 'Coefficients reported are all significant at the p < 0.05 level. set. As shown in table 3, the potential for cost-neutrality with high-cost treatment is clearly greatest among the highest baseline utilization groups. Only one inpatient cost offset year was observed among Group I and II patients, who represent 50 percent of the total sample. Under the most liberal cost-of-care and inpatient savings estimates (Condition A), savings would be equal to or greater than treatment costs for the highest two baseline utilization groups for all 8 years. However, in view of the progressive decline in an- nual inpatient costs over the years, cost offsets resulting in total costneutrality are less likely in later years under midrange conditions (C and D in table 3). Under the midrange conditions, cost-neutrality would be predicted to occur for no more than 3 years and only Table 3. Potential cost offsets, FY 1983-90, by baseline utilization group, and FY, under six conditions of intervention costs and inpatient savings (n = 24,826) Group FY 1983 FY 1984 FY 1985 FY 1986 FY 1987 FY 1988 FY 1989 FY 1990 I (n = 6,462) II (n = 6,064) III (n = 6,120) IV (n = 3,725) V (n = 2,455) A AB ABC ABCD AB ABC ABCD A ABC ABC A AB AB A AB AB A A A A A A Note.—FY = fiscal year; A = $4,000/year intervention, 85% inpatient savings; B = $5,500/year intervention, 85% inpatient savings; C = $4,000/ year intervention, 50% inpatient savings; D = $5,500/year intervention, 50% inpatient savings; E = $4,OOO/year intervention, 15% inpatient savings; F = $5,500/year intervention, 15% inpatient savings. (Under the most conservative cost estimates [E and F], inpatient cost-neutrality would not occur for any of the groups in any year.) Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 Unstandardized correlation coefficients1 849 VOL. 19, NO. 4, 1993 Discussion The longitudinal data presented in this article reveal a wide range of inpatient service usage and cost levels among VA inpatients hospitalized with a clinical diagnosis of schizophrenia. In the index year of this study, the lowest quarnle of users accounted for only one-third as many inpatient days and dol- lars as users in the highest tenth. Just as striking as this wide variation is the substantial and sustained decline in inpatient service usage and costs during the 8 postindex years. This decline in usage is most marked among those who used the most hospital services during the index year, but it is also apparent among virtually all utilization subgroups and all age groups. These changes in usage could perhaps be explained by a general decline in bed days of care (BDOC) per patient per year in the VA during the period under study, especially after diagnosticrelated group-based budgeting was introduced in 1984. In our study population, however, BDOC per patient declined most markedly between 1983 and 1986, during which time the average BDOC per year for psychiatric inpatients in the VA increased slightly (2.4%) (Rosenheck et al. 1990). Thus, changes in usage in this study population cannot be attributed to general VA system trends. Given these data, the clinical impression that the chronically mentally ill are regular and continuous users of inpatient services has been revised. As is consistent with evidence from other longitudinal studies (e.g., Harding et al. 1987), most schizophrenia patients eventually adapt to community living, making less and less use of hospital care over time. However, inpatient service usage, although reduced, remains significant among these patients after 8 years; it averages 13 days per year at a cost of $3,770 per patient per year. Although such costs are substantial, their reduction alone would not result in savings large enough to offset high-cost treatment. Although this study did not address the actual inpatient cost savings of any particular mental health intervention, the data do permit us to place an upper limit on potential savings. That is, they may be used to reasonably predict usage of inpatient treatment by groups not receiving innovative treatments—that is, the control group costs against which potential savings would be compared. Although the predictive power of our models was small, the type of data presented here could allow identification of utilization subgroups for whom high-cost treatment is most likely to be costneutral. If we were assessing a cohort of patients at the end of FY 1982 for possible high-cost treatment, given the type of information presented and assuming midrange treatment conditions, Table 4. Logistic regression analyses: Odds ratios for exceeding cost-effectiveness threshold—increased likelihood for each month (30 days) of 1982 hospitalization Treatment conditions1 A B C D FY 1983 FY 1984 FY 1985 FY 1986 FY 1987 FY 1988 FY 1989 FY 1990 1.14 1.16 1.18 1.20 1.13 1.15 1.16 1.16 1.11 1.13 1.14 1.13 1.08 1.10 1.11 1.13 1.08 1.09 1.11 1.12 1.08 1.10 1.10 1.12 1.08 1.09 1.09 1.10 1.05 1.07 1.08 1.09 Note.—All odds ratios are significant at the p < 0.0001 level; FY = fiscal year. 1 For definition of treatment conditions, see table 1. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 among the highest 25 percent of FY 1982 service users. Under the most conservative cost estimates (E and F), inpatient cost-neutrality would not occur for any of the groups in any year. Table 4 reports the results of the logistic regression analysis. For the midrange scenarios, each 30-day increment of FY 1982 days increased the chances of exceeding the cost-effectiveness threshold by 18 and 20 percent (Condition C and D, respectively) in FY 1983, but only by 8 and 9 percent in FY 1990. Thus, a patient who had been hospitalized for 90 days in FY 1982 (the 81st percentile) would be 48 percent more likely than a patient with fewer hospital days to reach the cost-effectiveness threshold in 1983 under Condition B and 60 percent more likely to do so under Condition D. SCHIZOPHRENIA BULLETIN 850 psychiatric disorder, 97 percent had a second inpatient episode in which schizophrenia was the primary diagnosis. Therefore, although definitive diagnostic evidence is not available, we feel the sample does represent the typical spectrum of male public sector schizophrenia patients. Since actual treatment decisions are likely to be made on the basis of clinical diagnosis rather than standardized research assessments, it is appropriate to use clinical diagnosis to characterize patients in studies such as this one. The incompleteness of the cost data poses a somewhat more difficult problem from several points of view. In the absence of information on the use of services other than VA hospital care (e.g., outpatient treatment services, halfway houses, nursing homes, nonVA inpatient services, or the criminal justice system), it remains possible that the decline in inpatient usage and costs reported here merely reflects a transfer of the care and cost burden to other providers rather than a true decline in service use or costs. Three points, however, can be made on this issue. First, even if some proportion of the cost of care is shifted to other providers, the observation of a sharp decline in inpatient service usage after an index hospitalization is of immediate importance to those funding the inpatient portion of care. Second, data from more complete cost studies (Weisbrod 1983; Bond 1984; Dickey et al. 1986a, 1986b) suggest that 54-92 percent of all health service costs incurred by the chronically mentally ill are attributable to inpatient care provided by institutions like the VA medical centers. We therefore believe that the majority of service costs are captured in our data. Third, in view of the special entitlement of veterans to VA services and considering that more than 60 percent of the veterans in this study receive VA support payments, it seems likely that an exceptionally large proportion of the most costly services used by these veterans would come from the VA and are documented in this study. Preliminary data from an outcome study of VA frequent hospital users conducted by the first author, for example, suggest that only 2.4 percent of inpatient days and less than 20 percent of outpatient visits by VA psychiatric patients are provided by non-VA health care agencies, and that 93 percent of all VA costs among these high service users are inpatient costs. It would thus appear that most health care and social costs incurred by the veterans in this study, and the costs that are most subject to change, are the inpatient costs on which we have presented comprehensive information. It must also be recognized that patients likely to require a great deal of inpatient care may also require substantial resources from outpatient providers and others. It is thus possible that the cost of services other than VA inpatient care might be quite large and that their reduction might offset the cost of expensive intervention, even after the projected 1-3 years' duration of potential savings in VA inpatient costs. One further limitation in our cost data is the lack of information on increased productivity. Weisbrod (1983) reported increased employment earnings as a consequence of intensive community care, and casual clinical reports suggest that some schizophrenia patients may make dramatic im- Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 inpatient cost-neutrality would appear to be possible for those veterans whose index-year service use placed them in the top 25 percent of the sample for a duration of 23 years. Thus, from the perspective of inpatient cost-efficiency, (1) only a modest proportion of schizophrenia patients are candidates for high-cost treatment, and (2) it is possible to identify those subgroups that are most likely to be cost-neutral using easily obtainable data such as those presented here. The striking decline in inpatient service usage and cost over time in this population signals a notable decline in the potential for costneutrality with high-cost treatment, at least with respect to inpatient costs. Inpatient cost offsets thus do not appear likely to be sustained over very long periods. The data reported here remind mental health policymakers and administrators that high-cost mental health interventions cannot be judged globally as cost-neutral or cost-effective. Cost-neutrality or cost-effectiveness can be meaningfully established only for particular patient groups and during delineated periods of time. Several limitations of this study must be acknowledged: the lack of standardized clinical or diagnostic information on the patients studied; the incompleteness of the available usage and cost data; and the imprecise prediction of future costs. In the absence of standardized DSM-III-R (American Psychiatric Association 1987) diagnostic data, this study must not be regarded as a study of the clinical course or outcome of schizophrenia. It is notable, however, that almost half of the study sample was receiving VA disability compensation for schizophrenia and that, of those readmitted for a 851 VOL 19, NO. 4, 1993 Conclusion Fiscally responsible use of highcost interventions requires sustained attention to the patient selection process, even beyond the setting of initial entry criteria. Students of the "product life cycle of medical technology" have observed that clinical innovations that are demonstrated to be cost-effective in carefully conducted experimental studies are often applied, in subsequent and more routine clinical practice, to much broader patient populations—populations for whom they are unlikely to be cost-neutral (Williams 1983). Changing usage patterns and economic conditions may also result in changes in the costeffectiveness of treatments, and these changes should be periodically evaluated. The potential for cost neutrality or savings should not be the only criterion used to select patients to receive expensive mental health treatment, but it should surely be one consideration, in addition to demonstrable clinical effectiveness, especially in times of restricted funding. References American Psychiatric Association. DSM-III-R: Diagnostic and Statistical Manual of Mental Disorders. 3rd ed., revised. Washington, DC: The Association, 1987. Bond, G.R. An economic analysis of psychosocial rehabilitation. Hospital and Community Psychiatry, 35:356-362, 1984. Dickey, B.; Cannon, N.L.; McGuire, T.G.; and Gudeman, J.G. The quarterway house: A two-year cost study of an experimental residential program. Hospital and Community Psychiatry, 37:1136-1143, 1986a. Dickey, B.; McGuire, T.G.; Cannon, N.L.; and Gudeman, J.G. Mental health cost models: Refinements and applications. Medical Care, 24:857-867, 1986b. Fontana, A.F., and Dowds, B.N. Assessing treatment outcome: II. The prediction of rehospitalization. Journal of Nervous and Mental Disease, 161:231-238, 1975. Gruber J.E. Paths and gates: The sources of recidivism and length of stay on a psychiatric ward. Medical Care, 20:1197-1208, 1982. Harding, CM.; Brooks, G.W.; Ashikaga, T.; Trauss, J.S.; and Breier, A. The Vermont longitudinal study of persons with severe mental illness: II. Long-term outcome of subjects who retrospectively met DSM-III criteria for schizophrenia. American Journal of Psychiatry, 144:727-735, 1987. Honigfeld, H., and Patin, J. A twoyear clinical and economic followup of patients on clozapine. Hospital and Community Psychiatry, 41:882-885, 1990. Lehman, A.F. Capitation payment and mental health care: A review of the opportunities and risks. Hospital and Community Psychiatry, 38:31-38, 1987. McClure, W. On the research status of risk-adjusted capitation rates. Inquiry, 21:205-213, 1984. Meltzer, H.Y.; Burnett, S.; Bastani, B.; and Ramirez, L.F. Effects of six months of clozapine treatment on the quality of life of chronic schizophrenic patients. Hospital and Community Psychiatry, 41:892-897, 1990. New York Times. Brutalizing the helpless. [Editorial] New York Times, December 18, 1991, p. A28. Olfson, M. Assertive community treatment: An evaluation of the experimental evidence. Hospital and Community Psychiatry, 41:634-641, 1990. Reid, W.H. Access to care: Clozapine in the public sector. Hospital and Community Psychiatry, 41:870874, 1990. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 provements in their employment status during clozapine treatment. Such benefits might, in themselves, offset the cost of treatment for some patients, even if health service usage levels remain low. This possibility cannot be assessed, however, from any currently available data. A third limitation of this study is the large unexplained variance in costs. The regression models presented here predicted only a small proportion of the total variance in cost, a proportion that, not surprisingly, declines over time. In addition to past usage, many factors, including personal history, treatment availability, and treatment compliance, influence service usage and costs among schizophrenia patients. The inclusion of standardized measures of clinical status, social supports, employment, residential status, and past outpatient service usage might further improve our models, but such data would be costly to collect. Data on inpatient use during a longer index period (e.g., 2-3 years) might also improve predictive power. Additional efforts to identify easily accessed predictors of high service usage on the national level are clearly needed for treatment-targeting efforts like the one presented here. Thus, while the data presented here do not demonstrate a full working model, they do serve to illustrate a conceptual approach that requires further development and refinement. 852 SCHIZOPHRENIA BULLETIN Weisbrod, B.A. A guide to benefitcost analysis, as seen through a controlled experiment in treating the mentally ill. Journal of Health Policy, Politics and Law, 7:808-845, 1983. Williams, A. The role of economics in the evaluation of health care technologies. In: Cuyler, A.J., and Honsberger, B., eds. Economic and Medical Evaluation of Health Care Technologies. Berlin, Germany: Springer Verlag, 1983. pp. 38-68. World Health Organization. Manual of the International Classification of Diseases, Inquiries, and Causes of Death. 9th Revision. Geneva, Switzerland: The Organization, 1978. Recent Books Falloon, I.R.H.; Laporta, M.; Fadden, G.; and Graham-Hole, V. Managing Stress in Families. New York, NY: Routledge, Chapman and Hall, 1993. 281 pp. Hatfield, A.B., and Lefley, H.P. Surviving Mental Illness: Stress, Coping, and Adaptation. New York, NY: Guilford Press, 1993. 206 pp. Howells, J.G. The Concept of Schizophrenia: Historical Perspectives. Washington, DC: American Psychiatric Press, 1991. 210 pp. Acknowledgments The authors thank Alan Fontana, Ph.D.; Gail McAvay, M.A.; Thomas McGuire, Ph.D.; Michael Neale, M.S.; Jolene Birmingham, Sc.M.; Paul Errera, M.D.; and Boris Astrachan, M.D., for their support and assistance with this article. The Authors Robert Rosenheck, M.D., is Director, Northeast Program Evaluation Center of the Department of Veterans Affairs, and Clinical Professor of Psychiatry, Yale University; Louis Massari, M.P.H., is Program Analyst, Northeast Program Evaluation Center; and Linda Frisman, Ph.D., is Project Director, Northeast Program Evaluation Center, West Haven, CT, and Associate Research Scientist, Department of Psychiatry, Yale University, New Haven, CT. Kurstak, E., ed. Psychiatry and Biological Factors. New York, NY: Plenum Press, 1991. 306 pp. Lickey, M.E., and Gordon, B. Medicine and Mental Illness: The Use of Drugs in Psychiatry. New York, NY: W.H. Freeman & Company, 1991. 443 pp. Robbins, M. Experiences of Schizophrenia: An Integration of the Personal, Scientific, and Therapeutic. New York, NY: Guilford Press, 1993. 511 pp. Downloaded from http://schizophreniabulletin.oxfordjournals.org/ at Pennsylvania State University on March 5, 2014 Revicki, D.A.; Luce, B.R.; Wechsler, J.M.; Brown, R.E.; and Adler, M.A. Cost-effectiveness of clozapine for treatment resistant schizophrenic patients. Hospital and Community Psychiatry, 41:850-554, 1990. Rosenheck, R.A.; Massari, L.; and Astrachan, B.M. The impact of DRG-based budgeting on inpatient psychiatric care in Veterans Administration medical centers. Medical Care, 28:124-134, 1990. Schroeder, S.A., and Cantor, J.C. On squeezing balloons: Cost control fails again. New England Journal of Medicine, 325:1099-1100, 1991. Stein, L.I., and Test, M.A. Alternative to mental hospital treatment: I. Conceptual model, treatment program and clinical evaluation. Archives of General Psychiatry, 37:392-397, 1980.