Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Department of Biomedical Engineering
BME 273
Professor: Paul King, Ph.D.
Advisers: Anita Mahadevan-Jansen, Ph.D.
Bart Masters
Integrated Fluorescence Probe and
Radiofrequency Ablator
April 27, 2010
Rachel Riti & Alex Walsh
Riti & Walsh
1
Abstract
More than 500,000 cases of liver cancer are documented per year, and additional liver
metastases result from approximately half of all cancers (Lin, Buttemere, & Mahadevan-Jansen,
2003). Eighty to 90% of liver cancer patients are not candidates for standard liver tumor
resection; therefore, the use of radiofrequency ablation (RFA) to damage tumor tissue has
increased (Buttemere et al., 2004). RFA is the use of high frequency electromagnetic waves to
heat tissue, generally to temperatures of 60 to 110oC (Buttemere et al., 2004). This procedure is a
minimally invasive method to destroy cancerous tissue; however, RFA is limited in its ability to
accurately detect the area of ablated tissue. Currently, thermocouples located on the ends of the
RFA electrodes are used to estimate the temperature of ablated tissue, and thus determine if
tissue death has occurred. Thermocouples are limited in several aspects as evidenced by a 4 to
19% tumor recurrence rate (Buttemere et al., 2004). A method for more accurately determining
the tissue temperature and region of tissue death is therefore necessary for prevention of cancer
recurrence. Fluorescence spectroscopy has been shown to be able to detect irreversible cell
damage during liver ablation (Anderson et al. 2004). The purpose of this project is to integrate
fibers capable of exciting and collecting fluorescence into an RFA probe for real-time
monitoring of tissue temperature during RFA procedures. Fluorescence will provide an accurate
measurement indicative of tissue death and the area of ablated tissue within the liver (Lin,
Buttemere, & Mahadevan-Jansen, 2003). One 100μm core diameter fiber was used with a 337nm
nitrogen diode laser pulsed at 20 Hz for excitation, and one 100μm core diameter fiber was used
for collection of the resultant fluorescence signal. The fluorescence of a section of bovine liver
was captured and processed throughout the experiment. Tissue degradation from the liver can be
quantified by a percentage increase in fluorescence to determine an increase in temperature in the
Riti & Walsh
2
tissue, or the shift in peak position observed in the fluorescence spectra of temperatures above
54oC (Figure 5) can also indicate tissue death. The preliminary design has shown that one 100μm
core excitation fiber and one 100μm collection fiber are sufficient to measure fluorescence.
Introduction
More than 500,000 cases of liver cancer are documented per year, and additional liver
metastases result from approximately half of all cancers (Lin, Buttemere, & Mahadevan-Jansen,
2003). The National Cancer Institute estimates that there were 22,620 new cases of liver cancer
reported in 2009 and 18,160 deaths due to liver cancer in the same year ("Liver Cancer"). Liver
cancer usually develops due to hepatitis B and C infections (Boscha et al., 2004). The fifth most
commonly occurring cancer globally, the frequency of primary liver cancer is increasing in
developed countries, and despite vaccines for hepatitis viruses, is expected to continue to
increase in the next decade (Boscha et al., 2004). Eighty to 90% of liver cancer patients are not
candidates for standard liver tumor resection; therefore, the use of radiofrequency ablation
(RFA) to damage tumor tissue has increased (Buttemere et al., 2004).
RFA is the use of high frequency electromagnetic waves to heat tissue, generally to
temperatures of 60 to 110oC (Buttemere et al., 2004). This procedure is a minimally invasive
method to destroy cancerous tissue; however, RFA is limited in its ability to accurately detect the
area of ablated tissue. Currently, thermocouples located on the ends of the RFA electrodes are
used to estimate the temperature of ablated tissue, and thus determine if tissue death has
occurred. The thermocouples are often an inaccurate measurement of the area of ablated tissue
because they are only able to provide the temperature of tissue in contact with the electrodes and
not the full region of ablation (Buttemere et al., 2004). Furthermore, thermocouple temperatures
have been observed to read lower temperatures then the temperature of the surrounding tissue
Riti & Walsh
3
(Elick & Bierbaum, 2003). This limitation of current RFA is evidenced by the tumor recurrence
rates of 4 to 19% in patients receiving RFA treatment (Buttemere et al., 2004). Radiofrequency
waves are used to destroy tissue of a 4 to 5cm diameter region around the RFA probe, and
therefore a method for more accurately determining the tissue temperature and region of tissue
death is necessary for prevention of cancer recurrence.
The thermocouples in RFA probes determine the temperature of tissue in contact with the
electrodes, and this temperature is applied to an Arrhenius integral to assess overall thermal
damage. This integral, however, uses tissue-specific constants to calculate tissue death; these
constants vary between individual patients and affect the overall accuracy of calculation.
Furthermore, the heating power and ablation duration times are fixed for RFA procedures,
resulting in varying degrees of success in tumor removal between patients (Lin, Buttemere, &
Mahadevan-Jansen, 2003). RFA probes require a feedback control conducted in real-time during
the tumor ablation procedure to accurately monitor thermal damage and determine when a tumor
has been completely ablated. Ultrasound techniques have been utilized to estimate volume of
tissue ablated during RFA but these methods are limited by large variations in predicted
temperatures and the presence of vapor bubbles in the tissue sample (Mast et al., 2008).
Fluorescence is the emission of visible light by a substance that has absorbed light of a
different wavelength; the absorption of a photon then triggers the emission of a photon with a
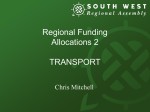
longer wavelength (Lakowicz, 2006). The autofluorescence of tissue samples is dependent upon
the temperature of the tissue sample (Masters et al.; Walsh et al.). This relationship suggests that
changes in the fluorescence signal of liver tissue can be used to quantify the temperature of tissue
as it is heated (Figure 1). Changes in fluorescence and diffuse reflectance spectra have been
characterized in liver tissue during RFA procedures (Lin, Buttemere, & Mahadevan-Jansen,
Riti & Walsh
4
2003; Buttemere, et al. 2004). Furthermore, fluorescence spectroscopy has been shown to be able
to detect irreversible cell damage during liver ablation (Anderson et al. 2004). In these three
studies, the optical spectroscopy measurements were obtained by a probe separate from the probe
used in RFA which was placed in the predicted region of ablation (Lin, Buttemere, &
Mahadevan-Jansen, 2003; Buttemere, et al. 2004; Anderson, et al. 2004).
Enucleated Eye
1
-10°C
0°C
20°C
0.5
50°C
1.5
Normalized Intensity
Normalized Intensity
1.5
1
-10°C
0°C
20°C
0.5
Excised Cornea
50°C
1.5
Normalized Intensity
Rat Skin
65°C
60°C
0
400 500 600 700
Wavelength (nm)
0
400 500 600 700
Wavelength (nm)
1
0.5
0°C
22°C
50°C
85°C
0
400 500 600 700
Wavelength (nm)
Figure 1. The normalized fluorescence intensity plotted as a function of wavelength in rat skin,
enucleated eye, and excised cornea (Walsh et al.).
The purpose of this project is to integrate fibers capable of exciting and collecting
fluorescence into an RFA probe for real-time monitoring of tissue temperature during RFA
procedures. The proposed design involves integrating fluorescence fibers with the current RFA
probe without affecting probe entry. The fluorescence of liver tissue can be measured during
ablation to assess the region of ablation. Because the fluorescence characteristics of liver tissue
change as the temperature of the tissue increases, the fluorescence fibers can be used as a
feedback mechanism during an RFA procedure. Fluorescence will provide an accurate
measurement indicative of tissue death and the area of ablated tissue within the liver (Lin,
Buttemere, & Mahadevan-Jansen, 2003).
Riti & Walsh
5
Materials and Methods
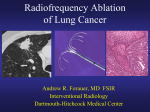
In the initial prototype, two fibers were attached along the side of the RFA probe for
measuring fluorescence (Figure 2a). Fully enclosing the fibers inside the trocar, needle, of the
Figure 2. (a) Three-dimensional design of developed design, with the optical fibers attached alongside
the trocar of the RFA probe; and (b) cross-section of the probe, showing dimensions of the trocar and
electrodes.
RFA probe would require dismantling and subsequently destroying the RFA probe. Without
fully understanding how the RFA probe was internally constructed, the efficiency of the ablation
could be compromised. The intent of this design was to demonstrate that fluorescence is a valid
technique for determination of temperature and ablation area, and would be a more accurate
measure of thermal damage than the thermocouples currently used in RFA probes; therefore, to
maintain the integrity of the probe and the optical fibers, the fluorescence fibers were placed
alongside the trocar.
The fibers were custom constructed in the Biomedical Optics laboratory in the following
manner. Three sections of 100μm core diameter fibers were cut to be six feet long. The cladding
was removed from the ends by burning away with a lighter. Epoxy glue was inserted into three
100μm fiber SMA connector and one end of each fiber was inserted into each connector. The
epoxy was allowed to harden over night. The fibers were threaded into three two-foot long
jackets which were attached to the connectors. All three of the fibers were threaded into a two
Riti & Walsh
foot jacket section to ensure that the ends remain together. Both ends of all fibers were cut and
polished to ensure smooth ends.
One 100μm core diameter fiber was used with a 337nm nitrogen diode laser pulsed at 20
Hz for excitation, and one 100μm core diameter fiber was used for collection of the resultant
fluorescence signal (Figure 2b). A white light source was used to measure diffuse reflectance
(150W halogen lamp). The fluorescence of a section of bovine liver, obtained from a local
grocery store, heated from 20 to 100oC was captured by a spectrometer and processed in a
custom LabVIEW program that acquired thermal and spectroscopic measurements throughout
the experiment (Figure 3).
Figure 3. The instrumentation setup used to capture fluorescence and temperature measurements as the
bovine liver tissue was heated.
To determine if the built fibers were fully functional, the amount of light captured from each of
the 100μm fibers was measured before the bovine liver was heated and measurements were
taken. The attenuation was then calculated using the equation:
Design criteria were established to determine the effectiveness of the design. These
criteria stipulated that neither the functionality of the RFA probe nor the functionality of the
6
Riti & Walsh
7
optical fibers could be compromised when integrated as the intent of the design is to improve the
current technique, and the current efficiency of RFA is desired. Because RFA is a minimally
invasive procedure, the design should not affect probe entry and alter the invasiveness of the
technique. Fluorescence measurements should be able to accurately indicate the area of ablation,
within 10%.
Results
The power of the laser, white light source, and both of the 100μm fibers was measured to
determine the functionality of the fibers. These measurements were used to calculate the
attenuation of light through each fiber to determine if the fibers were functional and would
provide accurate fluorescence measurements from the bovine liver (Table 1). It was determined
Power
(μW)
Laser
Fiber 1
Fiber 2
White
Light
Fiber 1
Fiber 2
Attenuation
(dB)
2.1
0.062
0.02
-15.298
-20.212
218.89
0.334
0.274
-28.165
-29.025
Table 1. The power measured of each component used in experimentation, and the calculated attenuation.
that the amount of light that was collected by the fibers in initial testing was too small to be used
for proof-of-concept measurements in tissue. Greater care when fabricating the fibers and a
method for ensuring the excitation and collection fibers remained near each other during
measurements would improve the fiber attenuation and collection of fluorescence. This probe
was able to detect background light and light from a white light source.
An alternate fluorescence probe was used to measure the temperature-fluorescence
relationship of bovine liver tissue while the tissue was heated to determine the effectiveness of
this optical solution to temperature monitoring during RFA. The alternate probe contained seven
Riti & Walsh
8
300μm fibers, arranged in a six around one configuration. The fibers in the 6 o’clock and 12
o’clock positions on the outer ring of the configuration provided the excitation, while the
remaining fibers were used for fluorescence collection.
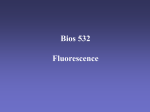
The fluorescence peak value for the probe was plotted as a function of fluorescence
intensity to determine the relationship between liver tissue fluorescence and temperature and to
determine a fluorescence change indicative of dead tissue (Figure 4). The peak intensity value
was normalized to the value closest to bovine body temperature, 38oC ("Body Temperature").
The plot shows that fluorescence peak values reach a maximum intensity between 55 and 60oC,
Normalized Fluorescence Intensity
as well as at 80oC.
Fluorescence Peak Intensity
2.5
2
1.5
1
0.5
20
40
60
80
100
Temperature (°C)
Figure 4. The fluorescence intensity of the bovine liver plotted as a function of increasing temperature of
the tissue.
Intracellular proteins denature at temperatures greater than 60oC (Curley & Izzo, 2002), so these
peaks are accurate indicators of irreversible thermal damage of tissue. Because the first
fluorescence peak occurs at the temperature of protein degradation, a 150% fluorescence
increase in intensity can be used as an indicator of tissue death and temperatures of about 60oC.
Riti & Walsh
9
A 200% increase of fluorescence is indicative of a temperature of 80oC and further thermal
damage to tissue molecules.
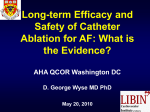
The fluorescence spectra at selected temperatures was also plotted to show the change in
spectra as the temperature changed (Figure 5). From the fluorescence spectra, the increase in
Fluorescence Intensity
Fluorescence Spectra of Liver
Tissue at Selected Wavelengths
2
75°C
1.5
1
0.5
84°C
96°C
54°C
52°C
48°C
37°C
21°C
0
400
500
600
700
Wavelength (nm)
Figure 5. Fluorescence spectra of the bovine liver tissue at selected wavelengths. The temperatures at
which the spectra were taken are indicated in the same color as the spectra are plotted.
temperature causes a peak shift of the first peak around 475 nm shifts to longer wavelengths. A
change in fluorescence peak position indicates a conformational change in the fluorophore.
Another indication of thermal damage present in the fluorescence spectra is the increase in
fluorescence of the peak at 600 nm which increases in intensity as the liver tissue is heated.
Following experimentation, the design was evaluated based on the previously stipulated
design criteria. Because the prototype connected the RFA probe and the optical fibers but the
systems remained separate entities, it was determined that the functionality of both systems was
maintained. This design, however, would affect probe entry into the abdomen and liver of a
patient as the fibers alongside the probe would require an incision for entry as they are not
equipped with a sharp end intended for traveling through the abdomen and into the liver. While a
temperature-fluorescence relationship established the ability of fluorescence to indicate thermal
Riti & Walsh 10
damage, the use of fluorescence measurements were not used to determine area of ablation in
this experiment; further experimentation with fluorescence measurements at varying lengths
from the electrodes is necessary for using fluorescence to determine ablation area.
Proposed Redesign
Based on the results of the designed probe and discussion with advisor Dr. MahadevanJansen, the proposed redesign of the integrated RFA and fluorescence probe would encase the
optical fibers in the trocar of the RFA probe and exit the needle with the electrodes during the
ablation procedure (Figure 6a). Eight sets of two 100μm core fibers will surround the central
Figure 6. (a) Three-dimensional design of proposed design, with the optical fibers enclosed in the trocar
of the RFA probe, at varying lengths; and (b) cross-section of the probe, showing dimensions of the
trocar, optical fibers, and electrodes.
RFA electrode (Figure 6b). The fiber pairs will be at varying lengths to measure the fluorescence
of the liver at different distances from the electrodes, providing several points at which thermal
damage can be assessed, allowing for quantification of the region of ablation by a computer
program (Figure 7).
Riti & Walsh 11
Figure 7. The instrumentation setup that would be used with the proposed design to capture fluorescence
and temperature measurements as tissue is heated.
The electrical circuitry of the electrodes in the RFA probe will need to be examined to
successfully house optical fibers within the trocar without compromising the efficiency of the
ablator and the fibers in order to build this probe. The fiber strength may also need to be
reinforced with additional cladding or fiber jacket as the 100μm fibers may be unable to
penetrate the liver tissue without breaking. Further strengthening of the fibers may require an
increase in the diameter of the RFA needle. This gauge increase will require consultation with
surgeons who currently perform RFA, to determine if the gauge increase necessary is compatible
with the RFA procedure.
Analysis of the Redesigned Integrated RFA and Fluorescence Probe with DesignSafe
indicated several areas of potential safety concern. The trocar needle is a concern if the probe is
used incorrectly; proper training of surgeons and hospital staff should eliminate this concern. The
process of radio frequency ablation could also have potential harmful effects if the electrodes
were activated improperly or in an inappropriate location. Training of physicians and warning
labels can prevent accidental ablation. To date, there are no known concerns with using a 337 nm
laser on living tissue. Improper disposal of the probe after use could be a health hazard, and
Riti & Walsh 12
warning labels and instructions of hospital staff for proper disposal should control the biohazard
waste.
Analysis of the manufacturing cost of both the multiple use components and the
disposable components of the integrated fluorescence-RFA probe suggests that the device would
cost about twice that of current RFA procedures (Table 2). Assuming 10% patients
Component
* Multiple Use Materials
RFA Generator
337 nm Laser
Spectrometer
Computer + Software
Total Cost:
* Single Use Materials
RFA Probe
RFA/Fluorescence Probe
- RFA electrodes
- 8 x 100µm fibers +
connectors
Grounding Pad
Total Cost:
Current Price
* Based off of current RITA
StarBurst Prices
$39,5001
$39,5001
Projected Cost
$1,5251
-
$3200^
$1751
$1700
$175
$3375
$39,500
$30002
$35003
$5000
$82,500
^ Based on the price for 8 preassembled 100-µm diameter core fibers preassembled from Ocean Optics.
Table 2: Cost analysis of the proposed RFA and fluorescence capable probe.
undergoing RFA procedures have tumor recurrence at the area of ablation (Buttemere et al.,
2004) and 10,000 RFA patients per year for ablation the benefit of this technology is $5 million
per year which greatly outweighs the cost. This is taking into account an average increased life
expectancy of 1 year for the 10% recurrence rate and a benefit of $50,000 per patient per year.
Additional costs could include development costs and animal and human trials necessary for
FDA approval. However, RFA procedures are commonly used for a variety of other diseases
Riti & Walsh 13
including kidney cancer and bone cancers; the same technology can be adapted to these
procedures, increasing the benefits.
Conclusions
Tissue degradation from the liver can be quantified in two ways. First, a percentage
increase in fluorescence can potentially be used to determine an increase in temperature in the
tissue. Second, the shift in peak position observed in the fluorescence spectra of temperatures
above 54oC (Figure 5) can also indicate tissue death. The preliminary design has shown that one
100μm core excitation fiber and one 100μm collection fiber are sufficient to measure
fluorescence. By uniting this concept with the fluorescence spectra found, eight pairs of fibers at
varying lengths will allow for the optimization of volumetric determination of ablated tissue
during the RFA procedure.
Recommendations
Recommendations for future work on this project including continuing the analysis and
design of the proposed redesigned probe. An understanding of the circuitry of the RFA
electrodes in the RFA probe is necessary for incorporating optical fibers within the RFA needle.
No ethical or societal issues need addressing at this point in the design. Once a working
prototype has been designed, the probe will need to be tested in tissue phantoms, ex vivo tissues,
and in vivo tissue studies. This process will include filing for FDA approval.
References
Anderson, C., Lin, W., Beckham, J., Mahadevan-Jansen, A., Buttemere, C., Pierce, J., Nicoud, I.,
Pinson., C., and R. Chari. "Fluorescence spectroscopy accurately detects irreversible cell
damage during hepatic radiofrequency ablation.” Surgery. 2004. 136(3):524-530.
Riti & Walsh 14
"Body Temperature." Academic American Encyclopedia. New York: American Encyclopedia,
1994: B 357.
Boscha FX, Ribesa J, Díaza M, Clériesa R. “Primary liver cancer: Worldwide incidence and
trends.” Gastroenterology. 2004;127(5):5-16.
Buttemere C, Chari RS, Anderson CD, Washington MK, Mahadevan-Jansen A, Lin W. “In vivo
assessment of thermal damage in the liver using optical spectroscopy.” J Biomed Opt.
2004;9:1018-1027.
Elick, O., Bierbaum, D. "Tissue Temperature-Controlled Radiofrequency Ablation." Pace.
2003;26(3):725-730.
Curley, S.A. and F. Izzo. "Radiofrequency ablation of primary and metastatic hepatic
malignancies." Int J Clin Oncol. 2002;7(2):72-81.
Lakowicz, Joseph R. Principles of fluorescence spectroscopy. 3rd ed. Baltimore: Springer
Science+Business Media, LLC, 2006.
Lin W, Buttemere C, Mahadevan-Jansen A. “Effect of thermal damage on the in vitro optical and
fluorescence characteristics of liver tissues.” IEEE J Sel Top Quant. 2003;9:162-170.
"Liver Cancer." National Cancer Institute, U.S. National Institutes of Health.
<http://www.cancer.gov/cancertopics/types/liver>.
Mast T, Pucke D, Subramanian S, Bowlus W, Rudich S, Buell J. "Ultrasound Monitoring of In
Vitro Radio Frequency Ablation by Echo Decorrelation Imaging." J Ultras Med.
2008;27(12):1685-1697.
Masters DB, Walsh A, Welch AJ, Mahadevan-Jansen A, Jansen D. “Effects of temperature on
fluorescence in human tissue.” Publishing Pending.
Riti & Walsh 15
Walsh A, Masters DB, Jansen ED, Welch AJ, Mahadevan-Jansen A. “The Effect of Temperature
on Fluorescence: An Animal Study, Lasers in Surgery and Medicine.” Publishing
Pending.
Cost Analysis References
1. "USA Price List," AngioDynamics.
2. Newport VSL-337
3. Ocean Optics Components
Riti & Walsh 16
Appendix 1: Innovation Workbench Solutions
Ideation Process
Project Initiation
Project Name: Integrated Fluorescent Probe and RF Ablator
1. Project objectives
1. Design a probe capable of both fluorescence measurements and RFA
2. Build the designed probe
3. Test the probe
2. Importance of the Situation
1. Surgeons are interested in determining accurate measurement of volume of ablated tissue.
2. Situation has been selected for improvement because ablation surgeries are not uncommon
procedures on liver tumors, a prevalent form of cancer.
3. If the situation is not improved, liver tumors might not be completely ablated and cancer can
metastasize, resulting in death.
4. Since thermocouples are not able to accurately show the ablation region because the tissue
surrounding the thermocouples is heated more quickly than tissue 3-4 cm away from the
thermocouples, this situation requires improvement.
5. We have consulted with our mentors, Bart Masters and Dr. Mahadevan-Jansen concerning
both RFA and fluorescence. We have also consulted with Dr. Herrel, from the VUMC,
concerning the use of RFA in the body.
6. Yes, liver tumors are not uncommon.
7. Patients with cancers of other types (not liver cancers) who can be treated with RFA may
also benefit from this new device.
Innovation Situation Questionnaire
1. Brief description of the situation
Currently, thermocouples are used to measure temperature during radio frequency ablation
(RFA) but the thermocouples do not measure ablated tissue temperature accurately and so
surgeons do not know if the entire tumor region is killed by the ablation.
2. Detailed description of the situation
2.1. Supersystem - System - Subsystems
2.1.1. System name
Radio frequency ablation
2.1.2. System structure
A RFA probe consists of:
Riti & Walsh 17
1. Connector
2. Deployment shaft
3. Main body
4. Fluid infusion port
5. Trocar
6. Multipronged electrodes
7. Thermocouples in the prongs
2.1.3. Supersystems and environment
Surgical suite
- RFA probe must be sterile
- Most RFA probes are single use
2.1.4. Systems with similar problems
- Any surgeries involving RFA
- Any system which requires a measurement of tissue temperature in a minimally invasive area
2.2. Input - Process - Output
2.2.1. Functioning of the system
- The primary function of a RFA is to heat the target tumorous tissue to a sufficient
temperature so that the tissue dies.
- The purpose of RFA is to ablate tumors in a minimally invasive manner.
2.2.2. System inputs
- Radiofrequency waves
- Laser (wavelength = 337 nm) to measure fluorescence
2.2.3. System outputs
- Fluorescence
Riti & Walsh 18
2.3. Cause - Problem - Effect
2.3.1. Problem to be resolved
There is not an effective way to measure the temperature of ablated tissue during RFA.
2.3.2. Mechanism causing the problem
- Thermocouples are attached to the probe and not the tissue
- Procedure is minimally invasive
- Ideally would like to measure the temperature of tissue in a region around the probe
2.3.3. Undesirable consequences if the problem is not resolved
- Excess ablation: death to normal tissue
- Insufficient ablation: tumor is not completely killed and continues to hinder patient
- Surgeons have to predict the region of ablation and tissue temperature reached
2.3.4. Other problems to be solved
- Will the RFA melt the fibers?
- Can fluorescence intensity from the tissue be used to predict tissue temperature?
2.4. Past - Present - Future
2.4.1. History of the problem
- Thermocouples have been used to measure tissue temperature during RFA
- Thermocouples are typically on the RFA prongs and do not contact the tissue creating
misleading temperature measurements
2.4.2. Pre-process time
The RFA is disposable, and doesn't require pre-process time.
2.4.3. Post-process time
Tissue heating takes 3-7 minutes, the RFA is disposable post-surgery.
3. Resources, constraints and limitations
3.1. Available resources
- RFA probe
- Fiber Optics
- Biomedical Optics Lab
- Alex Walsh, Rachel Riti
- Advisors: Bart Masters and Dr. Mahadevan-Jansen
- Time Resources:
November - Research
December - Develop a preliminary design
January - Reevaluate design, build fiber
February - Integrate RFA and fiber, test
March - Design critique, possible further research, begin redesign
Riti & Walsh 19
April - Complete redesign, test
3.2. Allowable changes to the system
- Small changes to the system are allowed
- Nothing can be removed from the system to effect the quality of RFA
- Nothing can be added to the system to decrease the ability to ablate
- The system must be able to be sterilized or produced for single use
3.3. Constraints and limitations
- Size of the trocar
- Size of the optical fibers
3.4. Criteria for selecting solution concepts
Increases the accuracy of temperature measurement without affecting the efficacy of RFA.
Problem Formulation and Brainstorming
Develop Concepts
1. Categorize preliminary ideas
- Thermal camera, tissue markers - both are invasive
- Optical fibers inside or outside of trocar
2. Combine ideas into concepts
- Fluorescence will not increase invasiveness of the procedure
- Optical fibers inside of the trocar will not affect probe entry
Riti & Walsh 20
Evaluate Results
1. Meet criteria for evaluating Concepts
- Test the efficiency of the optical fibers and RFA
- Do not affect probe entry
- Measure ablated region within 5% of actual region
- Tissue is dead at 10% of original fluorescence
2. Reveal and prevent potential failures
- Fibers melt from increasing temperature of the RFA electrodes - check melting temperature
of cladding and core of fibers used
- Size of the trocar is too large - consult Dr. Herrel for largest trocar that can be used in surgery
3. Apply Patterns/Lines of Evolution
Increasing ideality
Ensure that the trocar is small enough to be inserted into the liver and not cause considerable
damage to other areas of the body
Dynamization
Allow the prongs of the RFA and the optical fibers to retract independently of each other for
better data sampling.
Increasing controllability
Allow the surgeon to easily control the lengthening of the fibers versus the RFA prongs.
Riti & Walsh 21
Element universalization
Allow this probe to be used in areas of the body other than the liver.
4. Plan the implementation
- Create a probe with enclosed optical fibers
- Use 2 collection fibers, 2 excitation fibers
- Increase trocar gauge to fit the intended number of fibers and all prongs from the original
RFA
Riti & Walsh 22
Appendix 2: Design Safe Results
Riti & Walsh 23
Riti & Walsh 24