Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
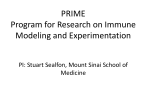
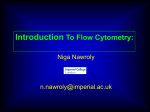
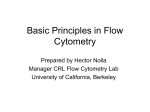
lab technology as published in CLI February/March 2004 F low Cytometry Flow cytometry for clinical microbiology by Dr. Hazel Davey Flow cytometry (FCM) is a rapid technique for the analysis of individual cells. Light scattering and fluorescence properties of cells are analysed as the cells pass through a laser beam and, in specialised instruments, cells with specific characteristics can be isolated. This review article describes FCM and discusses recent advances that may be expected to increase its use in clinical microbiology. New applications include susceptibility testing, where FCM allows death or damage to microorganisms to be identified without the necessity to observe microbial growth, as well as monitoring the status and extent of infection in HIV-positive patients. Flow cytometry (FCM) is a technique for the rapid, optical analysis of individual cells. Measurements are made by an array of detectors as the cells flow in a fluid stream through a laser (or arc lamp) beam [Figure 1]. At the sample interrogation point, light is scattered by the cells; the extent of light scatter provides information on the size and structure of the cell. In addition, fluorescence may result from the absorption and re-emission of light by chemicals that are either naturally present within the cell (autofluorescence), or which have been added to the sample prior to analysis. FCM has many advantages over conventional cytometry. Firstly, since acquisition rates of up to 10,000 cells.sec-1 can be achieved (depending on the instrument used), flow cytometric data sets often represent measurements of in excess of 100,000 cells. In contrast, measurements by microscopy often involve only a few hundred cells. The increased sample throughput of FCM leads to the acquisition of statistically significant results and the detection of rare cell types. Secondly, since FCM uses very sensitive electronic detectors to measure the intensity of scattered light or fluorescence at a given wavelength, different intensities of light scatter/fluorescence can be distinguished. By calibrating an instrument with samples of known size or fluorescent intensity, it is possible to obtain quantitative measurements. Thirdly, by using dichroic filters to optically separate light of different wavelength, flow cytometric measurements can be made on several different characteristics of each cell. Typical commercial flow cytometers allow 5-10 different parameters (e.g. size, protein content, DNA content, lipid content, antigenic properties, enzyme activity, etc.) to be collected for each cell, allowing the operator to distinguish between different cell types. Finally, since measurements are made on single cells, heterogeneity within the population can be detected and quantified in a way that cannot be achieved by other means. Whilst all commercial flow cytometers have the advantages described above, some specialised instruments (cell sorters) are able to physically separate cells on the basis of user-defined characteristics. Depending on the instrument, cells may be bulk-sorted or individual cells may be sorted onto microscope slides or microtitre/agar plates. Providing that appropriate cell staining and sample preparation methods have been used to maintain viability, sorted cells can be grown to give clonal colonies or broth suspensions for confirmation of identity via standard clinical microbiology methods. Over recent years a number of reviews of FCM have been published [see examples in reference 1]. The purpose of this review is to highlight the value of FCM for clinical samples, with particular reference to microorganisms. Dichroic Filters Flow cell Bandpass Filters Lasers & Lamps Waste Figure 1. Schematic drawing of a generalised flow cytometer. Modified with permission from a drawing by Robert Murphy, Carnegie Melon University, Pittsburgh, PA, USA. (The Purdue Cytometry CD-ROM Volume 4, J. Watson, Guest Ed., J. Paul Robinson, Publisher. Purdue University Cytometry Laboratories, West Lafayette, IN, USA. 1997, ISBN 1-890473-03-0). Clinical applications of microbial detection by FCM The detection of bacteria or yeasts in body fluids is important for the diagnosis of a number of different diseases. Urine may contain a variety of particulates, including red and white blood cells, epithelial cells, bacteria and inorganic chemical crystals. The presence and concentrations of these particulates can be used for the diagnosis of a range of diseases and disorders. Flow cytometers designed specifically for urinalysis are available commercially and these allow the simultaneous determination of many different cell types [2]. These devices have been shown to be more sensitive than manual microscopic methods [3]. In comparison to the relatively straightforward detection of bacteria in urine samples, blood is a much more challenging sample type to use. In clinical infections such as bacteraemia, concentrations of the contaminants may be of the order of 10 bacteria in 1 mL of blood, whilst the number of red blood cells is >109 per mL. The high 'background' cellular load of blood makes the detection of bacteria by microscopic methods all but impossible. Consequently, although bacteraemia is a potentially lifethreatening condition, diagnosis relies in many cases upon the growth of bacteria in media inoculated with samples of whole blood. However, methods are available to selectively lyse the erythrocytes in a blood sample, leaving a sufficiently low cell concentration to allow the rapid sample throughput capabilities of the flow cytometer to be utilised for the detection of bacteria. A number of products are now available commercially to achieve this, for example, CyLyse from Partec GmbH, Münster, Germany. Mansour and colleagues [4] developed a model system in which they used ethidium bromide labelling to nonspecifically detect Escherichia coli in blood at concentrations of 10 - 100 cells.ml-1. The sensitivity was 100 to 1000-fold better than that achieved using microscopy techniques, and took just 2 hours to perform, including sample preparation. In clinical presentations where bacterial concentrations are less than 10 per mL, a short preincubation step prior to flow cytometric analysis may be envisaged to increase the bacterial load of the sample to a level where it may be detected. The detection of specific pathogenic microorganisms in clinical samples has been much improved by the availability of monoclonal antibodies. These antibodies can be fluorescently labelled (either directly or indirectly) to enable them to be detected flow cytometrically. A variety of fluoresecent labels are available, the most common is fluorescein isothiocyanate (FITC). This has the advantage of being well-excited by the 488 nm Argon ion laser which is used as standard in most flow cytometers. Other (spectrally-distinct) molecules such as allophycocyanin, Texas Red and phycoerythrin allow multiple targets to be detected simultaneously. The labelled-antibody approach has proven to be useful for the detection of mycobacterial species from clinical (sputum) specimens [5]. Yi and colleagues showed that Mycobacteria could be detected F low Cytometry as published in CLI February/March 2004 Stain Mode of Action Results BacLight Kit: Molecular Probes – www.probes.com Propidium iodide excluded Live cells are green, dead by intact membranes. All cells are red. cells take up SYTO9 bis-(1,3-dibutylbarbituric acid) trimethine oxonol (DiBAC4(3)) Uptake by dead cells Dead cells appear green/yellow. Calcofluor White Uptake by dead cells Dead cells appear blue. 5-cyano-2,3-ditolyltetrazolium chloride (CTC) Respiratory activity Live cells appear red. Fluorescein diacetate/ Carboxy-fluorescein diacetate Enzymic activity Live cells appear green. Rhodamine 123 Uptake by live cells Live cells appear green. TO-PRO-3 / Propidium iodide Excluded by intact cell membrane Dead cells appear red. methods. A variety of fluorescent stains for assessing the viability of microorganisms have been identified [Table 1, see also reference 6] and these are particularly useful for determining the efficacy of antimicrobial compounds. Microorganisms exposed to antibiotic or antifungal compounds (either in vivo or in vitro) are compared to control (untreated) samples and appropriate stains are used to identify changes in nucleic acids, proteins, membranes, etc. Green Fluorescence Green Fluorescence Antibiotics disrupt cellular activities and the particular mode of action can be determined flow Table 1. Some fluorescent dyes used for determination of viability by FCM. cytometrically. For example, in as little as 3 hours; since Mycobacteria grow very slowantibiotic-induced damage to cell membranes can be ly in laboratory culture, a detection method that does not detected by the entry of fluorescent compounds (such as rely on growth is very advantageous for clinical diagnospropidium iodide) which are normally excluded by the tic purposes. The method described used a rabbit polyintact cell membrane. Alternatively, to deterclonal antibody against Mycobacterium species together mine the response of cells to an antibiotic, with a goat anti-rabbit IgG secondary antibody labelled which affects nucleic acid synthesis, one could with R-phycoerythrin, and detected several different use a stain such as DAPI, which binds to DNA, Mycobacterium species. However, use of a species-specifor pyronin Y, which binds to RNA. ic antibody as the primary antibody would allow the method to be used to detect M. tuberculosis specifically. In addition, FCM permits subpopulations with varying resistance to be identified and accurate Susceptibility testing assessment of the dose-response curve can also In an era of worrying and increasing levels of antibioticbe performed as part of the assay [see examples resistant pathogens, it is not surprising that understandin reference 7]. Flow cytometric susceptibility ing the interactions between microorganisms and the testing thus allows death or damage of microordrugs designed to kill them has become another imporganisms to be identified without the necessity to tant area for the clinical application of flow cytometric observe microbial growth (or lack thereof). Flow cytometric susceptibility testing can be performed in a few hours [Figure 2] and conseUntreated 40 min. quently this method has the potential to contribute to the decision of which drug or drug combination would be most appropriate for a particular patient. Red Fluorescence Red Fluorescence 3 hours Green Fluorescence Green Fluorescence 1 hour Red Fluorescence Red Fluorescence Figure 2. Antimicrobial susceptibility testing using flow cytometry. Two colour fluorescence histograms of Enterococcus faecium treated with vancomycin and stained with the FAST-2 kit (BioRad). With increasing exposure time, an increase in the number of dead and dying cells (events present in quadrants 2, 3, and 4) was observed. Data collected by Kuo-Ping Chiu and colleagues at BioRad, printed with permission (The Purdue Cytometry CD-ROM Volume 4, J. Watson, Guest Ed., J. Paul Robinson, Publisher. Purdue University Cytometry Laboratories, West Lafayette, IN, USA. 1997, ISBN 1890473-03-0). without the addition of reference controls [9]. Detection of the different lymphocyte populations is achieved using monoclonal antibodies targeted against the appropriate CD markers. The cells in a fixed volume (200 mL) of sample are counted; counting is switched on and off using an electrode to sense the depth of fluid in the sample tube. The combined detection and counting not only simplifies the procedure, thus reducing the potential for error, but also minimises costs. Future prospects A recent development that may be expected to promote the use of FCM for the analysis of clinical samples is the Amnis ImageStream System (www.amnis.com), which permits images of individual cells to be captured along with their multiparametric flow cytometric data. Thus dots on a flow cytometric data plot can be directly linked to an image of the cell. This has particular use when "abnormal" signals are detected by FCM - the operator can relate these signals back to up to six separate images of the cell to check for the presence of cell doublets, contaminating cell types or to verify the result of screening tests. HIV Figure 3. The CyFlow flow cytometer, image kindly provided by FCM has been used to great effect for monitor- Partec, GmbH. ing the status and extent of HIV infection. Whilst Over the last few years, kits designed specifically for the viral antigens can be detected by FCM [8], monitoring of flow cytometric analysis of microorganisms have become HIV infection usually relies on regular quantitation of available (see e.g. www.bdbiosciences.ca /downloads/hotlymphocyte populations. The absolute numbers of CD4+ lines/Cell_Viability_HL_Fall2003.pdf and lymphocytes and their percentage values within the total www.probes.com/ handbook/sections/1503.html). The lymphocyte populations are good indicators of the disgrowing popularity of such kits reflects, at least in part, ease and its progression. Fluorescently-labelled antibodtheir ease of use. Whilst this is to be welcomed, there is ies can be used to selectively label different types of lymsome danger that the kits may be adopted without analysis phocytes and thus FCM has an important role to play not of proper control standards. Despite the names of these only in disease surveillance, but also in determining the kits, distinguishing live and dead bacteria and yeasts is not efficacy of treatment. Ideally analysis of blood samples always straightforward and care in interpretation of the should be performed within hours of collection. results is still of great importance. Unfortunately, the majority of HIV-infected individuals are not within easy reach of the specialised laboratories In conclusion, FCM offers many advantages for clinical capable of performing these tests. A mobile flow cytommicrobiology. Recent developments are likely to open up etry laboratory has recently been developed to address further possibilities of new applications, as well as increasthis issue (Partec GmbH, Münster, Germany). The ing the use of existing flow cytometric techniques. CyFlow flow cytometer is installed in an off-road 4-wheel drive car and is powered using 12 V DC car batteries charged by solar panels [Figure 3]. The system has advantages over many flow cytometers in that lymphocyte populations can be simultaneously identified and quantified F low Cytometry References 1. Davey HM, Kell DB. Flow cytometry and cell sorting of heterogeneous microbial populations-the importance of single-cell analyses. Microbiological reviews 1996;60(4):641-696. 2. Delanghe JR, Kouri TT, Huber AR, Hannemann-Pohl K, Guder WG, Lun A, Sinha P, Stamminger G, Beier L. The role of automated urine particle flow cytometry in clinical practice. Clinica Chimica Acta 2000;301(1-2):1-18. 3. Hannemann-Pohl K, Kampf SC. Automation of urine sediment examination: A comparison of the sysmex UF100 automated flow cytometer with routine manual diagnosis (microscopy, test strips, and bacterial culture). Clinical Chemistry and Laboratory Medicine 1999;37(7):753-764. 4. Mansour JD, Robson JA, Arndt CW, Schulte TE. Detection of Escherichia coli in blood using flow cytometry. Cytometry 1985;6:186-190. 5. Yi WC, Hsiao S, Liu JH, et al. Use of fluorescein labelled antibody and fluorescence activated cell sorter for rapid identification of Mycobacterium species. Biochem Biophys Res Commun 1998;250(2):403-8. 6. Davey HM, Kaprelyants AS, Weichart DH, Kell DB. Estimation of microbial viability using flow cytometry. Current Protocols in Cytometry. New York: Wiley; 1999. p 11.3.1-11.3.20. 7. Pore RS. Ketoconazole susceptibility of yeasts by the FCST method. Current Microbiol. 1991;23:45-50. 8. McSharry JJ. Uses of flow cytometry in virology. Clinical microbiology reviews 1994;7(4):576. 9. Greve B, Cassens U, Westerberg C, Jun WG, Sibrowski W, Reichelt D, Gohde W. A new no-lyse, no-wash flowcytometric method for the determination of CD4 T cells in blood samples. Transfusion Medicine and Hemotherapy 2003;30(1):8-13. The author Hazel M. Davey, Ph.D., Postdoctoral Research Assistant, Institute of Biological Sciences, University of Wales, Aberystwyth, Ceredigion, SY23 3DD, Wales, U.K. Tel.: +44 1970 621829 Fax: +44 1970 622307 Email: [email protected] Website: http://qbab.aber.ac.uk/home.html as published in CLI February/March 2004