Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
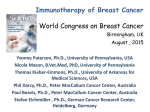
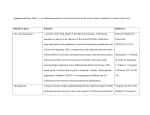
Anatomic Pathology / HER-2/NEU AMPLIFICATION AND HER-2/NEU OVEREXPRESSION HER-2/neu Gene Amplification Compared With HER-2/neu Protein Overexpression and Interobserver Reproducibility in Invasive Breast Carcinoma Mai P. Hoang, MD, Aysegul A. Sahin, MD, Nelson G. Ordòñez, MD, and Nour Sneige, MD Key Words: HER-2/neu; c-erbB-2; Fluorescence in situ hybridization; Gene amplification; Herceptin; Breast carcinoma; Immunohistochemistry; HercepTest; Interobserver reproducibility Abstract We compared the detection of HER-2/neu gene amplification by fluorescence in situ hybridization (FISH) with detection of HER-2/neu protein overexpression by immunohistochemistry using 2 antibodies on 100 archival invasive breast carcinomas. Protein overexpression for each marker was scored independently by 4 pathologists using standardized criteria, and consensus was compared with results obtained from gene amplification. The concordance rate between FISH and immunohistochemistry was 76% for e2-4001 and 91% for the HercepTest. Of the 37 cases positive by e2-4001, 21 demonstrated no gene amplification; 7 of 24 cases positive by the HercepTest demonstrated no gene amplification. However, 1 of 61 cases negative by e2-4001 showed gene amplification; none of the cases negative by the HercepTest showed amplification. The predictive values of gene amplification based on 0-1+, 2+, and 3+ immunohistochemical staining were best for cases scored as 3+ (75% for e2-4001 and 89% for the HercepTest). Complete agreement among observers for immunohistochemical scoring of e2-4001 and the HercepTest was achieved in 75 and 85 cases, respectively. The pairwise kappa agreement values were substantial for e2-4001 and substantial to almost perfect for the HercepTest. Immunohistochemical staining may be considered a useful screening test. While negative staining almost always correlated with a lack of gene amplification, positive membranous staining, especially 2+, did not predict gene amplification. The low interobserver reproducibility in separating 2+ from 3+ cases necessitates further confirmation by FISH before treatment decisions are made. 852 Am J Clin Pathol 2000;113:852-859 Carcinoma of the breast is the most common malignant neoplasm in women in the United States, and only lung cancer causes more cancer deaths in women.1 The HER2/neu proto-oncogene is amplified and overexpressed in 25% of invasive breast carcinomas, and this alteration predicts shortened disease-free survival and poor clinical outcome in cases of breast carcinoma.2-5 Also known as c-erbB-2, the HER-2/neu (human epidermal growth factor receptor) gene is located at 17q12-21.32 and is thought to be involved in the control of cell growth and development.6 It encodes a transmembrane 185-kd tyrosine kinase growth factor receptor similar to but distinct from the epidermal growth factor receptor.7 Amplification of the HER-2/neu proto-oncogene leads to marked overexpression of the membrane-bound growth factor receptor protein at the cell surface.8 Given the location of the receptor at the cell’s external surface, there has been considerable interest in developing and using specific neutralizing monoclonal antibodies that block the signaling function of these receptor tyrosine kinases. Recently, the use of recombinant humanized anti-p185HER-2/neu monoclonal antibody (Herceptin, Genentech, San Francisco, CA) in combination with cisplatin has been shown to result in clinical response in patients whose metastatic breast cancer is refractory to chemotherapy treatment and overexpresses HER-2/neu.9 The standard method to analyze HER-2/neu gene amplification has been the Southern blot hybridization test. However, this procedure requires nondegraded DNA, meaning that a large specimen, either fresh or frozen, is needed. Dilutional artifacts from the inclusion of normal cells also can mar the procedure’s results. Because it often is necessary to analyze small, paraffin-embedded tissues, other methods, such as fluorescence in situ hybridization (FISH) © American Society of Clinical Pathologists Anatomic Pathology / ORIGINAL ARTICLE and immunohistochemistry have been developed. By using specific proto-oncogene sequences as probes, FISH enables the detection of the amplified copy number on a cell-by-cell basis. On the other hand, immunohistochemistry measures the HER-2/neu protein overexpression at the membrane of the tumor cells. Although FISH and immunohistochemical (DAKO HercepTest, DAKO, Carpinteria, CA) methods have been approved by the US Food and Drug Administration as clinical tests for breast carcinoma,10 the question remains as to which is the better method to assess the HER-2/neu status of this disease, especially in the context of Herceptin therapy.11 Comparative studies of the application of FISH vs immunohistochemistry on paraffin-embedded breast carcinomas were published recently.12-14 We evaluated the detection of HER-2/neu gene amplification by FISH in comparison with the detection of HER-2/neu protein overexpression by 2 antibodies (one present in the DAKO HercepTest; the other, the Neomarkers monoclonal antibody e2-4001, Labvision, Union City, CA) on archival tissues of 100 invasive breast carcinomas. While the HercepTest is the only immunohistochemical test approved by the US Food and Drug Administration for this purpose, the Neomarkers monoclonal e2-4001 has been used by our laboratory for years, and changing to the HercepTest would result in a major increase in costs to the patients. For this reason, we included e2-4001 in our study. We also assessed interobserver variability in the evaluation of these 2 antibodies. Materials and Methods Case Selection The study material consisted of specimens from 100 consecutive cases of invasive breast carcinoma diagnosed at or referred to The University of Texas M.D. Anderson Cancer Center, Houston, in which archival material was available and the FISH test had been requested. The corresponding H&E-stained slides from all cases were reviewed. Unstained tissue sections containing tumor, as well as adjacent normal breast parenchyma when possible and corresponding to those used for the FISH test, were selected from each case for immunohistochemical staining. Fluorescence In Situ Hybridization FISH analyses were performed using the PathVysion HER-2 DNA Probe Kit (Vysis, Downers Grove, IL) according to the manufacturers’ instructions and using reagents, probes, and positive controls purchased from the manufacturers. The slides were evaluated for HER-2/neu gene copy number using an epifluorescence microscope (Zeiss, Thornwood, NY). © American Society of Clinical Pathologists The PathVysion kit uses 2 directly labeled fluorescent DNA probes: LSI HER-2/neu, which is specific for the HER-2/neu gene locus, and CEP 17, which is specific for the alpha satellite DNA sequence at the centromeric region of chromosome 17. The expected ratio of LSI HER-2/neu to CEP 17 is 2.0 for normal or unamplified breast tissue specimens. A ratio of greater than 2.0 was considered amplified. Signals were counted for 60 tumor nuclei within an area of invasive carcinoma. Signal enumeration was performed following the criteria established by Hopman et al15: overlapping nuclei were not counted, and split signals were counted as 1 chromosome component. The ductal epithelial cells served as the internal control. Stromal and inflammatory cells were excluded from analysis on the basis of the morphologic features of their nuclei. Immunohistochemical Studies For immunohistochemical studies, 4-µm-thick sections were cut from the same paraffin block that was used for the FISH analysis, mounted on charged slides, deparaffinized in xylene, and rehydrated in descending grades (100%70%) of ethanol. Sections were then subjected to heatinduced epitope retrieval by immersion in a 0.01-mol/L concentration of citrate buffer (pH 6.0) preheated to more than 90°C and heated in an electric vegetable steamer (Black and Decker, Shelton, CT) for 54 minutes. Endogenous peroxidase activity was blocked by a 5-minute treatment with 3% hydrogen peroxide in absolute methanol. The slides were incubated with the anti–HER-2/neu e24001 monoclonal antibody (1:100 dilution) on an autostainer (DAKO) for 60 minutes at room temperature. The immunoperoxidase staining was done using the LSAB2 peroxidase kit (DAKO). The antigen-antibody immunoreaction was visualized using 3-3´-diaminobenzedine as the chromogen. The slides were counterstained with Mayer hematoxylin. Similar sections also were stained for HER-2/neu according to the instructions of the manufacturer and using the reagents included in the HercepTest kit. The primary antibody included in the kit was polyclonal, raised in rabbits, and provided in a prediluted form. For each run, a composite slide of 3 formalin-fixed human breast carcinoma cell lines representing different levels of HER-2/neu protein expression (MDA-231 [0], MDA-175 [1+], and SKBR3 [3+]) was used as the control. In addition, for each case, 1 slide was incubated with normal rabbit serum instead of the primary antibody and used as a negative control. The immunohistochemical preparations were interpreted without knowledge of the results of the FISH tests and following the criteria recommended by DAKO for the HercepTest. Overexpression of HER-2/neu was defined as Am J Clin Pathol 2000;113:852-859 853 Hoang et al / HER-2/NEU AMPLIFICATION AND HER-2/NEU OVEREXPRESSION positive membranous staining in more than 10% of the neoplastic cells. Partial or incomplete, weak to moderate, and moderate to strong membranous staining in more than 10% of the tumor cells were scored as 1+ (negative), 2+ (weak positive), and 3+ (strong positive), respectively. Borderline cases between 1+ and 2+ were considered to be equivocal or indeterminate. The intensity of the staining of the adjacent normal ductal epithelium also was scored. Seventy-eight tumors were primary, and 22 represented metastases (to the lymph nodes in 18 cases, the liver in 2 cases, and to the stomach and to bone marrow in 1 case each). Fluorescence In Situ Hybridization FISH analysis was performed successfully on all 100 cases. There was 1 single fluorescent signal for each copy of the HER-2/neu gene. Seventeen (17%) cases showed gene amplification. The HER-2/neu–CEP17 ratio ranged from 2.3 to 13.2 (median, 11.8; mean, 8.6). Interobserver Reproducibility Four pathologists (M.P.H., A.A.S., N.G.O., N.S.) independently evaluated the immunohistochemical preparations in a test of interobserver reproducibility. Discrepant cases were reviewed at a multiheaded microscope to achieve consensus. The level of interobserver agreement was quantitated using the generalized kappa and pairwise kappa statistics.16 The pairwise kappa statistic is the proportion of cases in which 2 observers agree, adjusted for the level of agreement that would be expected to occur solely by chance. The generalized kappa is the summary of the agreement across all observers. The consensus opinion was viewed as conclusive. Interpretations for kappa are as described by Landis and Koch ❚Table 1❚.17 Immunohistochemical Studies and Interobserver Reproducibility e2-4001 HER-2/neu protein overexpression (consensus score) was detected in 37 (37%) of 100 analyzed cases. Sixty-one (61%) cases demonstrated no protein overexpression, and 2 (2%) cases were equivocal ❚Table 2❚. Complete agreement among the 4 observers was achieved in 75 cases (75%). Generalized kappa values indicated a substantial agreement (0.77; 95% confidence interval). The pairwise kappa value ❚Table 3❚ for agreement among observers was substantial (0.71 to 0.80). ❚Table 4❚ shows the proportion of cases assigned to each category of immunohistochemical score stratified by observers. There were significant differences in the way the observers scored cases in the weakly positive category (9%-18%). However, the differences in scoring were reduced when the weak and strong positive cases were combined. Good agreement was seen in the negative immunohistochemical category, with assigned percentages ranging from 61% to 64%. The overall concordance rate between gene amplification and protein overexpression was 75% (P < .0001). Correlation between immunohistochemical score and FISH is shown in ❚Table 5❚. Gene amplification was detected in 1 of the 61 cases with negative (0-1+) immunohistochemical staining, in neither of the 2 equivocal cases, in 1 of the 17 cases with weak (2+) immunohistochemical staining, and in 15 of the 20 cases with strong (3+) immunohistochemical staining (Table 5). As a result, the prediction of gene amplification based on Results Clinicopathologic Data The age of the patients at diagnosis ranged from 23 to 78 years (median, 51 years). Disease stage varied from T1 to T4. ❚Table 1❚ Interpretations for kappa Scores kappa Statistic Strength of Agreement <0.00 0.00-0.20 0.21-0.40 0.41-0.60 0.61-0.80 0.81-1.00 Poor Slight Fair Moderate Substantial Almost perfect ❚Table 2❚ Fluorescence In Situ Hybridization (FISH) vs Immunohistochemical Results by Consensus Score for 100 Cases* Immunohistochemical Results e2-4001 Overexpression FISH Amplification No amplification Total 16 (16) 21 (21) 37 (37) No Expression 1 (1) 60 (60) 61 (61) HercepTest Equivocal 0 (0) 2 (2) 2 (2) Overexpression 17 (17) 7 (7) 24 (24) No Expression 0 (0) 74 (74) 74 (74) Equivocal 0 (0) 2 (2) 2 (2) * Data are given as number (percentage). Neomarkers monoclonal antibody e2-4001, Labvision, Union City, CA; HercepTest, DAKO, Carpinteria, CA. 854 Am J Clin Pathol 2000;113:852-859 © American Society of Clinical Pathologists Anatomic Pathology / ORIGINAL ARTICLE ❚Table 3❚ Pairwise kappa Values Among Observers and With Consensus Score* Observer e2-4001/Observer 1 2 3 4 HercepTest/Observer 1 2 3 4 2 3 4 Consensus 0.79 0.75 0.77 0.80 0.80 0.71 0.91 0.82 0.78 0.88 0.88 0.76 0.72 0.83 0.76 0.72 0.88 0.90 0.77 0.83 * Neomarkers monoclonal antibody e2-4001, Labvision, Union City, CA; HercepTest, DAKO, Carpinteria, CA. ❚Table 4❚ Percentages of Cases Assigned to Each Category of Immunohistochemical Intensity by Each Observer* Test/Observer e2-4001 1 2 3 4 Consensus HercepTest 1 2 3 4 Consensus Negative Equivocal Weak Positive Strong Positive Weak and Strong Positive 64 62 63 61 61 0 0 0 4 2 18 15 9 13 21 18 23 28 22 16 36 38 37 35 37 75 73 72 74 74 0 1 5 0 2 7 6 3 10 7 18 20 20 16 17 25 26 23 26 24 * Neomarkers monoclonal antibody e2-4001, Labvision, Union City, CA; HercepTest, DAKO, Carpinteria, CA. ❚Table 5❚ Predictive Value of Immunohistochemical Results and Correlation Between Intensity and Fluorescence In Situ Hybridization (FISH)* Immunohistochemical Results e2-4001 Negative, 0-1+ (n = 61) Equivocal (n = 2) Weak positive, 2+ (n = 17) Strong positive, 3+ (n = 20) HercepTest Negative, 0-1+ (n = 74) Equivocal (n = 2) Weak positive, 2+ (n = 6) Strong positive, 3+ (n = 18) No. (%) of Cases Amplified by FISH 1 (2) 0 (0) 1 (6%) 15 (75) 0 (0) 0 (0) 1 (17) 16 (89) * Neomarkers monoclonal antibody e2-4001, Labvision, Union City, CA; HercepTest, DAKO, Carpinteria, CA. immunohistochemical results was 75% for those with strong positive (3+) immunohistochemical staining, 6% for the weak positive (2+) cases, and 2% for the cases negative by immunohistochemical studies. Benign ductal epithelium was present in 54 cases. Three of the 20 cases with 2+ and 3+ © American Society of Clinical Pathologists positivity demonstrated membranous staining. If this finding is considered,12 the immunohistochemical results for such cases would be considered negative; however, the predictive value for the remaining 17 cases is still low (7%). Of note, the percentage of positive tumor cells varied from 20% to 100% among positive cases, while it was more than 80% in 15 of 16 cases with concordant FISH and immunohistochemical results. HercepTest HER-2/neu protein overexpression (consensus score) was detected in 24 (24%) of 100 cases analyzed. Seventyfour cases (74%) demonstrated no protein overexpression, and 2 cases (2%) were equivocal (Table 2). Complete agreement among the 4 observers was achieved in 85 cases (85%). Generalized kappa values indicated a substantial agreement (0.78; 95% confidence interval). The pairwise kappa value (Table 3) for agreement among observers ranged from substantial to almost perfect (0.72 to 0.88). Table 4 shows the proportion of cases assigned to each category of immunohistochemical score stratified by the observers. The weak positive category Am J Clin Pathol 2000;113:852-859 855 Hoang et al / HER-2/NEU AMPLIFICATION AND HER-2/NEU OVEREXPRESSION reflected significant differences in the scoring by the observers, ranging from 3% to 10%. However, interobserver variability was reduced when the weak and strong positive cases were combined. Good agreement was seen in the negative immunohistochemical category, with assigned percentages ranging from 72% to 75%. The overall concordance rate between gene amplification and protein overexpression was 90% (P < .0001). None of the 74 cases with negative (0-1+) immunohistochemical staining, neither of the 2 cases with equivocal staining, 1 of the 6 cases with weak (2+) immunohistochemical staining, and 16 of the 18 cases with strong (3+) immunohistochemical staining demonstrated gene amplification by FISH (Table 5). The prediction of gene amplification based on immunohistochemical results was 89% for the strong positive (3+) cases and 17% for the weak positive (2+) cases. Benign ductal epithelium was present in 54 cases. In contrast with A Discussion Our comparative study shows an association between gene amplification and protein overexpression with a concordance rate of 76% for e2-4001 and 91% for the HercepTest. When the comparison was made in relation to B ❚Image 1❚ A and B, Two cases showing membranous staining for HER-2/neu protein scored as 3+ by all 4 observers (HercepTest, DAKO, Carpinteria, CA). C, Fluorescence in situ hybridization also showed amplification of HER-2/neu gene copy levels. C 856 results seen with the e2-4001 antibody, none of these cases demonstrated membranous staining. The percentage of positive tumor cells varied from 15% to 100% among the positive cases, and it was more than 75% in all 17 cases that demonstrated concordant FISH and immunohistochemical results. ❚Image 1❚ and ❚Image 2❚ illustrate examples of immunohistochemical studies in which there was complete as well as partial agreement among raters and their corresponding FISH results. Am J Clin Pathol 2000;113:852-859 © American Society of Clinical Pathologists Anatomic Pathology / ORIGINAL ARTICLE A C immunohistochemical scores (negative, 2+, 3+), the correlation between negative protein expression and lack of gene amplification was highly improved and approached 99% and 100% for e2-4001 and the HercepTest, respectively. However, among cases demonstrating protein overexpression, no gene amplification was detected in 21 (57%) of 37 positive cases stained with e2-4001 and 7 (29%) of 24 positive cases stained with HercepTest. Persons et al18 reported that 7 (7%) of 100 cases demonstrated HER-2/neu protein overexpression without HER-2/neu gene amplification. Others reported similar findings, with percentages ranging from 5%12 to 1%.13 While the differences in these reported percentages were related partially to the different antibodies being used for immunohistochemical studies and the different scoring systems, it has been speculated that some type of transcriptional or posttranscriptional regulation is responsible for the increased surface receptor expression in © American Society of Clinical Pathologists B ❚Image 2❚ A, Membranous staining for HER-2/neu protein scored as 3+ by 2 observers and 2+ (weak positive) by 2 observers; the consensus score was 2+ (HercepTest, DAKO, Carpinteria, CA). B, Fluorescence in situ hybridization (FISH) showing no amplification of gene copy levels. C, Membranous staining for HER-2/neu protein scored as +1 (weak) by 2 observers, negative by 1, and equivocal by 1; the consensus score was equivocal (HercepTest). Corresponding FISH showed no amplification of gene copy levels. the absence of gene amplification in breast carcinoma.19 Pauletti et al20 stated that 3% of breast tumors would overexpress HER-2/neu protein or messenger RNA in the absence of detectable gene amplification. Conversely, rare cases have gene amplification without a detectable level of protein overexpression. In our study, only 1 case with amplified HER-2/neu gene stained by e2-4001 was considered negative for protein overexpression, although 5% of the tumor cells showed 2+ membranous staining. Similar findings were reported by Persons et al,18 Jacobs et al,12 and Couturier et al,13 in whose studies 1 (1%) of 100, 2 (2%) of 100, and 1 (1%) of 100 cases with amplified HER2/neu gene demonstrated no protein overexpression, respectively. It is conceivable that preanalytic factors may have contributed to the discrepant results. Because our study is composed partly of material submitted on a referral basis, the effects of tissue fixation and processing cannot be excluded. Am J Clin Pathol 2000;113:852-859 857 Hoang et al / HER-2/NEU AMPLIFICATION AND HER-2/NEU OVEREXPRESSION In a recent study by Jacobs et al,12 membranous staining of the normal ductal epithelium was observed, and the authors suggested that the final scoring should be based on subtracting the score of the normal ductal epithelium from the tumor score. In our study, 3 cases demonstrated membranous staining of the normal epithelium when stained with the e2-4001 antibody; however, when the immunohistochemical results were considered negative, the predictive value of the remaining cases was still low. On the other hand, with the HercepTest, none of the cases showed positive staining of the benign epithelium. Therefore, the HercepTest is a more reliable immunohistochemical stain, especially in cases of metastasis wherein no normal breast epithelium would be available for evaluation. Although immunohistochemistry is less technically challenging and more rapid than FISH, the subjective measurement of staining intensity and the variability among various antibodies make FISH a more reliable test in selected cases. Since more than 50% of invasive breast carcinomas are HER-2/neu negative, and the negative predictive value for immunohistochemistry is 99% or more, it is conceivable that immunohistochemistry should be considered as a screening test. Because the majority of the discrepant cases were in the 2+ or weak positive group, confirmation of these cases by FISH is especially necessary. Clinical trials have shown that disease responds to Herceptin therapy only in cases with 3+ overexpression; as a result, most clinical trials involve patients whose tumor samples display 3+ overexpression.21,22 The lack of clinical response in 2+ cases on one hand and the lack of correlation with gene amplification on the other (6%-17%) suggest that weak (2+) overexpression is not specific to gene amplification, and, therefore, confirmation of these cases by FISH is necessary before therapy. We have shown that the HercepTest has better correlation with FISH and less interobserver variability than e24001. However, both e2-4001 and the HercepTest may be considered good screening tests because in 99% and 100%, respectively, of the cases with negative (0-1+) staining, FISH results were concordant. Weak (2+) overexpression of the HER-2/neu protein especially shows low correlation with gene amplification for both immunohistochemical stains. This finding, coupled with the low interobserver reproducibility in separating 2+ from 3+ cases, necessitates further confirmation of these cases with FISH in the settings of clinical trials and treatment decisions. Additional prospective studies to assess the predictive value of FISH in conjunction with immunohistochemistry and with patient responses to Herceptin are warranted. From the Department of Pathology, the University of Texas M.D. Anderson Cancer Center, Houston. 858 Am J Clin Pathol 2000;113:852-859 Address reprint requests to Dr Sneige: The University of Texas M.D. Anderson Cancer Center, Dept of Pathology, Box 53, 1515 Holcombe Blvd, Houston, TX 77030. Acknowledgments: We thank Thomas Brooks, Raju Nandagiri, Leslie E. Nesbitt, and Emily Tarco, for technical assistance and Edward N. Atkinson, MD, for statistical analysis. References 1. NIH Consensus Conference. Treatment of early-stage breast cancer. JAMA. 1991;265:391-395. 2. Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235:177-182. 3. Slamon DJ, Godolphin W, Jones LA, et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science. 1989;244:707-712. 4. Press MF, Berstein L, Thomas L, et al. HER-2/neu gene amplification characterized by fluorescence in situ hybridization: poor prognosis in node negative breast carcinomas. J Clin Oncol. 197;15:2894-2904. 5. Seshadri R, Firgaira FA, Horsfall DJ, et al. Clinical significance of HER-2/neu oncogene amplification in primary breast cancer. The South Australian Breast Cancer Study Group. J Clin Oncol. 1993;11:1936-1942. 6. Popescu NC, King CR, Kraus MH. Localization of the human erbB-2 gene on normal and rearranged chromosomes 17 to bands q12-21.32. Genomics. 1989;4:362-366. 7. Bargmann CI, Hung M-C, Weinberg RA. The neu oncogene encodes an epidermal growth factor receptor–related protein. Nature. 1986;319:226-234. 8. Gullick WJ. The role of the epidermal growth factor receptor and the c-erbB-2 protein in breast cancer. Int J Cancer Suppl. 1990;5:55-61. 9. Pegram MD, Lipton A, Hayes DF, et al. Phase II study of receptor-enhanced chemosensitivity using recombinant humanized anti-p185HER-2/neu monoclonal antibody plus cisplatin in patients with HER-2/neu-overexpressing metastatic breast cancer refractory to chemotherapy treatment. J Clin Oncol. 1998;16:2659-2671. 10. Graziano C. HER-2 breast assay, linked to Herceptin wins FDA’s okay. CAP Today. 1998;12:13-16. 11. McNeil C. How should HER2 status be determined? J Natl Cancer Inst. 1999;91:111. 12. Jacobs TW, Barnes MJ, Yazji H, et al. Comparison of fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) for the evaluation of HER-2/neu. J Clin Oncol. 1999;17:1974-1982. 13. Couturier J, Nicolas A, Beuzeboc P, et al. High correlation between ERBB2 amplification detected by FISH and gene overexpression detected by immuno-histochemistry in breast cancers [abstract]. Mod Pathol. 1999;12:18A. 14. Jimenez RE, Wallis T, Tabaczka P, et al. Fluorescent in situ hybridization (FISH) vs immunohistochemistry (IHC) for determination of HER-2/neu status in breast cancer [abstract]. Mod Pathol. 1999;12:23A. 15. Hopman AH, Ramaekers FC, Raap AK, et al. In situ hybridization as a tool to study numerical chromosome aberrations in solid bladder tumors. Histochemistry. 1988;89:307-316. © American Society of Clinical Pathologists Anatomic Pathology / ORIGINAL ARTICLE 16. Fleiss JG. Statistical Methods for Rates and Proportions. New York, NY: Wiley; 1981:225-232. 17. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159-174. 18. Persons DL, Borelli KA, Hsu PH. Quantitation of HER2/neu and c-myc gene amplification in breast carcinoma using fluorescence in situ hybridization. Mod Pathol. 1997;10:720-727. 19. Earp HS, Dawson TL, Li X, et al. Heterodimerization and functional interaction between EGF receptor family members: a new signaling paradigm with implications for breast cancer research. Breast Cancer Res Treat. 1995;35: 115-132. 20. Pauletti G, Godolphin W, Press MF, et al. Detection and quantitation of HER-2/neu gene amplification in human breast cancer archival material using fluorescence in-situ hybridization. Oncogene. 1996;13:63-72. © American Society of Clinical Pathologists 21. Ingle BJ, Pritchard K, Shepard L, et al. Initial report of the SWOG biological correlative study of C-ERB-2 expression as a predictor of outcome in a trial comparing adjuvant CAF T with tamoxifen (T) alone [abstract]. Proc ASCO. 1998;17. Abstract 374. 22. Shak S, Paton V, Bajamonde A. Addition of Herceptin (humanized anti-HER2 antibody) to first-line chemotherapy for HER2 overexpressing metastatic breast cancer (HER2 +/MBC) markedly increases anticancer activity: a randomized, multinational controlled phase III trial [abstract]. Proc ASCO. 1998;17. Abstract 377. Am J Clin Pathol 2000;113:852-859 859