Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
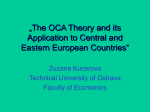
Mookerjee Yago-Baenas 1 M, 1 G, 2 T, Mehta Beecher-Jones Hooshmand-Rad 1 2 2 Jalan R , Eliot L , Shapiro D 2 R, Parihar 1 N, Sharma 1 V, Failure Group, UCL I nstitute of Liver and Digestive Health, Royal Free Cam pus, London, UK .; 2 I ntercept P harm aceuticals, I nc Background NO intrahepatic resistance NOS ↓ DDAH impacts ADMA metabolism by increasing portal pressure via ↓ NO ADMA X DDAH Cirrhosis and Inflammation rf FXR Agonists promote transcription of many genes, including DDAH. Hypothesis: OCA lowers ADMA in cirrhosis by increasing hepatic DDAH, increasing intra-hepatic NO and lowering portal pressure Aim Open label, phase 2, proof of concept study to evaluate if short-term treatment with OCA is well tolerated and can lower portal pressure in patients with cirrhosis Study Design A cohort of 12 patients with established alcoholic cirrhosis and portal hypertension were recruited based on clinical/histological and radiological criteria. The first 4 patients were assessed for drug safety and tolerance; the subsequent 8 were evaluated for hepatic venous pressure gradient (HVPG) before and after 7 days of oral OCA (10 mg/day). Key Inclusion Criteria: • Age: 18-70 yrs.; all female patients of child-bearing potential were screened for pregnancy and advised on contraception • Efficacy cohort: significant portal hypertension (HVPG) ≥ 12 mmHg • Patients with large/grade 3 varices identified by endoscopy within 6 months of screening were in a banding program at entry Key Exclusion Criteria: 105 106 109 110 113 114 115 116 20 15 10 5 105 106 109 110 113 114 115 116 120 110 100 90 80 70 0 Baseline HVPG measured pre-treatment and at the end of 7 days OCA treatment (N=8): Five of eight (5/8) patients in whom HVPG was measured, met the protocol-specified criteria for a positive response (HVPG <12mm or >15% fall). Six (6) patients had a mean reduction from 16 mmHg to 12 mmHg; a mean percent reduction of 24% (shown in blue). Two (2) patients were non-responders, shown in black. One showed no change. The other (with initial HVPG = 12 mmHg) had an HVPG increase. Of interest, this patient was an in-patient and was subsequently treated for decompensation with infection, though his infection screen at the time of study was negative. Total Bilirubin Mean Arterial Pressure (MAP) measured at the time of HVPG assessment: In 6 patients, there was a mean increase in MAP from 84 mmHg at baseline to 97 mmHg after treatment, including the 2 HVPG nonresponders (shown in black). In 2 patients (shown in red), initial MAP is higher than anticipated (based on the patients’ clinical records and measurement on subsequent follow-up). 45 80 100 50 0 Screening/Baseline End of Treatment Normal range <21 60 40 20 0 Screening/Baseline End of Treatment Normal Normal range: Range:M<41; M<41;F<33 F<33 Serum Creatinine Serum Albumin Alanine Aminotransferase 150 End Baseline End Serum Creatinine (umol/L) X L-Arginine 130 25 Albumin (g/L) hepatic blood flow Mean Arterial Pressure - 7 days OCA 10mg HVPG - 7 days OCA 10mg ALT (IU/L) Hypothesis Twelve (12) out-patients (7 male; mean age 53 yrs.) were recruited with a mean Child-Pugh score of 7.6. Nine (9) out of 12 patients dosed with10 mg OCA experienced at least one adverse event (AE). The most frequent AEs were nausea (2 patients) and headache (2 patients). All AEs in this patient group were mild in severity, non-serious and resolved without sequelae. Eight (8) patients had haemodynamic evaluation to determine the effect of short-term OCA therapy. Total Bilirubin (umol/L) • Portal hypertension is a major cause of morbidity and mortality in advanced cirrhosis and current therapies are limited in both efficacy and tolerance. • Obeticholic acid (OCA; 6 ethyl-chenodeoxycholic acid; INT-747) is a derivative of the natural FXR ligand, the primary bile acid chenodeoxycholic acid (CDCA). OCA is ~100x a more potent FXR agonist than CDCA. • Preclinical studies show that 5 days of therapy with OCA in BDL rats reduces portal pressure, mediated by an increase in eNOS activity and a reduction in hepatic concentrations of the endogenous NOS inhibitor, asymmetric dimethylarginine (ADMA) [Hepatology 2009, Vol 50, 74A]. Results MAP - mm Hg 1 Liver 1 RP , HVPG - mm Hg Intercept Pharma Logo UCL Institute of Liver and Digestive Health Effect of the FXR Agonist Obeticholic Acid on Portal Pressure in Alcoholic Cirrhosis: A Phase 2 Proof of Concept Study 40 35 30 25 Screening/Baseline End of Treatment Normal (Normalrange: Range:35-50 35-50) 120 90 60 30 0 Screening/Baseline End of Treatment NormalNormal Rangerange: male: M<66-112; 66 - 112; female: F<59-9249 - 92 Biochemical characteristics are shown for the 12 patients receiving OCA therapy. No significant change was noted in serum total bilirubin, ALT, albumin and creatinine between screening and posttherapy. Coagulation status (INR) and AST, ALP and GGT levels were also not different (data not shown) after therapy. • Patients with active, high consumption of alcohol or prior non-compliance to therapy Conclusion • Concomitant vasoactive drugs (beta blockers, nitrates, vasopressin or analogues) ≤ 6 weeks prior to randomization • Use of the following drugs within 3 months of randomization – Systemic corticosteroids – Pentoxifylline – Ursodeoxycholic acid (UDCA) – Potential hepato-toxins e.g. methyl-dopa, sodium valproic acid, isoniazid • Alcoholic hepatitis or overt infection • Co-existing disease (including cardiac, renal and pulmonary); HIV • Hepatitis B or C virus treatment <12 months of randomization HVPG: • Measurements were made using standard balloon occlusion catheter techniques, in triplicate, with the same interventionist; • Response to therapy was defined as either: HVPG reduction <12 mmHg or ≥15% fall from baseline. This pilot study demonstrated that short-term, low-dose OCA therapy was safe, well tolerated and lowered HVPG as per protocol to <12 mmHg or ≥15% fall from baseline in 5 of 8 evaluated patients, with one further patient manifesting a reduction in HVPG of over 14%. In patients manifesting a reduction in HVPG (6 /8 patients), the mean percent reduction was 24%. In 2 non-responders, one showed no change in HVPG; the other an increase from 12 mmHg at baseline. Mean arterial pressure (MAP) did not decrease across the whole cohort and aside form 2 patients with high baseline MAP, the remainder of the group showed a net increase in MAP after therapy. These data warrant further evaluation in a larger, controlled study over a longer duration to determine if the effects of therapy are sustained.