Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
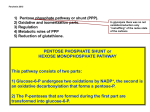
IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 * 16:34 Pagina 436 CHAPTER 17 Red blood cell enzyme defects Joan-Luis Vives Corrons IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 437 CHAPTER 17 • Red blood cell enzyme defects 1. Introduction The maturation process of erythroblasts involves the disappearance of virtually all the metabolic pathways specific to any other cell in the body, leaving only the components essential for maintaining the supply of energy and the defence against oxidising agents. The mature red blood cell (RBC), however, is optimally adapted to perform its most important function during its estimated 120-day lifespan in the circulation: the binding, transport and delivery of oxygen to all tissues. For this, the RBC requires three essential metabolic pathways: • Anaerobic glycolysis, which is the only source of energy (ATP production) for maintenance of cell structure and function • Anti-oxidant pathways necessary for the protection of RBC proteins against oxidation, through the synthesis of glutathione (GSH), and of haemoglobin against iron oxidation through the maintenance of iron in its functional, reduced, ferrous state (cytochrome b5 reductase) • Nucleotide metabolism for the maintenance of the purine and pyrimidine nucleotides. Moreover, erythrocytes possess a unique glycolytic bypass for the production of 2,3bisphosphoglycerate (2,3-BPG) a crucial metabolite in the regulation of haemoglobin affinity for oxygen. RBC enzymopathies have been described in all these metabolic pathways and almost all are associated with chronic haemolytic anaemia (CHA), with the exception of the enzymopathies of the pentose phosphate pathway and glutathione metabolism, which are associated with acute haemolytic crises only after exposure to oxidant substances. Some of the most rare enzyme defects are also expressed in other tissues. In general, however, the deficiency is more pronounced in RBCs, when compared with other cells, because of the long lifespan of the mature erythrocyte after the loss of protein synthesis. In general, these enzymopathies are associated, in addition to haemolytic anaemia (acute or chronic), with systemic (non-haematological) manifestations such as neuropathy (with or without mental retardation), muscular disease, recurrent infections and metabolic acidosis. By far the majority of red cell enzymopathies are hereditary in nature, although acquired deficiencies have also been described, mainly in malignant haematological disorders (1). Since the discovery of glucose 6-phosphate dehydrogenase (G6PD) deficiency in 1956, and pyruvate kinase (PK) deficiency in 1961, erythroenzymopathies associated with hereditary haemolytic anaemia have been extensively investigated (2-4). The mode of inheritance is autosomal recessive for almost all of erythroenzymopathies, but autosomal dominant for ADA overproduction and X-linked for G6PD and PGK deficiencies. In general, the genetic mutations that cause RBC enzyme defects are DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 437 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 438 associated with three different clinical phenotypes: a) haemolytic syndrome associated with either chronic anaemia (CHA) or acute haemolytic crises, b) permanent cyanosis with methaemoglobinaemia and c) increased RBC mass or erythrocytosis. 2. Erythroenzymopathies associated with hereditary haemolytic anaemia Erythroenzymopathies associated with CHA show common findings and generally differ greatly from case to case, even in one enzyme deficiency or within the same family. The degree of haemolysis is dependent on the severity of enzyme deficiency, a consequence of the properties of the mutant enzyme with regard to functional abnormalities, molecular instability, or both. In addition to the anaemia, other clinical findings are jaundice, due to increased indirect-reacting bilirubin, reticulocytosis, and splenomegaly. RBC morphology usually shows anisocytosis and polychromasia without specific changes, with the exception of echinocytosis, eccentrocytosis and basophilic stippling, which are frequently seen in PK, G6PD and P5’N deficiencies, respectively. The morphological abnormalities such as spherocytosis and elliptocytosis characteristic of some RBC membrane disorders, are not seen in erythroenzymopathies. This is the reason why erythroenzymopathies belong to the so-called hereditary non-spherocytic haemolytic anaemias (HNSHA). In most cases of G6PD deficiency, acute haemolytic anaemia (AHA) is caused either by the ingestion of oxidant drugs, such as salicylic acid or antimalarials (primaquine) or by infection. In some cases, haemolysis is seen after ingestion of fava beans (favism). Anaemia and/or neonatal jaundice are also common features. Although glutathione reductase (GR) deficiency would cause the same symptoms, and is associated with favism, it is extremely rare. Diagnosis: The most frequent human enzymopathy, G6PD deficiency, can be diagnosed by a simple screening test (5). However, when the patient suffers from a longstanding CHA either PK deficiency or another glycolytic enzymopathy, or an unstable haemoglobin should be suspected. The haemoglobin heat stability test is a simple and reliable screening test to detect unstable haemoglobins. However, a direct RBC enzyme activity assay is necessary to confirm the diagnosis of RBC enzyme deficiencies (6). In hereditary PK deficiency it is important to remove leukocytes from RBC suspension before making the red cell haemolysate because leukocytes possess 300 times more PK activity than RBCs. In addition, leukocytes have a different isoenzyme, which has normal activity in PK deficient cases. Currently, DNA diagnosis has become an available procedure for the study of almost all erythroenzymopathies. However, it is still not simple because there are often several or many mutations even in one enzyme deficiency. If the mutation(s) in a particular family is (are) already known, DNA diagnosis is relatively easy, and prenatal diagnosis is possible. Normal genomic DNA or cDNA for 438 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 439 CHAPTER 17 • Red blood cell enzyme defects most of the enzymes causing hereditary haemolytic anaemia has been isolated allowing a rapid advancing in the understanding of the molecular basis of RBC enzyme defects associated with hereditary haemolytic anaemia. PK and class I G6PD deficiencies comprise the two most common erythroenzymopathies associated with CHA followed by glucose-phosphate isomerase (GPI) and pyrimidine 5’- nucleotidase deficiencies. Very rare enzymopathies include the deficiencies of hexokinase (HK) adenylate kinase (AK), phosphofructokinase (PFK), phosphoglycerate kinase (PGK), triose-phosphate isomerase (TPI), glutathione peroxidase (GSH-Px), glutathione reductase (GR), glutathione synthetase (GS), gamma-glutamylcysteine synthetase (GGCS) and the overproduction of adenosine deaminase (ADA). Considered together, all these enzymopathies account for less than 10 percent of all the patients with enzyme deficiency associated with CHA. Moreover in some cases, the CHA is associated with severe clinical manifestations like neuropathy (TPI, PGK, GGCS, GS and AK) and/or myopathy (PFK, PGK, AK) or frequent infections (TPI). Almost all these enzymes are located in the two main metabolic pathways of RBC: anaerobic glycolysis and anti-oxidative metabolism (Figure 1). Figure 1: RBC metabolism. Anaerobic glycolysis and antioxidant pathways GSH NADP Glucose CO2 ATP ADP HK G6P 6PG G6PD GPI Glutathione peroxidase Glutathione reductase NADPH GSSG 6PGD Ru5P F6P ATP ADP PFK H2O 2H + GSH GSH ANTIOXIDANT METABOLISM FDP Aldolase H2O2 ADP ATP Glycine Glutathione-synthetase γ-glutamyl-cysteine DHAP G3P G3PD ANAEROBIC GLYCOLYSIS Pi NAD NADH 1,3-BPG Mutase 2,3-BPG Phosphatase 3-PG Mutase GCS ADP ATP TPI Cysteine Glutamic acid PGK ADP ATP ATP ADP 2-PG PEP Enolase PK NADH NAD Pyruvate Lactate Lactate dehydrogenase DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 439 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 440 General aspects of treatment and prevention: There is no treatment for hereditary RBC enzyme deficiencies. Non-specific supportive measures such as red cell transfusions provide the only currently accepted approach. Splenectomy is not curative but is frequently of value, especially in infants and young children with severe disease. Haemoglobin concentration often increases by 1-3 g/dL, reducing or even eliminating transfusion requirements. Phototherapy is recommended in case of neonatal hyperbilirubinaemia, but exchange transfusion may become necessary in severe cases. G6PD-deficient patients should be advised to avoid potentially haemolytic drugs or, in case of indispensable drugs, to ensure that they are used in sub-haemolytic doses. 2.1 Glucose-6-phosphate dehydrogenase (G6PD) deficiency G6PD catalyses the first step in the hexose monophosphate shunt which is necessary for producing NADPH. NADPH in turn is required for the maintenance of reduced glutathione (GSH), a tripeptide that protects the RBC from oxidative damage (Figure 1). G6PD is distributed in all cells and the active enzyme is a monomer of 515 aminoacids, with a molecular weight of about 59 kDa. The enzyme is active as a tetramer or dimmer, depending on pH (7). 2.1.1 Clinical manifestations G6PD deficiency (OMIM 305 900) is the most common known enzymopathy and it is estimated to affect 400 million people worldwide. G6PD deficiency is X-linked and caused by different mutations in the G6PD gene, resulting in protein variants with different levels of enzyme activity that are associated with a wide range of biochemical and clinical phenotypes. Major clinical manifestations are AHA after ingestion of drug or fava beansand/or neonatal jaundice. A very small proportion of G6PD-deficient individuals have a CHA and this has been defined by World Health Organisation (WHO) classification as Class I G6PD-deficiency (see below). Favism presents as an acute haemolytic crisis, usually after 24 to 72 h of ingestion of the beans (or contact with fava bean products) with severe anaenia (sometimes requiring blood transfusion) and haemoglobinuria (dark urine), which is more severe than that caused by drugs or infection, although bilirubin concentration is slightly lower. In the acute stages of favism a number of characteristic changes in RBC morphology are frequently observed, including eccentrocytosis (Figure 2A) or bite-cells (Figure 2B). The anaemia worsens until days 7–8 and after drug cessation, haemoglobin concentrations recover after approximately 12 days. Heinz bodies (denatured haemoglobin precipitates) in peripheral red blood cells, detected by methyl violet staining, are a typical finding (Figure 3). Favism can develop after ingestion of dried or frozen beans, but is particularly likely to occur after eating fresh beans; the disorder is most frequent in the period when beans are harvested. Although favism was first noted to be common in Mediterranean countries, it was 440 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 441 CHAPTER 17 • Red blood cell enzyme defects Figure 2: MGG stained blood smear from a patient with G6PD deficiency and acute haemolytic crisis of favism A B A. Several erythrocytes with a ragged appearing, poorly haemoglobinised fringe of cytoplasm along one side of the cell can be seen. This appearance (eccentrocytes or hemi-ghosts) results from an apposition and adherence of opposing inner surfaces of the cell membrane with a variable exclusion of haemoglobinised cytoplasm to an "eccentric" location in the cell. B. Several bite-cells or red blood cells (RBCs) from which, one or more semicircular portions have been removed from the cell margin. subsequently also observed in other geographical areas such as Middle East, the Far East, and North Africa. Most patients who develop favism have the Mediterranean variant of G6PD deficiency but favism is also very common with the G6PD A-variant in populations where the growth and consumption of fava beans is widespread. Drugs capable of producing an acute haemolytic crisis in G6PD deficiency can Figure 3: Methyl violet stained RBCs be classified into two main groups: a) from a patient with G6PD deficiency drugs that have been shown to be showing a characteristic inclusion of capable of producing clinically significant denatured haemoglobin (Heinz bodies) haemolytic anaemia in doses that are normally used (Table 1) and b) drugs that have been shown to have a minor effect on red cell survival when given in large doses, such as aspirin, but which can be given safely to most patients with G6PD deficiency (Table 2). Patients with CHA due to G6PD deficiency have, in general, a history of severe neonatal jaundice, chronic anaemia exacerbated by oxidative stress, blood DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 441 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 442 Table 1: Drugs and chemicals which should be avoided by all persons with G6PD deficiency Acetanilid Phenazopyridine (Pyridium) Diaminodiphenyl sulfone Phenylhydrazine Furazolidone (Furoxone) Primaquine Glibenclamide Sulfacetamide Henna (Lawsone) Sulfanilamide Isobutyl nitrite Sulfapyridine Methylene Blue Thiazolesulfone Naphthalene Trinitrotoluene (TNT) Niridazole (Ambilhar) Urate oxidase Nitrofurantoin (Furadantin) Beutler E. Glucose-6-phosphate dehydrogenase deficiency: A historical perspective. Blood 2008; 111: 16-24 Table 2: Drugs that probably can be safely given in normal therapeutic doses to G6PD-deficient patients without haemolytic anaemia Acetaminophen (paracetamol, Tylenol, Tralgon, hydroxyacetanilide) Acetophenetidin (phenacetin) Acetylsalicylic acid (aspirin) Aminopyrine (Pyramidon, aminopyrine) Antazoline (Antistine) Antipyrine Ascorbic acid (vitamin C) Benzhexol (Artane) Chloramphenicol Chlorguanidine (Proguanil, Paludrine) Chloroquine Colchicine Diphenyldramine (Benadryl) Isoniazid L-Dopa Menadione sodium bisulfite (Hykinone) p-Aminobenzoic acid p-Aminosalicylic acid Phenylbutazone Phenytoin Probenecid (Benemid) Procainamide hydrochloride (Pronestyl) Pyrimethamine (Daraprim) Quinine Streptomycin Sulfacytine Sulfadiazine Sulfaguanidine Sulfamerazine Sulfamethoxazole (Gantanol) Sulfamethoxypyridazine (Kynex) Sulfisoxazole (Gantrisin) Tiaprofenic acid Trimethoprim Tripelennamine (Pyribenzamine) Vitamin K Beutler E. Glucose-6-phosphate dehydrogenase deficiency: A historical perspective. Blood 2008; 111: 16-24 442 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 443 CHAPTER 17 • Red blood cell enzyme defects transfusion requirement, splenomegaly and gallstones at early age. Chronic haemolysis attributable to G6PD deficiency is sometimes exacerbated by co-inherited (and unrelated) genetic erythrocyte alterations, such as membrane defects, thalassaemia, glucose6-phosphate isomerase deficiency, pyruvate kinase deficiency and congenital dyserythropoietic anaemia. Unexpectedly high amounts of non-conjugated bilirubin can be seen in the co-inheritance of G6PD deficiency and Gilbert’s syndrome (8). 2.1.2 Epidemiology and molecular studies The highest frequencies of G6PD deficiency have a global distribution that is very similar to that of malaria (Africa, the Mediterranean region, Middle East and sub tropical Asia), lending support to the so-called malaria protection hypothesis. However as a result of migration, the disorder is also found in North and South America and in northern European countries. In 1967, an expert committee of the WHO proposed standard biochemical procedures for characterising variants, such as enzyme activity, Km for glucose 6-phosphate, heat stability and electrophoretic pattern (10). After this, the WHO introduced a classification of G6PD variants into five classes according to the severity of the clinical phenotype (Table 3). Class I: severe enzyme deficiency with chronic nonspherocytic haemolytic anaemia; Class II: severe enzyme deficiency (less than 10% of normal); Class III: moderate-to-mild enzyme deficiency (10%-60% of normal); Class IV: mild or no enzyme deficiency (60%-100% of normal); and Class V: increased enzyme activity more than twice normal. There appeared to be 2 types of mutations among Africans: G6PD A, a normally active enzyme with rapid electrophoretic mobility, and G6PD A–, an enzyme with the same mobility as G6PD A, but with diminished activity. The enzyme variant found in Mediterranean subjects was designated as G6PD B– but Table 3: WHO classification of G6PD deficient variants CLASS I Severe G6PD deficiency (< 1%) associated with chronic haemolytic anaemia (CHA) • Very rare variants (sporadic) CLASS II Severe G6PD deficiency (1-5%) associated with acute haemolytic anaemia (AHA) • G6PD Mediterranean variants (polymorphic) • G6PD Asiatic variants (polymorphic) CLASS III Moderate to severe G6PD deficiency (5-20%) associated with AHA • G6PD A- CLASS IV Normal G6PD activity (100%) • G6PD B+ • G6PD A+ CLASS V Hyperactive G6PD activity (> 150%) • G6PD Hecktoen DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 443 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 444 subsequently renamed G6PD Mediterranean. G6PD Mediterranean variant is by no means the only mutant enzyme found in the Mediterranean region; other enzyme variants such as G6PD Seattle are common as well. In Asia even more heterogeneity was found. These standard methods of WHO for differentiating variants from one another were used by most investigators and until 1990, about 450 apparently different variants were described. These methods, however, were not precise, and there was obviously a professional advantage for an investigator to describe a new variant rather than rediscover an old one. Thus, minor differences, due to technical variation, may be the basis of describing the same variant under several different names. In this situation, it has become increasingly difficult to decide whether a new variant actually differs from all those that had been described before. After isolation of G6PD cDNA, the primary structure of the enzyme was determined, allowing the understanding of the polymorphisms of G6PD gene in a much more precise fashion than had been possible when differentiation of variants depended on enzyme kinetics, heat stability, and electrophoretic mobility. Accordingly, it was possible to show quite rapidly that Yoshida’s deduction that G6PD A was a result of a substitution of aspartic acid for asparagine had been quite correct. Interestingly, it became apparent that G6PD A– is not a single variant but a group of variants that have in common the same mutation as G6PD A+, together with one additional mutation, usually c.202 GA (V68M) (11). The current database of some 160 mutants so far studied indicate that G6PD gene mutations are due, with a few exceptions, to single missense point mutations, entailing single amino acid replacements in the G6PD protein. The exceptions are small deletions (of one to eight amino acids) found in very few individuals. In most cases these mutations cause G6PD deficiency by decreasing the in vivo stability of the protein producing a great acceleration of G6PD activity decrease with red cell aging. In some variants the amino acid replacement can also affect the catalytic function of the enzyme (for instance, a decreased affinity of G6PD for the substrate) leading to a much more severe clinical phenotype such as chronic haemolytic anaemia even in the absence of any oxidant challenge (WHO Class 1 variants). Recently it has been demonstrated that the cluster of mutations around exons 10 and 11 designates the subunit interface, which interacts with other important residues located elsewhere but which is brought close to this domain by protein folding. Stability of the active quaternary structure is crucial for normal G6PD activity (11). 2.2 Pyruvate kinase (PK) deficiency PK catalyzes the irreversible transfer of a phosphoryl group from phosphoenolpyruvate (PEP) to ADP, thus yielding pyruvate and ATP; it is a regulatory key enzyme of the glycolytic pathway (Figure 1). There are four isozymes of PK: PK-M1, PK-M2, PK-L, and PK-R. The PK-M1 isoenzyme is expressed in skeletal muscle, heart, and brain, and it 444 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 445 CHAPTER 17 • Red blood cell enzyme defects is the only isoenzyme that is not subject to allosterically regulation. The PK-M2 isenozyme is expressed in early foetal tissues, but also in most adult tissues, including leucocytes and platelets. PK-R is exclusively expressed in RBCs, whereas PK-L is predominantly expressed in the liver (12). The PK-R and PK-L subunits are both transcribed from the single gene PK-LR by the use of alternative promoters (Figure 4). The active PK-R enzyme is a tetramer of four identical subunits and each subunit is divided into 4 domains (Figure 5). The enzyme is allosterically activated by its Figure 4: Genetic mechanism of liver PK (PK-L) and red blood cell PK (PK-R) isozymes synthesis by selective transcription from a single gene PK-LR using alternative promoters PK-R ISOZYME (RBCs) 1 3 4 5 6 7 8 9 10 11 12 3 5' 2 3 4 5 6 7 8 9 10 11 12 PK-L ISOZYME (Liver) NO CODING SEQUENCE EXONS CODING SEQUENCE INTRONS Figure 5: PK-LR monomer. Molecular model based on cat muscle PK enzyme B DOMAIN Active Centre A DOMAIN FDP Binding site N DOMAIN C DOMAIN DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 445 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 446 substrate fructose-bis-phosphate (FBP) and negatively regulated by ATP. Furthermore, PK has an absolute requirement for cations Mg2+ and Ca+. 2.2.1 Clinical manifestations PK deficiency (OMIM 266 200) is the most common enzymopathy associated with CHA, and about 300 patients have been reported so far. CHA usually occurs in compound heterozygotes for two different mutant alleles and in homozygotes, where the increased 2,3-BPG levels ameliorate the anaemia by lowering the oxygen-affinity of haemoglobin. Phenotypically, the clinical picture varies from severe haemolysis causing neonatal death, to a well-compensated haemolytic anaemia and only very rare cases can present with hydrops foetalis. 2.2.2 Epidemiology and molecular studies The estimated prevalence of PK deficiency is 51 cases (i.e., homozygous or compound heterozygous patients) per million in the white population. In 1979, recommended procedures for the biochemical characterisation of PK variants were issued by a subcommittee of the International Committee for Standardisation in Haematology (13). More recently mutations of PK gene leading to CHA have been extensively studied using molecular biology procedures. By the year 2008, more than 180 gene mutations in PKLR had been reported to be associated with PK deficiency (14). Most of these mutations (70%) are the missense mutants c.1456CÆT (Arg486Trp), c.1529GÆA (Arg510Gln), c.994GÆA (Gly332Ser), and the nonsense mutant c.721GÆT (Glu241stop). They affect conserved residues in structurally and functionally important domains of PK. A clear geographical distribution has been observed among the most frequent mutations of PK enzyme (Table 4). 2.3 Glucose phosphate isomerase (GPI) deficiency GPI deficiency (OMIM 172 400) is the second most common erythroenzymopathy of Table 4: Geographical distribution of the most frequent PK-LR gene mutations leading to chronic haemolytic anaemia (CHA) 446 Central Europe and North-America G1529 A (Arg510Glu) C1594 T (Arg 532Trp) G 994 A (Gly332Ser) Southern Europe C1456T (Arg486Trp) Fatal mutations (CHA in heterozygotes) G409A (Ala137Thr) (South Europe) G1091A (Gly364Asp) (Northern Europe) G721T (Glu241stop) (Worldwide) THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 447 CHAPTER 17 • Red blood cell enzyme defects glycolytic enzymes after PK deficiency, and approximately 50 different cases have been described to date. GPI deficiency is an autosomal recessive genetic disorder associated with mild to severe CHA in homozygotes or compound heterozygotes. In a very few cases, GPI deficiency is associated with neurological impairment and granulocyte dysfunction. Twenty-nine mutations have been detected in GPI, 24 of which were missense mutations, 3 were nonsense mutations, and 2 were mutations that affected splice sites. Mapping of these mutations to the crystal structure of human GPI has provided insight into the molecular mechanisms causing haemolytic anaemia in this disorder. In accordance with the 3-dimensional structure, mutations can be categorised into 3 distinct groups that affect the overall structure, the dimer interface, and the active site. Nearly all GPI mutants described are heat unstable, whereas kinetic properties are more or less unaffected (15). 2.4 Pyrimidine 5’ nucleotidase (P5’N-1) deficiency P5’N-1, uridine monophosphate hydrolase-1 (UMPH-1) or cytosolic 5:nucleosidase II (cN-III) is an enzyme which major role is in the catabolism of the pyrimidine nucleotides, uridine monophosphate (UMP) and cytidine monophosphate (CMP), mainly resulting from RNA degradation during erythrocyte maturation. P5’N-1 deficiency (OMIM 606 224) is an autosomal recessive disorder characterised by CHA with marked reticulocytosis and increased concentrations of pyrimidine nucleotides within mature erythrocytes A characteristic RBC morphological abnormality is a heavy basophilic stippling, and its observation is very helpful for P5’N diagnosis (Figure 6). Since the first description of P5’N in 1974, about one hundred P5’N-deficient patients have been reported worldwide Figure 6: Severe basophilic stipling although it is possible that a larger spontaneous aggregation of ribosomal number have been not detected. It RNA in the cytoplasm of erythrocytes has been suggested that P5’N-1 in a case of P5’N-1 deficiency deficiency is the third most common RBC enzymopathy, after G6PD and PK deficiencies, although this is not the case for the different geographical areas (16). P5’N-1 deficiency can also be acquired as a result of lead poisoning or oxidative stress. Lead is a powerful inhibitor of P5’N and determination of lead levels should be included whenever the constellation of haemolytic anaemia, P5’N deficiency, and basophilic stippling is DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 447 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 448 found. Lead-induced acquired P5’N deficiency is treatable, unlike the congenital deficiency for which no therapy is available (16). It is worth mentioning several clinical reports of severe haemolytic anaemia in patients with co-inheritance of P5’N deficiency and the thalassaemic haemoglobin Hb E. This provides a further support to the idea that P5’N is particularly susceptible to oxidative damage resulting from the instability of haemoglobin in thalassaemic syndromes (17). 2.5 Enzymopathies associated with haemolytic anaemia and systemic disease Some very rare enzymopathies, in addition to causing acute or chronic haemolytic anaemia, are associated with systemic (non-haematological) manifestations such as neuropathy with or without mental retardation, myopathy, recurrent infections and metabolic acidosis (Table 5). Understanding of the clinical behaviour of these enzymopathies requires a deep knowledge of their genetics, biochemical properties and the structural consequences of responsible mutations on the enzyme molecule. This phenotype, however, is not only depending on the molecular properties of mutant proteins but also on a complex interplay of physiologic, environmental, and other genetic factors (polymorphisms posttranslational modifications, epigenetic modification, etc). Moreover, aberrant enzymatic function in non-erythroid tissues may also influence the clinical outcome of hereditary enzymopathies. Their study is also fostered by the growing recognition that several glycolytic enzymes have diverse, non-enzymatic functions (18), including modification of cell motility, control Table 5: Erythroenzymopathies associated with haemolytic anaemia and systemic disease 448 1 Phosphofructokinase (PFK)deficiency - Muscle disease (glycogenosis Type VII) (OMIM 171 850) 2 Triose Phosphate Isomerase (TPI) deficiency - Progressive neurologic disorder (Spasticity) - Recurrent infections (OMIM 190 450) 3 Phosphoglycerate kinase (PGK) deficiency - Neuromuscular manifestations (rhabdomyolysis) (OMIM 300 653) 4 Adenylate kinase deficiency (AK) deficiency - Psychomotor impairment (mental retardation) (OMIM 103 000) 5 Glutathione synthetase (GS) deficiency (OMIM 266 130) - Metabolic acidosis (5-oxoprolinuria) - Neurological symptoms (psychomotor retardation and ataxia) - Recurrent bacterial infections 6 Gamma-glutamylcysteine synthetase (GGS) deficiency - Metabolic acidosis (5-oxoprolinuria) - Neurological symptoms (psychomotor retardation and ataxia) - Recurrent bacterial infections THE HANDBOOK 2009 EDITION (OMIM 230 540) IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 449 CHAPTER 17 • Red blood cell enzyme defects of apoptosis and regulation of oncogenes. In addition these have important roles in the regulation of the transcription of an array of genes by multiple mechanisms. Accordingly it remains to be determined whether the non-erythroid clinical phenotypes of mutations of some red cell enzyme genes can be explained by their newly discovered non-glycolytic roles. Hence, future research in RBC enzymopathies should take all these new factors and phenotypic modifiers into account when considering the relationship between genotype and phenotype correlation. 3. Erythroenzymopathies associated with methaemoglobinaemia Hereditary methaemoglobinaemia can be divided into two forms. One is due to Hb M, which has autosomal dominant inheritance, and the other is due to an enzyme abnormality of the NADH-dependent methaemoglobin reductase system. The later has an autosomal recessive inheritance and is due to cytochrome b5 reductase (b5R) deficiency (19). The two disorders can be diagnosed by the absorption spectrum of a clear, stroma-free haemolysate. Methaemoglobinaemia due to b5R deficiency (OMIM 250 800) can be classified into two main groups with drastically different clinical manifestations. In one group, patients not unwell and the only clinical manifestation is cyanosis (hereditary b5R deficiency type I), which can be treated with the administration of methylene blue. In the other group, in addition to cyanosis there is a much more severe clinical syndrome characterised by microcephaly, opisthotonos, retarded growth and progressive neurological impairement leading to generalysed hypertonia, mental retardation and death before puberty (hereditary b5R deficiency type II). Unfortunatelly this clinical form of hereditary b5R deficiency has no treatment but it is very rare. 3.1 Hereditary b5R deficiency type I This is found worldwide, but it is endemic in some populations such as the Athabascan Indians, Navajo Indians, and Yakutsk natives of Siberia. In other ethnic and racial groups, the defect occurs sporadically. Homozygotes or compound heterozygotes have methaemoglobin concentrations of 10 to 35% and appear cyanotic but are usually asymptomatic even with levels up to 40%. Life expectancy is not shortened, and pregnancies occur normally. Significant compensatory elevation of haemoglobin concentration is sometimes observed (erythrocytosis). The b5R activity of the erythrocytes of heterozygotes is approximately 50% of normal. Although this activity level is sufficient to maintain normal methaemoglobin levels during normal conditions, oxidant stress can overwhelm the erythrocyte’s capacity to reduce methaemoglobin and produce acute symptomatic methaemoglobinaemia. DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 449 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 450 The cyanosis can be effectively treated with methylene blue or ascorbic acid and it is only indicated for cosmetic reasons, because it has no effect on the neurological abnormalities. 3.2 Hereditary b5R deficiency type II This is less frequent than the former, and patient’s life expectancy is significantly shortened due to the neurological complications which are very severe. Enzyme deficiency is generalised and manifested by a nearly total lack of microsomal cytochrome b5 reductase in all the cells. Amniotic cells contain easily measurable b5R activity; thus, prenatal diagnosis of homozygous b5R deficiency is feasible. From molecular point of view, in hereditary b5R deficiency type I the enzyme deficiency is limited to the RBCs and the abnormal gene product is produced at a normal rate but is unstable. As a result in b5R deficiency type I, only mature RBCs, which cannot synthesise proteins, are affected. By contrast in b5R deficiency type II, mutations cause underproduction of the enzyme or an enzyme with decreased enzymatic activity with a generalised enzyme deficiency in all cell types. In summary, congenital methaemoglobinaemias, with the exception of type II congenital methaemoglobinaemias, are asymptomatic and only of cosmetic concern to some. In contrast, a comparable level of methaemoglobin in patients with acquired methaemoglobinaemia is symptomatic due to severe acute tissue hypoxia which may be life-threatening. 4. Erythroenzymopathies associated with erythrocytosis Congenital erythrocytosis can result from a extremely rare RBC enzymopathy due to bisphosphoglycerate mutase (BPGM) deficiency (OMIM 222 800). Only two affected families have been described so far. In both cases patients had a complete deficiency of erythrocyte BPGM, increased ATP levels, ruddy cyanosis, high haemoglobin concentration (190g/L) and no evidence of haemolysis (20). BPGM is a tri-functional enzyme whose main function is to synthesise 2,3-diphosphogycerate (2,3-BPG). In the erythrocyte, 2,3-BPG is synthesised and dephosphorylated in a special bypass called “Rapoport-Luebering shunt” (Figure 1). This glycolytic bypass is unique to mammalian red blood cells and represents an important physiologic means for regulating the oxygen affinity of haemoglobin, which is also influenced by changes of blood pH. 2,3-BPG is synthesised by BPGM, an enzyme that also displays two other activities, a phosphatase activity that degrades 2,3-BPG and a minor mutase activity identical to that of glycolytic phosphoglycerate mutase. Quantitatively, 2,3-BPG is the major glycolytic intermediate. Increased 2,3-BPG levels result in a decrease of affinity of haemoglobin for oxygenwhich is more readily transferred to tissue. The anaemia is thus ameliorated and exercise tolerance is 450 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 451 CHAPTER 17 • Red blood cell enzyme defects improved. This beneficial effect is absent in the distal glycolytic enzyme defects HK, GPI, PFK, aldolase, and TPI deficiency that all cause a decrease in 2,3-BPG levels. Several of the distal glycolytic enzymes (i.e., HK and PFK) are inhibited by 2,3-BPG. References 1. Kahn A. Abnormalities of erythrocyte enzymes in dyserythropoiesis and malignancies. Clin Haematol 1981; 10: 123-138. 2. Tanaka KR, Paglia DE. Pyruvate kinase and other enzymopathies of the erythrocyte. In: Scriver CR, Beaudet AL, Sly WS, Valle D (eds): The Metabolic and Molecular Basis of Inherited Disease (ed 7). New York, NY, McGraw-Hill, 1995, p. 3485. 3. Eber SW. Disorders of erythrocyte glycolysis and nucleotide metabolism. In: Handin RI, Lux SE, Stossel TP, eds. Blood Principles and Practice of Hematology. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003: 1887-1914. 4. Prchal JT, Gregg XT. Red cell enzymopathies. In: Hoffman R, Benz E, eds. Hematology: Basic Principles and Practice, 4th ed. 2005: 653–659. 5. Beutler E. Red Cell Metabolism. A Manual of Biochemical Methods. 3rd Ed. Orlando, FL, Grune & Stratton, 1984. 6. Lewis SM, Bain BJ, Bates I. Dacie and Lewis Practical Haematology. 10th Ed. Curchill Livingstone, 2006. 7. Naylor CE, Rowland P, Basak K, et al. Glucose 6-phosphate dehydrogenase mutations causing enzyme deficiency in a model of the tertiary structure of the human enzyme. Blood 1996; 87: 2974-2982. 8. Luzzatto L, Metha A, Vulliamy T. Glucose 6-phosphate dehydrogenase deficiency. In: Scriver CR, Beaudet AL, Sly WS, et al, eds. The metabolic and molecular basis of inherited disease, 8th ed. Columbus: McGraw- Hill, 2001: 4517-4553. 9. Kaplan M, Hammerman C. Glucose-6-phosphate dehydrogenase deficiency: A hidden risk for kernicterus. Semin Perinatol 2004; 28: 356–364. 10. Betke K, Beutler E, Brewer GJ, et al. Standardization of procedures for the study of glucose6-phosphate dehydrogenase. Report of a WHO scientific group. WHO Tech Rep Ser No. 366, 1967. 11. Hirono A, Beutler E. Molecular cloning and nucleotide sequence of cDNA for human glucose-6-phosphate dehydrogenase variant A(–). Proc Natl Acad Sci USA 1988; 85: 3951–3954. 12. Kanno H, Fujii H, Miwa S. Structural analysis of human pyruvate kinase L-gene and identification of the promoter activity in erythroid cells. Biochem Biophys Res Commun 1992; 188: 516-523. 13. Miwa S, Boivin P, Blume KG, et al. Recommended methods for the characterization of red cell pyruvate kinase variants. Br J Haematol 1979; 43: 275. 14. Zanella A, Fermo E, Bianchi P, et al. Pyruvate kinase deficiency: The genotype-phenotype association. Blood Rev 2007; 21: 217-231. 15. Repiso A, Oliva B, Vives Corrons JL, et al. Red cell glucose phosphate isomerase (GPI): A molecular study of three novel mutations associated with hereditary nonspherocytic DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 451 IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 452 hemolytic anemia. Hum Mut 2006, #937, online. 16. Vives-Corrons JL. Chronic non-spherocytic haemolytic anaemia due to congenital pyrimidine 5’nucleotidase deficiency: 25 years later, Bailliere’s Best Pract Res Clin Haematol 2000; 13: 103–118. 17. Zanella A, Bianchi P, Fermo E, Valentini G. Hereditary pyrimidine 5‘-nucleotidase deficiency: From genetics to clinical manifestations. Br J Haematol 2006; 133: 113–123. 18. Kim J, Dang CV. Multifaceted roles of glycolytic enzymes. Trends Biochem Sci 2005; 30: 142–150. 19. Jaffe ER, Hultquist DE. Cytochrome b5 reductase defi ciency and enzymopenic hereditary methemoglobinemia. In: Scriver CR, Beaudet AL, Sly WS, Valle D (eds), The Metabolic and Molecular Basis of Inherited Disease (ed 7), New York, NY,McGraw-Hill, 1995, p. 3399. 20. Hoyer JD, Allen SL, Beutler E, et al. Erythrocytosis due to bisphosphoglycerate mutase deficiency with concurrent glucose-6-phosphate dehydrogenase (G-6-PD) deficiency. Am J Hematol 2004; 75: 205-208. Multiple Choice Questionnaire To find the correct answer, go to http://www.esh.org/iron-handbook2009answers.htm 1. The most frequent RBC enzymopathy associated with chronic haemolytic anaemia is: a) Pyruvate kinase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . b) Glucose-6-phosphate dehydrogenase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . c) Pyrimidine 5' nucleotidase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . d) Reduced glutathione deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Acute haemolysis after fava beans ingestion is a usual clinical manifestation of: a) Glutathione synthetase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . b) Pyruvate kinase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . c) Glutathione reductase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . d) Pyrimidine 5' nucleotidase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3. Diagnosis of pyruvate kinase deficiency requires the measurement of enzyme activity on: a) Whole blood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . b) Leukocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 452 THE HANDBOOK 2009 EDITION IRON2009_CAP.17(436-453):EBMT2008 4-12-2009 16:34 Pagina 453 CHAPTER 17 • Red blood cell enzyme defects c) Leukocyte-free haemolysates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . d) Blood serum or plasma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4. One of the following RBC enzymopathies can be associated with progressive neuropathy: a) Glucose-6-phosphate dehydrogenase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . b) Glucose-phosphate isomerase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . c) Triose phosphate isomerase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . d) Aldolase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. Basophilic stippling is a RBC abnormality that can be frequently present in: a) Oxidative metabolism impairment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . b) Increased reduced glutathione (GSH) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . c) Adenosine deaminase (ADA) hyperactivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . d) Pyrimidine 5' nucleotidase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DISORDERS OF ERYTHROPOIESIS, ERYTHROCYTES AND IRON METABOLISM 453