Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
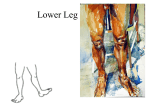
The Foot, Ankle, & Lower Leg Injuries • Foot Anatomy – Bones • 26 bones – 7 tarsal-talus, calcaneous, navicular, cuboid, 3 cuneiforms – 5 metatarsal – 14 phalanges- 1st toe has 2; toes 2-5 has 3 – Arches • Anterior metatarsal - shaped by the distal heads of the MT; stretches across the 1st to the 5th • Transverse - extends across the transverse tarsal bones; forms a half dome; gives protection to soft tissue and increases the foot’s mobility • Medial longitudinal – originates along the medial border of the calcaneus and extends to the • • distal head of the 1st MT; supports the medial arch Lateral longitudinal – outer aspect of foot & follows the same pattern as the medial longitudinal; much lower & less flexible than the medial longitudinal Muscles and Movements – Dorsiflexion • Tibialis anterior • Extensor digitorium longus • Extensor hallicus longus • Peroneus tertius – Plantarflexion • Peroneus longus/brevis • Tibialis posterior • Flexor digitorium longus • Flexor hallicus longus – Inversion, adduction, and supination – • • Tibialis posterior • Flexor digitorium longus • Flexor hallicus longus • Tibialis anterior • Extensor hallicus longus Eversion, abduction, and pronation • Peroneus longus/brevis • Peroneus tertius • Extensor digitorium longus Foot assessment – History • Type of surface for training? • Type of footwear worn? • Is discomfort increased when footwear is worn? – Observation • Is athlete favoring the foot, walking with a limp, or unable to bear weight? • Does the foot change color weight bearing vs. non weight bearing? • Pes planus (flatfoot) or pes cavus (high arch)? • Toe abnormalities? • Is the foot well-aligned? Does it maintain its shape on weight bearing? Shoe patterns? – • Palpation • Medial, lateral, dorsal, and plantar aspects of foot • Pulses – Tibialis posterior-behind medial malleolus – Dorsal pedal-midpoint between medial & lateral malleolus to the proximal end of the 1 st intermetatarsal space Recognition and management of specific injuries – Heel bruise • Cause – sudden stop & go; sudden horizontal & vertical movement • Signs – severe pain in heel; unable to bear weight • Care – ice; rest; NWB for 24 hours; heel cup; doughnut – Plantar fascitis • Cause – leg length discrepancy; inflexibility of longitudinal arch; Gastroc/soleus tightness; shoes without arch support • Signs – pain worse in morning; pain with long sitting periods, but lessens after first few steps • Care – vigorous heel cord stretching; PF stretching; heel cup; arch tape; orthotics – Fractures of the metatarsal – • Cause – direct force • Signs of injury – swelling; pain; deformity; pt. tenderness • Care – rest; immobilization Jones fracture • Cause – neck of 5th MT-overuse; acute inversion; high velocity rotation • Signs – sharp pain of lateral border of foot; “pop”; Care – cast 6-8 weeks; longer with surgery; long rehab due to poor blood supply – Bunions – • Cause – painful deformity of head of 1st MT; shoes-pointed, too narrow, to short, high heels • Signs – tenderness, swelling, enlargement with calcification of head of 1 st MT • Care – shoes; doughnut; orthotics Blisters • Cause – shearing forces acting on skin • Signs – fluid-clear, bloody, or infected • Care – petroleum jelly; doughnut; second skin; drain; antibiotic ointment; wearing socks with no folds/wrinkles – Morton’s Neuroma – • Cause – mass that occurs about the nerve sheath of the common plantar nerve; collapse of the transverse arch of the foot; excessive foot pronation • Signs – burning paresthesia; severe intermittent pain in the forefoot • Care – padding; shoes; surgery Turf toe • Cause – hyperextension of 1st MTP joint from sudden trauma or overuse; turf • Signs – pain; swelling • Care – steel insoles; tape to prevent DF – Calluses – – • • Cause – shoes too narrow/short; friction; faulty foot mechanics • Signs – hard, cracked, layers of skin usually found on calcaneus and plantar aspect of foot • Care – emery callus file; wedges; doughnuts; orthotics Ingrown toenail • Cause – toenail grown into soft tissue • Signs – inflammation; infection • Care – soak in hot water for 20 minutes; cotton; trimming nail across Toenail hematoma • Cause – stepped on; dropping object on toe; kicking another object • Signs – extreme pain; bleeding in nail bed • Care – ice; drill nail The Ankle and Lower Leg Anatomy – Bones • Tibia • Fibula • Talus • Calcaneus – Ligaments • Lateral • Tibiofibular-anterior & posterior; holds the tibia & fibula together • Anterior talofibular (ATF) – prevents anterior displacement of talus • Posterior talofibular (PTF) – prevents posterior displacement of talus • Calcaneofibular – restrains inversion of calcaneous • Medial • Deltoid – triangular in shape; restrains eversion of calcaneous – • Musculature Anterior Compartment extensor digitorium longus extensor hallicus longus tibialis anterior Superficial posterior compartment gastrocnemius soleus Deep posterior compartment tibialis posterior flexor digitorium longus flexor hallicus longus Lateral compartment peroneus longus peroneus brevis Prevention – Heel cord stretching • Before and after activity – Strength training • Achieving static & dynamic joint stability – Neuromuscular control • Enhanced by locomotion on uneven surfaces or balance board – Footwear – • • Shoes for which they are intended Taping/bracing • Prophylactic protection Assessing the Lower Leg – History • Is there any sense of muscle weakness or difficulty in walking? • Could you bear weight right away? • Have you hurt the ankle before? • Was there immediate swelling, or did the swelling occur later (or at all)? – Observation • Is there a normal walking pattern? • Are the bony contours of the ankle normal and symmetrical, or is there a deviation such as a bony deformity? • Are the color and texture of the skin normal? • Is there crepitus or abnormal sound in the ankle joint? – Palpation – • Bony & soft tissue • Determine obvious structural deformities, areas of swelling, or points of tenderness Special tests • Thompson test – squeeze the calf muscle while the leg is extended and the foot is hanging over the edge of the table; + test is one in which squeezing the calf muscle does not cause the heel to move or pull upward • Homan’s sign – athlete is in a supine position with the knee fully extended; the ankle is passively dorsiflexed so that the calf muscles are stretched; + test is pain in the calf – indication of deep vein thrombophlebitis • Bump, lever, and compression - + test indicates a possible fracture to lower leg and/or ankle • Anterior drawer test – athlete sits with legs and feet relaxed; grasping the lower leg in one hand and the calcaneus in the palm of the other hand, the tibia is pushed backward as the calcaneus is pulled forward; + test occurs when the foot slides forward and sometimes makes a clunking sound as it reaches its end point indicating a tear in the ATF ligament • Talar tilt test – with the foot positioned at 90° to the lower leg and stabilized, the calcaneus is inverted; + test is excessive motion of the talus indicating injury to the CF and possibly the ATF and PTF ligaments • • Functional Exam – If the following movements aggravate a recent injury, they should be avoided • Walks on toes (tests PF) • Walks on heels (tests DF) • Walks on lateral border of feet (tests inversion) • Walks on medial border of feet (tests eversion) • Hops on the injured ankle • Start/stop run motion • Changing directions quickly • Figure 8’s Injuries to the Ankle – Ankle sprains – – • • Cause – INV/PF most common; EV may involve avulsion-longer to heal • Signs – tearing of ligament; swelling; joint instability; grades • Care – RICE; NSAIDs; horseshoe; splint; NWB; rehab Ankle fractures • Cause – same MOI as sprains • Signs – immediate swelling; point tenderness over bone; apprehension to bear weight • Care – splint; referral; cast for 6 weeks; rehab Tendinitis • Cause – faulty foot mechanics; footwear; acute trauma; tight heel cord; training errors • Signs – pain with active and passive movement; swelling; crepitus; stiffness • Care – rest; ice; NSAIDs; orthotics/tape Injuries to the Lower Leg – Tibial and fibular fractures • Cause – tibia – most common long bone fx; direct or indirect trauma-combination of rotation & compression force • Signs – immediate pain; swelling; deformity; pain with ambulation • Care – referral; immobilization for weeks/months – Tibial and fibular stress fractures • Cause – tibia > fibula; repetitive loading; jumping athletes • Signs – pain with activity; worse when stopped; focal pt. tenderness on bone vs. diffuse • Care – REST; weight bearing is OK-sometimes with a walking boot – Shin splints (Medial Tibial Stress Syndrome) • Cause – strain of tibialis posterior in running activities; secondary to faulty foot mechanics; heel cord tightness; muscle weakness; shoes; changing surfaces • Signs – diffuse pain distal tibia; initially pain is post activity, but as the condition progresses, pain is with daily ambulation, and in the morning there is pain and stiffness • Care – rule out stress fracture; G/S stretching; ice; strengthening of lower leg muscles; correct foot mechanics • Compartment syndrome – Cause – increase in pressure causes compression of muscle & neurovascular structures; acute – direct trauma; acute exertional – no trauma; evolves with minimal to excessive activity; chronic – symptoms consistent at certain point in activity & ceases post activity – Signs – deep aching pain; tightness/swelling of compartment; pain with passive stretch; neurological involvement is rare – Care – ice; elevation; no compression NSAIDs; surgery (fasciotomy) • Achilles’ tendon rupture – Cause – sudden, forceful PF; 30 + - ballistic movement • Signs – feel/hear pop; kicked/shot; PF is painful & limited; palpable defect • Care – surgery; 6-8 weeks immobilization • Achilles’ tendinitis – Cause – repetitive stresses/strains; increase in duration/intensity is too soon; hill workouts increase the pain – Signs – general pain & stiffness; gradual onset; morning pain/stiffness; warm & painful to palpation; thickening; crepitus – Care – decrease activity; G/S stretching – – • Shin contusions • Cause – forceful blow to the anterior leg • Signs – intense pain; hematoma forms & is jellylike; possible compartment syndrome or fracture • Care – RICE; NSAIDs; padding Leg cramps and spasms • Cause – fatigue; excess loss of fluid • Signs – pain with contraction of the calf muscle • Care – mild, gradual stretching; ice massage; water/electrolyte replacement Gastrocnemius strain – Cause – medial head is particularly susceptible; sports that require quick stops/starts and jumping; quick stop with foot planted flat and suddenly extends the knee – – Signs – pain; swelling; muscle disability; “hit in the calf with a stick” Care – gentle, gradual stretch after muscle cooling; wedge in shoe; elastic wrap