Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
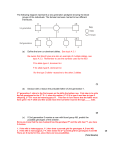
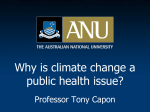
Vol. 9, 557–562, June 2000 Cancer Epidemiology, Biomarkers & Prevention Genetic Polymorphisms of N-Acetyltransferases 1 and 2 and Gene-Gene Interaction in the Susceptibility to Childhood Acute Lymphoblastic Leukemia1 Maja Krajinovic, Chantal Richer, Hugues Sinnett, Damian Labuda, and Daniel Sinnett2 Service d’Hématologie-Oncologie, Centre de Cancérologie Charles-Bruneau, Centre de Recherche, Hôpital Sainte-Justine (M. K., C. R., H. S., D. L., D. S.), and Département de Pédiatrie, Université de Montréal, Montreal, Quebec, H3T 1C5 Canada (D. L., D. S.). Abstract Acute lymphoblastic leukemia (ALL) is the most common pediatric cancer. In utero and postnatal exposures to various carcinogens may play a role in the etiology of this disease. N-acetyltransferases, encoded by the NAT1 and NAT2 genes are involved in the biotransformation of aromatic amines present in tobacco smoke, environment, and diet. Their rapid and slow acetylation activity alleles have been shown to modify the risk to a variety of solid tumors in adults. To investigate the role of NAT1 and NAT2 variants as risk-modifying factors in leukemogenesis, we conducted a case-control study on 176 ALL patients and 306 healthy controls of FrenchCanadian origin. Slow NAT2 acetylation genotype was found to be a significant risk determinant of ALL (odds ratio, 1.5; 95% confidence interval, 1.0 –2.2) because of overrepresentation of the alleles NAT2*5C and *7B and underrepresentation of NAT2*4. Besides a slight increase in NAT1*4 allele frequency among cases, no independent association of NAT1 acetylation genotypes and ALL risk was observed. However, the risk associated with NAT2 slow acetylators was more apparent among homozygous individuals for NAT1*4 (odds ratio, 1.9; 95% confidence interval, 1.1–3.4). When NAT2 slow acetylators were considered together with the other risk-elevating genotypes, GSTM1 null and CYP1A1*2A, the risk of ALL increased further, which showed that the combination of these genotypes is more predictive of risk then either of them independently. These findings suggest that leukemogenesis in children is associated with carcinogen metabolism and consequently related to environmental exposures. Received 10/18/99; revised 3/22/00; accepted 3/28/00. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by the Fondation Charles-Bruneau and Power Corporation Inc/ Fondation Hôpital Ste-Justine. 2 To whom requests for reprints should be addressed, at Centre de Cancérologie Charles-Bruneau, Hôpital Sainte-Justine, 3175 Côte Ste-Catherine, Montréal (Québec), H3T 1C5, Canada. Phone: (514) 345-4931; Fax: (514) 345-4731; E-mail: [email protected]. Introduction ALL3 is the most frequent form of cancer affecting children. As a sporadic cancer, it can be considered as a complex disease in which the effect of a series of low penetrance genes, modulated by external factors, modify the individual’s risk of cancer (1). Despite many efforts, little is known about leukemogenesis, particularly with respect to genetic susceptibility and environmental factors (2–5). Individuals having a modified ability to metabolize carcinogens seem to be at increased risk of cancer (see review by Perera; Ref. 6). Furthermore, infants and children may be at greater risk than adults from a variety of environmental toxicants because of differential exposure and/or physiological immaturity (7–9). Therefore, functional polymorphisms in genes encoding carcinogen-metabolizing enzymes may have relevance in determining susceptibility to pediatric cancer. Recently, we showed that the GSTM1 null and CYP1A1*2A genotypes were both significant predictors of ALL risk in children (10), which suggests that polymorphisms in genes that encode carcinogen-metabolizing enzymes may indeed play a role in leukemogenesis. N-acetyltransferases 1 (NAT1) and 2 (NAT2) are conjugating enzymes involved in the metabolism of aryl- and heterocyclic amines (11, 12). Genetic polymorphisms that have been described in both NAT1 and NAT2 genes correlate with biochemical phenotypes ranging from slow to fast acetylators (11–16). Associations have been reported between these DNA variants and the risk of a number of cancers including head and neck, lung, breast, laryngeal and bladder cancers (14, 17–21) as well as colorectal carcinomas (16, 22). Interestingly, both fast and slow NAT2 acetylators were shown to represent susceptibility factors in different carcinomas (13, 14, 19, 21–25). Such a dual effect is presumably attributable to differences in biochemical pathways of carcinogen activation in the liver and in other organs that become eventually affected (14, 21, 22). The prevalence of acetylator variants varies remarkably among different populations (11, 12). Therefore, special care has to be taken to avoid interpretation errors attributable to population heterogeneity. We recently proposed that French-Canadians who represent a population founded in the 17th century by immigrants from France (26, 27) constitute an appropriate genetic model for such genetic epidemiology studies (10). Here we report a case-control study on the relationship between DNA variants in NAT1 and NAT2 genes and the susceptibility to childhood ALL in the French-Canadian population from the Province of Quebec, Canada. We also exam- 3 The abbreviations used are: ALL, acute lymphoblastic leukemia; GSTM1 and GSTT1, glutathione-S-transferase M1 and T1; CYP1A1, cytochrome P450 1A1; NAT1 and NAT2, N-acetyltransferases 1 and 2; OR, odds ratio; CI, confidence interval; WT, wild type. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. 557 558 Role of NAT1 and NAT2 Polymorphisms in Childhood ALL Fig. 1. Schematic illustration of NAT1 allelic variants. The WT allele (NAT1*4) and allelic variants tested in this study are shown. The NAT1*3 allele is characterized by a silent C/A substitution at position 1095. When accompanied by T/A substitution at the position 1088 leading to the shift in a polyadenylation signal, it defines NAT1*10. In addition to the diagnostic polymorphism at the position 640 (Ser-to-Ala replacement at codon 214), NAT1 *11 allele is also associated with other nucleotide changes (indicated in italics): C/T at ⫺344, A/T at ⫺40, G/A at 445, G/A at 459, a 9-bp deletion between positions 1065 and 1090, and by C/A substitution at position 1095. A G-to-A substitution at position 560 (Arg to Glu replacement at codon 187) on the NAT1*10 background defines NAT1*14A allele. A C-to-T substitution at the position 559 (change of Arg-to-stop codon) defines NAT1*15 allele. Numbering of nucleotide positions for NAT1 are as in Deitz et al. (30). Fig. 2. Schematic illustration of NAT2 allelic variants. The WT allele (NAT2*4) and allelic variants analyzed in this study are shown. The NAT2*12A is characterized by an A-to-G base substitution at position 803 (Lys-to-Arg substitution at codon 268). The NAT2*5A allele is characterized by a T/C substitution at position 341 (Ile-to-Thr replacement at codon 114), which is accompanied by silent C-to-T mutation at position 481. The base substitution at the position 803 on the NAT2*5A background defines the NAT2*5B allele. NAT2*5C differs from NAT2*5B by the absence of a mutation at position 481. The NAT2*6A allele is characterized by a G/A substitution at position 590 (Arg-to-Gln replacement at codon 197). NAT2*7B allele is defined by G-to-A substitution at position 857 causing Gly-to-Glu replacement at codon 286. Numbering of positions is according to Cascorbi et al. (14). ined the effect of the combined multilocus genotypes on childhood ALL susceptibility. Materials and Methods Subjects. Childhood ALL patients (n ⫽ 176) were diagnosed in the Division of Hematology-Oncology of Ste-Justine Hospital, Montreal, Canada, between August 1988 and September 1997. They comprised 108 males and 68 females with a median age of 6.0 years. The distribution of ALL subtypes was as follows: 142 pre-B and 21 T-cell ALLs and 13 with undetermined lineage. A control group (n ⫽ 306) was randomly selected from a large institutional DNA bank. All of the participants were of French origin and resided in the Province of Quebec, Canada. The inclusion criteria for patients and controls have been described previously (10). The Institutional Review Board approved the research protocol, and informed consent was obtained from all of the participating individuals and/or their parents. Genotyping. DNA was isolated from buccal epithelial cells, peripheral blood, or bone marrow in remission as described in Baccichet et al. (28). All of the selected polymorphisms in NAT1 (C559T, G560A, T640G, T1088A, and C1095A) and NAT2 (T341C, C481T, G590A, A803G, and G857A) were revealed by allele-specific oligonucleotide (ASO) hybridization assays (29). In some cases the NAT1 and NAT2 genotypes were confirmed by PCR-RFLP as described in Deitz et al. (30) and Cascorbi et al. (14), respectively. The alleles defined by these polymorphisms are given in Fig. 1 and 2. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 1 NAT2 allele Rapid *4 *12A None 803 Slow *5A *5B *5C *6A *7B 341, 481 341, 481, 803 341, 803 282, 590 282, 857 Total a Linkage of mutations (position) Frequency of NAT2 alleles in ALL patients and controls ALL patients (n ⫽ 176) Controls (n ⫽ 291) ORa 95% CI P 25.9 0.3 0.6 2.5 0.5–0.9 0.4–15.0 0.01 0.4 2.4 44.2 1.0 24.9 1.2 1.6 0.9 3.1 1.2 2.9 0.7–3.4 0.7–1.2 1.1–8.5 0.9–1.6 1.1–7.4 0.3 0.5 0.02 0.3 0.03 n % n % 65 3 18.5 0.9 151 2 13 148 11 100 12 3.7 42.0 3.1 28.4 3.4 14 257 6 145 7 352 100 582 100 ORs were calculated from the ratio of the number of alleles of interest versus all of the other alleles in ALL patients compared with the ratio in control individuals. Statistics. The test for case-control differences in the distribution of the genotypes was based on 2 statistics. The level of significance was calculated by Fisher’s exact test. ORs were used to measure the strength of association between the tested genotypes and ALL risk. Crude ORs are given with 95% CIs. Unconditional logistic analysis was used to compute age and gender as covariables as well as the effect of combined genotypes at risk of ALL susceptibility. All of the statistical tests were based on two-tailed probability and were performed using SPSS version 7.5. Linkage disequilibrium between NAT1 and NAT2 alleles was tested with the software package GenePop (version 3.1). Results The genotypes at 10 polymorphic sites in NAT1 and NAT2 genes (Fig. 1 and 2) were obtained for 176 children with ALL and 306 healthy controls, both groups consisted of FrenchCanadians residing in the Province of Quebec, Canada. The selected polymorphisms define the most common allelic variants found in populations of European descent (11, 31). Some individuals were not successfully genotyped for the whole set of tested polymorphisms, thus explaining a certain variation in the total number of samples listed in Tables. In this study, both pre-B and T-cell ALLs were considered together because no significant differences were observed in terms of the tested genotypes (data not shown). The frequency of NAT2 alleles as well as the distribution of the genotypes in ALL patients and controls are given in Tables 1 and 2, respectively. The observed allelic frequencies were similar to those reported in other populations of European descent (11, 29). Of note, we did not observe linkage disequilibrium between NAT1 and NAT2 loci as reported elsewhere (31). The allele frequency distribution among ALL patients differed from the control group: NAT2*5C and *7B were overrepresented in the patient group, whereas NAT2*4 was underrepresented (Table 1). When genotypes were determined, we found that those predicting a slow NAT2 acetylator phenotype (so-called NAT2 slow-acetylation genotype), i.e., two copies of any “slow” allele (*5A, *5B, *5C, *6A, or *7B), was present in 64.8% of the patients as compared with 54.6% of controls (Table 2). These results suggest that slow-acetylation activity of NAT2 is associated with an increased risk of ALL (OR, 1.5; 95%CI, 1.0 –2.2; P, 0.03). At the same time, a significant decrease in NAT2 rapid-acetylation genotypes (presence of at least one copy of allele *4 or *12A) among cases pointed to a protective role of NAT2 activity (OR, 0.7; 95% CI, 0.4 –1.0; P, Table 2 Distribution of NAT2 genotypes in children with ALL and controls The distribution of NAT2 genotypes between cases and controls differs significantly, 2 ⫽ 31.126; P ⫽ 0.04. Only the genotypes detected in at least one of the groups are listed. ORs with 95% CIs and corresponding P values are given for rapid and slow acetylator genotypes (in bold), *4/*4, and *4/*12A individuals together, *4/*4 homozygous individuals, and NAT2 *4 heterozygous individuals (in italics). ALL patients Controls n % n % 5 1 2.8 0.6 20 1 Genotype Rapid acetylationa *4/*4 *4/*12A Total OR (95% CI) P 6.9 0.3 0.3 (0.1–1.0) 0.03 0.4 (0.2–1.0) 0.06 6 3.4 21 7.2 *4/*5A *4/*5B *4/*5C *4/*6A *4/*7B *5B/12A *6A/12A 2 28 0 21 3 1 1 1.1 15.9 0.0 12.0 1.7 0.6 0.6 3 75 2 30 0 1 0 1.0 25.8 0.7 10.3 0.0 0.3 0.0 Total 56 31.8 111 38.2 0.7 (0.5–1.1) 0.09 Sum of rapid 62 35.2 132 45.4 0.7 (0.4–1.0) 0.03 Slow acetylationb *5A/*5B *5A/*5C *5A/*6A *5B/*5B *5B/*5C *5B/*6A *5B/*7B *5C/*6A *6A/*6A *6A/*7B 7 1 3 29 9 38 7 1 17 2 4.0 0.6 1.7 16.5 5.1 21.6 4.0 0.6 9.7 1.1 7 1 3 51 3 64 5 0 23 2 2.4 0.3 1.0 17.5 1.0 22.0 1.7 0.0 7.9 0.7 1.5 (1.0–2.2) 0.03 Sum of slow Total 114 64.8 159 54.6 176 100.0 291 100.0 a Rapid acetylation genotype corresponds to the presence of at least one copy of NAT2*4 or NAT2*12A. b Slow acetylation genotype corresponds to the presence of two alleles with slow acetylation capacity. 0.03; Table 2), particularly in individuals homozygous for the NAT2*4 allele (Table 2). Multivariate analysis that included age and gender as covariables did not change the interpretation of these results. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. 559 560 Role of NAT1 and NAT2 Polymorphisms in Childhood ALL Table 3 NAT1 allele Linkage of mutationsa (position) *4 *3 *10 *11 *14A *15 None 1095 1088, 1095 640, 1095 560, 1088, 1095 559 Total Frequency of NAT1 alleles in childhood ALL patients and controls ALL patients (n ⫽ 155) Controls (n ⫽ 306) n % n % 244 3 51 6 5 0 78.7 1.0 16.8 1.9 1.6 0.0 447 16 122 20 5 2 73.0 2.6 19.9 3.3 0.8 0.3 310 100 612 ORb (95% CI) P 1.4 (1.0–1.9) 0.4 (0.1–1.3) 0.8 (0.6–1.1) 0.6 (0.2–1.5) 2.0 (0.6–6.9) 0.4 (0.02–8.2) 0.06 0.1 0.2 0.3 0.3 0.6 100 a Only the polymorphisms analyzed in this study are given. For instance, despite the presence of other polymorphisms associated with allele *11 (see Fig. 1), the nucleotide substitution at position 640 was considered a diagnostic change for NAT1 *11. b ORs were calculated from the ratio of the number of alleles of interest versus all other alleles in ALL patients compared with the ratio in control individuals. Table 4 Distribution of NAT1 genotypes in children with ALL and controls ALL patients Genotype n % n % 99 63.9 172 56.2 *4/*3 *4/*11 *4/*14A 1 4 3 0.6 2.6 1.9 12 14 4 3.9 4.6 1.3 Sum of */*4a 7 5.1 30 9.8 *3/*3 *3/*11 *11/*11 0 1 0 0.0 0.6 0.0 1 0 1 0.3 0.0 0.3 108 69.7 204 66.7 5 1 38 1 2 0 3.2 0.6 24.5 0.6 1.3 0.0 20 2 73 4 1 2 6.5 0.7 23.9 1.3 0.3 0.7 47 30.3 102 33.3 155 100.0 306 100.0 *4/*4a Sum of non-*10b *10/*10 *10/*3 *10/*4 *10/*11 *10/*14A *10/*15 Sum of -*10b Total Table 5 Controls OR (95% CI) P 1.4 (0.9–2.1) 0.1 Association between NAT1 and NAT2 genotypes and childhood ALL NAT1a NAT2b Cases (n ⫽ 154) Controls (n ⫽ 266) non-*4/*4 non-*4/*4 *4/*4 *4/*4 Rapid Slow Rapid Slow 25 31 31 67 64 57 56 89 OR (95% CI) P 1.0 1.9 (1.1–3.4) 0.03 a 1.0 (0.4–2.5) 1.0 1.1 (0.8–1.7) 0.5 0.9 (0.6–1.3) 0.5 a The NAT1*4 was the only NAT1 allele with increased frequency in cases versus controls; therefore, OR was estimated for homozygous and heterozygous (*/*4) NAT1*4 individuals. b Because the presence of at least one copy of the NAT1*10 allele is presumably associated with elevated acetylation capacity (16), individuals were stratified according to the presence or absence of the allele *10. The NAT1 genotyping data for the patient and the control group are reported in Tables 3 and 4. A modest increase of NAT1*4 allele is observed among ALL patients (OR, 1.4; 95% CI, 1.0 –1.9; P, 0.06) compared with the controls (Table 3), which could explain a higher, although not significant, prevalence (OR, 1.4; 95% CI, 0.9 –2.1; P, 0.1) of patients homozygous for this allele (Table 4). The patients and controls were also arbitrarily grouped based on the presence or absence of the putative rapid allele *10 (16). The frequency of NAT1*10 carriers and noncarriers did not differ between cases and controls (Table 4), which suggests that the NAT1 acetylation genotype is not independently related to overall risk of childhood ALL. Involvement of NAT1 and NAT2 enzymes in similar metabolic pathways prompted us to examine the effect of the combined genotypes for these loci (Table 5). An increase in the risk of ALL (OR, 1.9; 95%CI, 1.1–3.4; P, 0.03) for individuals with NAT2 slow acetylators that are homozygous for the NAT1*4 allele compared with the risk for individuals without these genotypes was observed. *4/*4, homozygous individuals for NAT1*4 allele; non-*4/*4, nonhomozygous individuals for NAT1*4. b Rapid, rapid acetylation genotype; Slow, slow acetylation genotype. From a previous study of the same case-control group, we reported that children carrying the GSTM1 null genotype or at least one CYP1A1*2A allele had an increased risk of ALL (10). Here, we investigated whether this risk was increased further by additionally considering NAT2 genotypes. The reference group (OR, 1.0) was defined as children having the following “lowrisk” genotypes: NAT2 rapid acetylation, presence of GSTM1, and absence of CYP1A1*2A allele. The estimated risk of ALL for all of the combinations of genotypes at risk is given in Table 6. The presence of only one risk-elevating genotype did not influence the risk. However, the overall risk of ALL increased with the number of risk-increasing genotypes (P for trend, 0.0001), with ORs of 2.7 (95%CI, 1.4 – 4.9; P, 0.002) and 3.1 (95%CI, 1.1– 8.4; P, 0.03) for two and three genotypes, respectively (Table 6). Discussion ALL in children offers a unique opportunity to examine the effect of carcinogen-metabolism genes in the risk of pediatric cancers (10). The young ages of patients and, thus, a short latency period between the appearance of the initiating mutation and the detection of tumor cells should facilitate the identification of risk factors, as compared with adult cancer patients in whom many factors come into play because of long latency periods. Here, we determined the frequencies of NAT1 and NAT2 allelic variants in French-Canadians from Quebec, Canada. This population was founded by a few thousand immigrants from France in the 17th century (26, 27). After the British conquest in the middle of 18th century, the flow of French immigrants practically ceased. However, because of a large demographic growth, this population grew naturally and expanded to about 10 million in Quebec and elsewhere in North America. Despite the founder effect (26), the overall frequencies of the genotypes tested in controls agree with those reported for other populations of European descent (11–14, 16, Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 6 Association between NAT2, GSTM1, and CYP1A1 genotypes and childhood ALL GSTM1 CYP1A1*2Aa NAT2b Cases (n ⫽ 174) Controls (n ⫽ 285) OR (95% CI) No genotypes at risk Present ⫺/⫺ Rapid 19 53 1.0 (referent) One genotype at risk Null Present Present ⫺/⫺ ⫺/⫺ ⫹/⫹; ⫺/⫹ Rapid Slow Rapid 29 33 2 60 69 9 1.3 (0.7–2.7) 1.3 (0.7–2.6) 0.6 (0.1–3.1) 0.5 0.5 0.7 64 138 1.3 (0.7–2.4) 0.5 60 9 11 69 10 5 2.4 (1.3–4.5) 2.5 (0.9–7.1) 6.1 (1.9–20.1) 0.006 0.1 0.003 80 84 2.7 (1.4–4.9) 0.002 11 10 3.1 (1.1–8.4) 0.03 Total Two genotypes at risk Null Present Null ⫺/⫺ ⫹/⫹; ⫺/⫹ ⫹/⫹; ⫺/⫹ Slow Slow Rapid Total Three genotypes at risk Null ⫹/⫹; ⫺/⫹ Slow P ⫺/⫺, absence of alleles; ⫹/⫹; ⫺/⫹, presence of at least one allele. b Rapid, rapid acetylation genotype; Slow, slow acetylation genotype (see in Table 2). a 29, 32), which suggests that the implications of our results could be extended to these groups as well. We found that children carrying NAT2 slow-acetylation genotypes were at increased risk of developing ALL (OR, 1.5; 95% CI, 1.0 –2.2), mainly because of the overrepresentation of alleles NAT2*5C and *7B. We observed a lower prevalence of the NAT2*4 allele in the patients’ group, which may suggest a protective role for this allele. The effect was more obvious in homozygous individuals as it was also reported by others (14). To our knowledge, this is the first study documenting an association between NAT2 variants and the risk of hematological malignancies, particularly in children. However, these data are in agreement with the studies of solid neoplasias in adults that report that NAT2 slow-acetylator individuals are at greater risk of head and neck, breast, and laryngeal cancers (17–19) as well as bladder cancer (20, 21). When NAT1*10 was considered alone or combined with NAT2 slow-acetylation genotype, our data provided no evidence of involvement of this allele in ALL susceptibility. In other studies, NAT1*10 has been associated with an increase of N-acetyltransferase activity (16), higher levels of DNA adducts (33), and an elevated risk of colon, bladder, or breast carcinomas (16, 23, 32). The risk of cancer was accentuated when NAT1*10 genotypes were combined with NAT2 at-risk genotypes (16, 32). However, in light of conflicting data in the literature, the role of NAT1*10 in tumorigenesis still remains unclear (34 –36). On the other hand, we noted a slight increase in the frequency of NAT1*4 among cases, which, when combined with NAT2 slow-acetylator genotypes, further increases the risk of ALL (OR, 1.9; 95% CI, 1.1–3.4). Taken together, the results for NAT1 should be interpreted with caution because the functional significance of NAT1 variants remains to be clarified. It is difficult to predict how the genotypes at risk will modify the infant’s (or fetus’) response to different exposures. Epidemiological studies have led to the suggestion that in utero and postnatal exposures to various biological, physical and chemical factors may be important determinants of childhood ALL (7, 37, 38). Children may be at greater risk than adults from toxic substances because of differential exposure or physiological immaturity (7, 9, 19). We have recently shown that the risk of ALL among children carrying certain CYP1A1 variants was modified by maternal exposure to pesticides during the pregnancy (39). Both NAT1 and NAT2 enzyme activities are detectable in human placentas (40, 41), although it seems that placental N-acetylation activity is predominantly attributable to NAT1 (11, 40 – 42). Thus, it is possible that genetically deter- mined variability in N-acetylation of aromatic amines present in different environmental and occupational pollutants like dyes, tobacco smoke, antioxidants, medications, or pesticides may confer cancer susceptibility on children (13, 14, 19, 21–25). Predominance of the competing N-oxidation in subjects with NAT2 slow acetylation would lead to the formation of aryl hydroxylamines. Because NAT1 is widely expressed in different tissue (11, 43), it can act locally, performing O-acetylation of hydroxilated arylamines, which will result in the formation of arylnitrenium ions and DNA adducts (44). Recently, we reported that the GSTM1 null genotype and the presence of at least one CYP1A1*2A allele were significant predictors of ALL risk (10). When these two genotypes were combined with genotypes predicting NAT2 slow acetylators, we found that the presence of only one risk-elevating genotype had little effect on OR estimates. However, the combination of risk-elevating genotypes seemed to confer an increased risk of ALL among the carriers compared with those with the more beneficial genotypes (OR, 2.7; 95% CI, 1.4 – 4.9; and OR, 3.1, 95% CI, 1.1– 8.4, respectively). These results are similar to those obtained in nonhematological malignancies for the combined effect of NAT2 and GSTM1 (19, 25, 45). However, the basis of synergy between CYP1A1 and NAT2 is less obvious because they are involved in different metabolic pathways. This effect could be mediated through CYP1A2 that is involved in the first step of the activation of the aromatic amines (13). It has been recently shown that CYP1A2 activity was higher in individuals with GSTM1 null genotype or heterozygous for CYP1A1 variants compared with individuals with GSTM1 or no CYP1A1 polymorphisms (46). Consequently, slow acetylators may not be able to compete with high activity of CYP1A2 for aromatic amines. In this study, the simultaneous analysis of several loci suggests that the combination of risk-elevating genotypes is more predictive of ALL risk than when they are taken independently. In other words, the etiology of childhood ALL cannot be explained by allelic variability at a single locus probably, because of the complexity of xenobiotics metabolism and the diversity of chemicals to which individuals are exposed. Acknowledgments We thank all of the patients and control subjects who participated in this study as well as the physicians and the clinical staff for their collaboration and Ulrike Brockstedt for critical reading of the manuscript. D. S. is a scholar of the Fonds de la Recherche en Santé du Québec. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. 561 562 Role of NAT1 and NAT2 Polymorphisms in Childhood ALL References 1. Dean, M. Cancer as a complex developmental disorder—nineteenth Cornelius P. Rhoads memorial award lecture. Cancer Res., 58: 5633–5636, 1998. 2. Champlin, R., and Gale, R. P. Acute lymphoblastic leukemia: recent advances in biology and therapy. Blood, 73: 2051, 1989. 3. Linet, M. S. (ed.), The Leukemias: Epidemiologic Aspects. New York: Oxford University Press, 1985. 4. Pendergrass, T. W. Epidemiology of acute lymphoblastic leukaemia. Semin. Oncol., 12: 80, 1985. 5. Greaves, M. F. Speculations on the cause of childhood acute lymphoblastic leukemia. Leukemia, 2: 120 –125, 1986. 6. Perera, F. P. Molecular epidemiology: insights into cancer susceptibility, risk assessment, and prevention. J. Natl. Cancer Inst., 88: 496 –509, 1996. 7. Whyatt, R. M., and Perera, F. P. Application of biologic markers to studies of environmental risks in children and the developing fetus. Environ. Health Perspect., 103: 105–110, 1995. 8. Perera, F. P., Jedrychowski, W., Rauh, V., and Whyatt, R. M. Molecular epidemiologic research on the effects of environmental pollutants on the fetus. Environ. Health Perspect., 107: 451– 460, 1999. 9. Perera, F. P. Environment and cancer: who are susceptible? Science (Washington DC), 278: 1068 –1073, 1997. 10. Krajinovic, M., Labuda, D., Richer, C., Karimi, S., and Sinnett, D. Susceptibility to childhood acute lymphoblastic leukemia: influence of CYP1A1, CYP2D6, GSTM1 and GSTT1 genetic polymorphisms. Blood, 93: 1496 –1501, 1999. 11. Deloménie, C., Grant, D. M., Krishnamoorthy, R., and Dupret, J. M. Les arylamine N-acétyltransferases: génétique à la susceptibilité aux xénobiotiques. Médecine/Sciences, 14: 27–36, 1998. 12. Meyer, U. A., and Zanger, U. M. Molecular mechanism of genetic polymorphism of drug metabolism. Ann. Rev. Pharmacol. Toxicol., 37: 269 –296, 1997. 13. Brockmoller, J., Cascorbi, I., Kerb, R., and Roots, I. Combined analysis of inherited polymorphisms in arylamine N-acetyltransferase 2, glutathione S-transferases M1 and T1, microsomal epoxide hydrolase, and cytochrome P450 enzymes as modulators of bladder cancer risk. Cancer Res., 56: 3915–3925, 1996. 14. Cascorbi, I., Brockmoller, J., Mrozikiewicz, M., Bauer, S., Loddenkemper, R., and Roots, I. Homozygous rapid arylamine N-acetyltransferase (NAT2) genotype as a susceptibility factor for lung cancer. Cancer Res., 56: 3961–3966, 1996. 15. Hughes, N. C., Janezic, S. A., McQueen, K. L., Jewett, M. A., Castranio, T., Bell, D. A., and Grant, D. M. Identification and characterization of variant alleles of human acetyltransferase NAT1 with defective functions using p-aminosalicylate as an in-vivo/in-vitro probe. Pharmacogenetics, 8: 55– 66, 1998. 16. Bell, D. A., Stephens, A., Castranio, T., Umbach, D. M., Watson, M., Deakin, M., Elder, J., Hendrickse, C., Duncan, H., and Strange, C. Polyadenylation polymorphism in the acetyltransferase 1 gene (NAT1) increases risk of colorectal cancer. Cancer Res., 55: 3537–3542, 1995. 17. Ambrosone, C. B., Freudenheim, J. L. Graham, S., Marshall, R. R., Vena, J. E., Brasure, J. R., Michalek, A. M., Laughlin, R., Nemoto, T., Gillenwater, K. A., Harrington, A. M., and Shields, P. G. Cigarette smoking, N-acetyltransferase 2 genetic polymorphisms, and breast cancer risk. J. Am. Med. Assoc., 276: 1494 –1501, 1996. 18. Drozdz, M., Gierek, T., Jendryczko, A., Pilch, J., and Piekarska, J. NAcetyltransferase phenotype of patients with cancer of the larynx. Neoplasma, 34: 481– 484, 1987. 19. Gonzales, M. V., Alvarez, V., Pello, M. F., Menendez, M. J., Suarez, C., and Coto, E. Genetic polymorphism of N-acetyltransferase-2, glutathione S-transferase-M1, and cytochromes P450IIE1 and P450IID6 in the susceptibility to head and neck cancer. J. Clin. Pathol., 4: 294 –298, 1998. 20. Mommsen, S., Barfod, N. M., and Aagaard, J. N-Acetyltransferase phenotypes in the urinary bladder carcinogenesis of a low-risk population. Carcinogenesis (Lond.), 6: 199 –201, 1985. 21. Risch, A., Wallace, D. M., Bathers, S., and Sim, E. Slow N-acetylation genotype is a susceptibility factor in occupational and smoking related bladder cancer. Hum. Mol. Genet., 4: 231–236, 1995. 22. Chen, J., Stampfer, M. J., Hough, H. L., Garcia-Closas, M., Willett, W. C., Hennekens, C. H., Kelsey, K. T., and Hunter, D. J. A prospective study of N-acetyltransferase genotype, red meat intake, and risk of colorectal cancer. Cancer Res., 58: 3307–3311, 1998. 23. Millikan, R. C., Pittman, G. S., Newman, B., Tse, C-K. J., Selmin, O., Rockhill, B., Savitz, D., Moorman, P. G., and Bell, D. A. Cigarette smoking, N-acetyltransferase 1 and 2 and breast cancer risk. Cancer Epidemiol. Biomarkers Prev., 7: 371–378, 1998. 24. Agundez, J. A., Ladero, J. M., Olivera, M., Abildua, R., Roman, J. M., and Benitez, J. Genetic analysis of the arylamine N-acetyltransferase polymorphism in breast cancer patients. Oncology, 52: 7–11, 1995. 25. Hirvonen, A., Pelin, K., Tammilehto, L., Karjalainen, A., Mattson, K., and Linnainmaa, K. Inherited GSTM1 and NAT2 defects as concurrent risk modifiers in asbestos-related human malignant mesothelioma. Cancer Res., 55: 2981–2983, 1995. 26. Labuda, D., Zietkiewicz, E., and Labuda, M. The genetic clock and the age of the founder effect in growing populations: a lesson from French Canadians and Ashkenazim. Am. J. Hum. Genet., 61: 768, 1997. 27. Bouchard, G., and De Braekeleer, M. (eds.) Histoire d’un génome. Québec: Presses de l’Université du Québec, 1990. 28. Baccichet, A., Qualman, S. K., and Sinnett, D. Allelic loss in childhood acute lymphoblastic leukemia. Leuk. Res., 21: 817– 823, 1997. 29. Labuda, D., Krajinovic, M., Richer, C., Skoll, A., Sinnett, H, Yotova, V., and Sinnett, D. Rapid detection of CYP1A1, CYP2D6, NAT variants by multiplexPCR and allele-specific oligonucleotide assay Anal. Biochem. 275: 84 –92: 1999. 30. Deitz, A. C., Doll, M. A., and Hein, D. W. A restriction fragment length polymorphism assay that differentiates human N-acetyltransferase-1 (NAT1) alleles. Anal. Biochem., 253: 219 –224, 1997. 31. Henning, S., Cascorbi, I., Münchow, B., Jahnke, V., and Roots, I. Association of arylamine N-acetyltransferases NAT1 and NAT2 genotypes to laryngeal cancer risk. Pharmacogenetics, 9: 103–111, 1999. 32. Taylor, J. A., Umbach, D. M., Stephens, E., Castranio, T., Paulson, D., Robertson, C., Mohler, J. L., and Bell, D. A. The role of N-acetylation polymorphisms in smoking-associated bladder cancer: evidence of a gene-gene-exposure three-way interaction. Cancer Res., 58: 3603–3610, 1998. 33. Badawi, A. F., Hirvonen, A., Bell, D. A., Lang, N. P., and Kadlubar, F. F., Role of aromatic amine acetyltransferases, NAT1 and NAT2, in carcinogen-DNA adduct formation in the human urinary bladder. Cancer Res., 55: 5230 –5237, 1995. 34. Probst-Hensch, N. M., Haile, R. W., Li, D. S., Sakanoto, G. T., Louie, A. D., Lin, B. K., Frankl, H. D., Lee, E. R., and Lin, H. J. Lack of association between the polyadenylation polymorphism in the NAT1 (acetyltransferase 1) gene and colorectal adenomas. Carcinogenesis (Lond.), 17: 2125–2129, 1996. 35. Grant, D., Hughes, N., Janezic, S., Goodfellow, G., Chen, H., Gaedigk, A., Yu, V., and Grewal, R. Human acetyltransferase polymorphisms. Mutat. Res., 376: 61–70, 1997. 36. Butcher, N. J., Ilett, K. F., and Minchin, R. F. Functional polymorphism of the human arylamine N-acetyltransferase type 1 gene caused by C190T and G560A mutations. Pharmacogenetics, 8: 67–72, 1998. 37. Neglia, J. P., and Robison, L. L. Epidemiology of the childhood acute leukemias. Pediatr. Clin. North Am., 35: 675– 692, 1988. 38. Linet, M. S., and Devesa, S. S. Descriptive epidemiology of childhood leukaemia. Br. J. Cancer, 63: 424 – 429, 1991. 39. Infante-Rivard, C., Labuda, D., Krajinovic, M., and Sinnett, D. Childhood leukemia: risk associated with exposure to pesticides and with gene polymorphisms. Epidemiology, 10: 481– 487, 1999. 40. Smelt, V. A., Mardon, H. J., and Sim, E. Placental expression of arylamine N-acetyltransferases: evidence for linkage disequilibrium between NAT1*10 and NAT2*4 alleles of the human arylamine N-acetyltransferase loci NAT1 and NAT2. Pharmacol. Toxicol., 83: 149 –157, 1998. 41. Derewlany, L. O., Knie, B., and Koren, G. Arylamine N-acetyltransferase activity of the human placenta. J. Pharmacol. Exp. Ther., 269: 756 –760, 1994. 42. Pacifici, G. M., Bencini, C., and Rane, A. Acetyltransferase in human development and tissue distribution. Pharmacology, 32: 283–291, 1986. 43. Cribb, A. E., Grant, D. M., Miller, M. A., and Spielberg, S. P. Expression of monomorphic arylamine N-acetyltransferase (NAT1) in human leukocytes. J. Pharmacol. Exp. Ther. 259: 1241–1246, 1991. 44. Grant, D. M. Molecular genetics of the N-acetyltransferases. Pharmacogenetics, 3: 45–50, 1993. 45. Hirvonen, A., Saarikoski, S. T., Linnainmaa, K., Koskinen, K., HusgafvelPursiainen, K., Mattson, K., and Vainio, H. Glutathione S-transferase and Nacetyltransferase genotypes and asbestos-associated pulmonary disorders. J. Natl. Cancer Inst., 88: 1853–1856, 1996. 46. MacLeod, S., Sinha, R., Kadlubar, F. F., and Lang, N. P. Polymorphisms of CYP1A1 and GSTM1 influence the in vivo function of CYP1A1. Mutat. Res., 376: 135–142, 1997. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research. Genetic Polymorphisms of N-Acetyltransferases 1 and 2 and Gene-Gene Interaction in the Susceptibility to Childhood Acute Lymphoblastic Leukemia Maja Krajinovic, Chantal Richer, Hugues Sinnett, et al. Cancer Epidemiol Biomarkers Prev 2000;9:557-562. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cebp.aacrjournals.org/content/9/6/557 This article cites 42 articles, 14 of which you can access for free at: http://cebp.aacrjournals.org/content/9/6/557.full#ref-list-1 This article has been cited by 8 HighWire-hosted articles. Access the articles at: http://cebp.aacrjournals.org/content/9/6/557.full#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cebp.aacrjournals.org on August 3, 2017. © 2000 American Association for Cancer Research.