Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
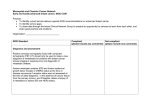
Clinical Medicine: Therapeutics Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. A Review of Vinorelbine in the Treatment of Advanced Breast Cancer A. Brunello, A. Roma, U. Basso and A. Jirillo Istituto Oncologico Veneto, Division of Medical Oncology, 35126 Padova, Italy. Email: [email protected] Abstract: Vinorelbine is a semi-synthetic vinca alkaloid that has been shown active in many tumor types and is currently registered for the treatment of advanced breast cancer (ABC) and non-small cell lung cancer (NSCLC), and it is used in other cancer type such as prostate cancer, lymphomas, gynecologic malignancies. This agent has a generally favorable safety profile, and may be suitable for use in special populations such as the elderly and/or frail patient. However, with the taxanes established as standard second line treatment for ABC after failure of an anthracycline, Vinorelbine has been generally relegated for use as third line therapy, in competition with the oral compound Capecitabine. Combination regimens of Vinorelbine and Gemcitabine have been indeed widely studied, and have been demonstrated to be safe and effective. More recently, the exciting results observed with the combination of Vinorelbine and Trastuzumab in patients with Her-2 overexpressing tumors, as well as the development of a reliable formulation and revised schedule of oral Vinorelbine appear to have revived the interest in this compound in the management of this disease. Yet, data from properly designed randomized clinical trials are eagerly awaited to confirm the amount of available data which are mostly based on phase II studies. Keywords: vinorelbine, advanced breast cancer, vinca alkaloid, trastuzumab, oral Clinical Medicine: Therapeutics 2009:1 1715–1726 This article is available from http://www.la-press.com. © Libertas Academica Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://www.creativecommons.org/licenses/by/2.0) which permits unrestricted use, distribution and reproduction provided the original work is properly cited. The authors grant exclusive rights to all commercial reproduction and distribution to Libertas Academica. Commercial reproduction and distribution rights are reserved by Libertas Academica. No unauthorised commercial use permitted without express consent of Libertas Academica. Contact [email protected] for further information. Clinical Medicine: Therapeutics 2009:1 1715 Brunello et al Introduction These structural modifications give highly specific antimitotic properties to Vinorelbine, as well as enhanced lipophilicity. Similarly to other vinca alkaloids, Vinorelbine induces cytotoxic effects by inhibiting polymerization of tubulin dimers into microtubules, disrupting mitotic spindle formation and preventing cell division. Thus, its activity is cell cycle specific. Vinorelbine is selective for mitotic microtubules; it has minimal to no activity (except in higher concentrations) on axonal or other microtubule classes, with a reduction in the frequency and severity of neuro-toxicity, typically observed with other microtubule agents.3 Vinorelbine is extensively metabolized in the liver through cytochrome P450 iso-enzymes of the CYP3A subfamily. Biliary excretion is the predominant route of elimination, accounting for at least 50% of an intravenous dose. Extensive biliary excretion of metabolites also appears to occur.4,5 The elimination half-life after intravenous administration is 42 to 45 hours and 24 to 56 hours after oral administration.5,6 Pharmacokinetics in elderly patients (older than 65 years) is similar to those reported in younger people.7 This report reviews the most important studies involving Vinorelbine in ABC with particular regard to the results of randomized trials in order to evaluate its role in this subset of patients. Vinorelbine represents both an active and a well tolerated treatment for metastatic breast cancer in patients who display anthracycline and/or taxanesrefractory disease, or who are not suitable for such treatments. Some concerns, though, have been raised Despite the recent trend toward treatment of early stage breast cancer aggressively with anthracyclines and taxanes, nearly half of those women will have metastatic recurrence. Advanced breast cancer (ABC) generally responds to chemotherapy yet, given the usual prior exposure to these drugs, many women facing first-line therapy for recurrent disease will now have developed anthracycline- and taxane-refractory metastatic breast cancer, presenting a major therapeutic challenge. A number of established drugs have proved to be effective in this setting: Capecitabine; Gemcitabine; Vinorelbine; and new drugs are currently being developed, such as camptothecins, epothilones, mitosis inhibitor E7389, the ascidian-derived anticancer compound trabectedin and others. ABC is however an incurable disease, with a median survival of 2–3 years, with response rates to monotherapy ranging from about 20%–75% in chemotherapy-naïve patients.1 Moreover, the quantity and quality of the available evidence regarding the efficacy of currently used drugs in patients with locally advanced or metastatic breast cancer previously treated with both a taxane and an anthracycline are extremely limited.2 Vinorelbine (5’-noranhydrovinblastine) is a semisynthetic vinca alkaloid, from the Catharanthus alkaloid family. The clinical development of Vinorelbine started in the 1980s and, although a derivative of Vinblastine, Vinorelbine is structurally different, with an 8-membered ring as opposed to the 9-membered ring characteristic of naturally occurring vinca alkaloids. VINBLASTINE VINORELBINE OH N N CH3 H H N H N H C O CH3 N OCH3 C O OCH3 N H3CO H3CO CH3 H N H3C O O H C OH OCH3 C N O CH3 CH3 H H3C O O H C O C O CH3 OCH3 Figure 1. 1716 Clinical Medicine: Therapeutics 2009:1 Vinorelbine in ABC about a potential cross-resistance between taxanes and Vinorelbine, and contradictory evidence exists on the use of Vinorelbine in patients with disease refractory to taxanes. In a phase II trial, no responses were seen with Vinorelbine among 14 patients with ABC refractory to taxanes,8 whereas other studies indicate possible responses in patients treated with Vinorelbine for ABC judged taxane-refractory.9–11 In the next paragraphs single agent activity and combinations regimens with Vinorelbine are discussed, as well as combinations with targeted therapy, namely Trastuzumab. Vinorelbine: single agent activity Many phase II studies have demonstrated the activity and tolerability of intravenous administration of Vinorelbine, with response rates ranging from 40%– 60% in chemo-naïve disease and with good tolerability,12 Table 1. Vinorelbine rarely induces total alopecia or severe gastrointestinal events or symptomatic cardiac events. The major dose-limiting hematological toxicity associated with Vinorelbine is neutropenia. Common non-hematological side-effects include G1–G2 peripheral neuropathy, constipation and phlebitis. Because of its clinical activity and its mild toxicity profile and, in particular, the absence of alopecia could be particularly attractive for women. Indeed, for all the above mentioned reasons, Vinorelbine as single agent represents a valid alternative in the treatment of metastatic breast cancer in elderly patients. Sorio and colleagues demonstrated that Vinorelbine administered intravenously at the dose of 30 mg/m2 on days 1 and 8 every 3 weeks was well tolerated. Responses were observed in 6 out of 20 evaluable patients (ORR 30%) and no correlation between dosage, age and toxicity was observed.7 In another study, Vinorelbine was administered weekly at the same dosage (30 mg/m2). The dose-limiting toxicity observed was hematologic, easily recovered with dose adjustment. Asthenia, gastroenteric toxicity and injection site reactions were the predominant nonhematologic adverse events. Neurotoxicity and alopecia were relatively infrequent and mild.13–15 Only two randomized phase III trials are available testing Vinorelbine single agent,16,17 Table 2. Vinorelbine given with schedule 30 mg/m2 (days 1 and 8)16 has been shown to be as effective as single agent as in the combination with Gemcitabine as for overall survival, whereas the combination significantly improves progression-free survival (PFS), when toxicity was significantly higher in the combination arm. The study by Jones and colleagues explored Vinorelbine with schedule 30 mg/m2 weekly,17 showing a survival benefit in anthracycline-refractory ABC with use Table 1. Phase II studies involving Vinorelbine in ABC patients. Authors N Route Setting ORR PFS months OS months 145 i.v. 1st line 41 5.8 18 50 i.v. 1st line 50 5 15 44 i.v. 1st line 41 6 NA Weber et al 60 i.v. 1st line 35 4.5 15.5 Bruno et al 63 i.v. 1st line 44 3 11.7 56 i.v. 1st line 38 9 NA 27 i.v. 1st line 59 NA 19 34 i.v. 1st line 50 4.4 10 100 i.v. 2nd line 16% NA NA 60 i.v. 1st line, 2nd line 12% 3.0 10.3 50 i.v. 1st line 20% 3.4 NA 131 oral 2nd line 11% NA 9.9 72 oral 1st line 24% NA NA Fumoleau et al 18 Garcia-Conde et al Romero et al 20 21 22 Vogel et al 13 Terenziani et al Twelves et al 23 24 Degardin et al Langkjer et al 25 26 Toi et al27 Winer et al28 Amadori et al 29 19 Clinical Medicine: Therapeutics 2009:1 1717 Brunello et al Table 2. Phase III randomized studies involving single agent Vinorelbine in ABC patients. Authors Arms Martin et al ORR PFS months OS months 26% 4.0 16.4 36% 6.0 15.9 Vinorelbine 30 mg/m weekly 46% 2.8 8.7 Melphalan 25 mg/m every 4 weeks i.v 28% 2.0 7.7 PLD 10% 2.9 11 V (or MC + Vbt)* 12% 2.5 9 Vinorelbine 30 mg/m 16 2 Vinorelbine + Gemcitabine 30/1200 mg/m Jones et al 17 2 2 2 Keller et al 11 *14% of patients in the V arm actually received Mitomicin (MC) and Vinblastine (Vbt). of Vinorelbine versus Melphalan, with comparable toxicity and quality of life. In a more recent trial performed in a population of 301 women with ABC who had failed a taxane as first or second line therapy, Vinorelbine (which was the chosen comparator in 85% of the cases; n = 129) was shown equivalent to Pegylated Liposomal Doxorubicin (PLD), a novel Doxorubicin formulation with comparable efficacy and better safety profile.11 Only the subgroup of patients without previous exposure to anthracyclines (17% of the study population) had a somewhat better PFS with PLD. Combination regimens with Vinorelbine One of the virtues of Vinorelbine is the fact that, in view of its mild toxicity profile, it can be easily combined with virtually any other cytotoxic. A large number of phase II trials have been performed which have generally shown encouraging activity with an acceptable safety profile (Table 3). Examples include Paclitaxel30–37 Docetaxel;38–46 Doxorubicin;47–51 Epirubicin52–54 Mitoxantrone;55–57 Pegylated Liposomal Doxorubicin;14,58–61 Gemcitabine;62–73 5-Fluorouracil;74–79 platinum compounds;80–83 and Capecitabine,84–88 which will be separately discussed. Several triplets have also been investigated but increased toxicity should be expected.89–92 Some of these combinations were eventually investigated in phase III trials, and will be discussed in more detail in the following section. The combination of Vinorelbine and 5-Fluorouracil, one of the most extensively studied in patients with ABC, was compared to Docetaxel in a small randomized phase III trial (sample size 176 patients).93 Although there were no differences in terms of efficacy, the combination resulted in more toxicity, with also toxic deaths registered, as compared to single agent Docetaxel. Yet, it must be noticed that high doses of 5-Fluouracil (750 mg/m2/day for 5 days) have been administered in this trial. Randomized trials have evaluated the addition of Vinorelbine to an anthracycline such as Mitoxantrone,94 Doxorubicin,95,96 and Epirubicin97 against Table 3. Combination regimens with Vinorelbine. Authors Arms Setting ORR PFS months OS months Toxicity V + 5FU Docetaxel Previous anthracyclines 43% 39% 5.1 6.5 15 16 More Namer et al94 V + Mitoxantrone FAC/FEC 1st line 35% 33% 8 5 20 16 More Blajman et al95 V + Doxorubicin FAC 1st line 75% 74% 7.5 9 17.8 17.3 Similar Norris et al96 V + Doxorubicin Doxorubicin 1st/2nd line 38% 30% 6.2 6.1 13.8 14.4 More Ejlertsen et al97 V + Epirubicin Epirubicin 1st line 50% 42% 10.1 8.2 19.1 18.0 More Bonneterre et al 1718 93 Clinical Medicine: Therapeutics 2009:1 Vinorelbine in ABC standard anthracycline arms. Only one of these trials suggested an advantage for the combination in terms of response rates and progression-free survival, at the price of higher toxicities for the combination arms. Generally, toxicities for the combination arms were statistically increased in the combination arms in trials comparing single agent versus combination with Vinorelbine. These results are in line with those of other randomized clinical trials in ABC, showing that combination chemotherapy is usually not superior to optimal sequential treatment, and is likely to result in more toxicity, therefore the use of combination chemotherapy regimens in advanced settings should be limited to those patients requiring rapid shrinking of life-threatening tumors. Vinorelbine and Capecitabine, Phase II studies Vinorelbine is currently occupying a delicate place in the management of ABC especially for third line therapy after failure of anthracyclines and taxanes, in open competition with the oral compound Capecitabine, an oral fluoropyrimidine carbamate which is enzymatically converted via a 3 enzymatic step to 5’-deoxy-5-fluorocytidine (5’-DFCR), 5’-deoxy5-fluorouridine (5’-DFUR), and finally 5-FU. To date, no randomized phase III trial comparing directly Vinorelbine vs. Capecitabine has been performed. The limited data coming from a phase II study98 and retrospective data sets99,100 show similar activity of the two agents or, in the case of retrospective data, higher activity for Capecitabine. In particular, safety profiles are different, with more G3–G4 hematological toxicity for Vinorelbine, and more grade 3 cutaneous toxicity for Capecitabine. In addition, Capecitabine and Vinorelbine have been compared in a pharmacoeconomic analysis performed in the United States. Mean monthly cost for patients with advanced breast cancer was higher for patients receiving Vinorelbine when compared to matched patients receiving Capecitabine and the main difference in cost was dictated by management of treatment related toxicity and chemotherapy i.v. administration.101 Capecitabine is an attractive combination partner since it displays a high single agent activity and a non overlapping toxicity profile, with only minimal myelodepression and no alopecia. Moreover, there Clinical Medicine: Therapeutics 2009:1 is a synergistic effect due to Vinorelbine mediated up-regulation of thymidine phosphorilase (TP), which has a crucial role in the 3-step conversion of Capecitabine to 5-FU at tumor site.102 The combination of Capecitabine and Vinorelbine has been investigated in a variety of phase I studies and phase II studies, which are illustrated in Table 4. Recently, an oral formulation of Vinorelbine has become available. Some studies also evaluated an all oral combination of Vinorelbine and Capecitabine, which could represent an attractive option in particular subsets of patients, such as elderly patients. Oral Vinorelbine Among the options for treatment of anthracycline- and taxanes-pretreated advanced breast cancer, Capecitabine has been generally preferred by patients because of the convenience of the oral route, but recently a novel oral formulation of Vinorelbine (ONVB) which has apparently overcome the problem of erratic absorption has become available. In patients with NSCLC, oral and intravenous Vinorelbine have been shown to have comparable activity.115 In pharmacokinetic studies, equivalence in bioavailability has been demonstrated between the oral and intravenous formulation.116 Oral Vinorelbine is rapidly absorbed, with a Tmax of 0.75–1.4 hours.116,117 Bioavailability of soft-gelatine capsules, the third and most recent oral formulation of Vinorelbine, is 33%–43%,116,117 with 38% inter-individual variability.116 Low bioavailability may be attributed to both incomplete absorption and to a first-pass effect (intestinal and hepatic). The problems with hematologic toxicity observed in earlier trials,118 have been managed by administering the first course of ONVB at the dose of 60 mg/m2 days 1 and 8, and only if no toxicity is observed escalating to a dose of 80 mg/m2 days 1 and 8. This helped reducing the severe toxicity which was typically observed at first cycle, with the occurrence of even toxic deaths in the earlier trials.118 This schedule has demonstrated moderate efficacy but is characterized by a high rate of neutropenia, the risk of which increases after dose escalation to 80 mg/m2.119 Consequently close hematological monitoring is essential.118 Furthermore, differently from intravenous formulation, oral Vinorelbine has been shown to be associated with frequent nausea, vomiting and 1719 Brunello et al Table 4. Phase II studies in first and subsequent lines of Vinorelbine and Capecitabine for ABC. Author N Dose (mg/m2) C days 1–14 V days 1 and 8 ORR TTP OS Elghazaly et al103 45 C 2000 V 25 64% 9 NA Ghosn et al85 30 C 1700 V 25 70% 10 30.4 Ghosn et ala,104 40 C 1700 V 25 55% 12.3 35.8 Köler et alb,105 30 C 2000 V 25 77% NA NA Hess et alb,106 70 C 1000/1300 V 20 43%–57% 4.3/7.0 NA Iodice et alb,107 53 C 2000–2500 V 20–25 62% 12.1 21.3 Palumbo et al108 32 C 2000 V 25 72% 9.1 NA Stuart et al88 58 C 2000 V 25 43% NA NA Davis et al109 22 C 2000 V 25 33% 5.8 3.5 Orphanos et al110 30 C 2000 V 20 50% NA NA Estévez et al111 31 C 2000 V 20 49% 7.6 27.2 Lorusso et al112 38 C 2000 V 25 37% 6.8 11.3 Xu B et al113 77 C 1900 V 25 47% 6 NA Ahn et al114 44 C 2500 V 25 50% 5.3 17 1st line 2nd line a b Sequential Docetaxel. Studies specifically addressed to elderly patients. diarrhea,118,119 and prophylactic antiemetics are recommended.118 Nonetheless, oral formulation may be attractive for patients not willing to be treated with i.v. drugs and for elderly patients, a subset of patients in which it has been demonstrated fair safety of this formulation, though activity raises concerns.120 Although experience with oral Vinorelbine is less extensive than with the intravenous formulation, the pivotal phase II trial that has investigated the new schedule in patients with ABC resulted in response rates of 31% and median duration of response of 4 months in previously untreated patients.119 Furthermore, it has 1720 been shown that ONVB brings added value in terms of patients’ convenience allowing improved quality of life and reduced hospital stays while keeping optimal compliance to treatment schedule in a French experience.121 All oral combinations of Vinorelbine and Capecitabine have been investigated in phase I and II studies, with overall response rates ranging from 26%–61%, median progression-free survival 6–10.5 months and median overall survival 10–48 months.87,122 In particular, when used in first line settings, response rates are in the range of 44%–51% with median Clinical Medicine: Therapeutics 2009:1 Vinorelbine in ABC progression free survival of 8.4 months.86,123 Among the major benefits for these combination regimens is the possibility of continuing therapy for prolonged periods in patients with controlled disease, whereas this would not be possible for anthracycline and/or taxanes containing regimens due to cumulative toxicity. Recently, new metronomic schedules have been proposed, which can be appealing for the low toxicities and manageable side effects that render the schedule easily applicable to vulnerable populations such as elderly patients oral Vinorelbine 80 mg/m2 fractionated in days 1, 3, and 5, three week on-one week off, every 4 weeks. ORR 41%, with median time to disease progression was 7.1 months and median overall survival was 12.7 months.124 with a taxane (e.g. prior exposure to taxanes, pre-existing peripheral neuropathy, patient’s choice depending on potential side effects), Vinorelbine has been demonstrated an effective option. In the preclinical setting, synergism between Trastuzumab and Vinorelbine has been demonstrated.127 Vinorelbine and Trastuzumab have no overlapping toxic effects, which contrast with the use of Trastuzumab in combination with anthracyclines.128 A phase I dose-finding study evaluated escalating doses of Vinorelbine in 12 patients.129 Vinorelbine was given at doses of 20, 25 and 30 mg/m2 in successive cohorts, on a day 1 and 8 schedule every 21 days, in combination with Trastuzumab. Toxic effects were primarily hematological; one case of febrile neutropenia and one episode of acute cholecystitis were noted among six assessable patients receiving Vinorelbine 30 mg/m2 and this was therefore determined as the maximum tolerated dose. Several phase II trials (Table 5) and one phase III trial130 have now reported data for Trastuzumab in combination with Vinorelbine in the HER2-positive MBC setting. The trials have included 450 assess able patients, the majority (94%) having HER2positive status, defined as an immunohistochemistry (IHC) score of 3+ or by FISH. In particular, in the phase III trial,130 the Vinorelbine-Trastuzumab combination showed similar efficacy to the weekly Vinorelbine and HER2 positive disease Trastuzumab, a 95% humanized monoclonal antibody targeted against the extracellular domain of the HER-2 receptor, is the standard of care for patients with HER2 over-expressing tumors (about 20% of breast carcinomas) in association with chemotherapy. In the pivotal trials of single agent Trastuzumab, response rates of 15% and 30% have been reported in previously treated125 and untreated126 patients. Trastuzumab is frequently combined with a taxane, however in patients who are not suitable for therapy Table 5. Trials with combination of Trastuzumab and Vinorelbine. Authors Jahanzeb et al N Schedule Setting ORR PFS months OS months 40 30 mg/m /w 1st line 78% 72 w NA Bernardo et al132 48 25 mg/m2/w 1st line 86% 2 NA Burstein et al 133 54 25 mg/m /w 1st line 68% 5.6 NA Burstein et al 15 40 25 mg/m /w 1st line 75% NA NA 69 30 mg/m /w 1st line 62% 9.9 23.7 52 25 mg/m /w 1st line 58% 7 26 69 30 mg/m /w NA 61% 10 NA Chan et al 131 134 Bayo-Callero et al Porta et al 135 136 Schilling et al 2 2 2 2 2 2 41 25 mg/m /w NA 44% 7.8 NA Franquesa et al138 18 25 mg/m2/w 1st and 2nd line 44% 11.9 NA Brunello et al 19 20–30 mg/m /w 1st line 57% NA NA 35 25 mg/m /w 2nd line 51% 9 27 25 25 mg/m /w up to 4th 72% NA NA 41 25 mg/m /w 1st line 51% 8.5 NA 139 Papaldo et al Lal et al 137 140 141 Burstein et al 2007* ,130 2 2 2 2 2 *Phase III trial. Clinical Medicine: Therapeutics 2009:1 1721 Brunello et al taxanes-Trastuzumab combination, yet the trial was prematurely closed due to slow accrual. On the contrary of trials of combination taxanesTrastuzumab, the studies of combination VinorelbineTrastuzumab demonstrate a more favorable therapeutic index, with rates of cardiomiopathy not higher than those reported with Trastuzumab single agent. Although it would be inappropriate to consider the combination Trastuzumab-Vinorelbine as standard treatment for patients with Her-2 overexpressing ABC in the absence of controlled trials, this schedule may be considered an acceptable option for patients willing to avoid the side effects associated with taxanes (such as alopecia), or for selected patients relapsing after previous exposure to taxanes, a situation likely to be more common with the increasing use of taxanes in the (neo-)adjuvant setting. Schedules with three-weekly Trastuzumab have been studied as well,142 with manageable toxicity and activity which falls in the range of expected response rates for weekly schedules, though at the lower limits. The oral formulation of Vinorelbine has also been investigated in association with Trastuzumab for HER2 overexpressing tumors. An observational study143 demonstrated that the combination is an effective and safe treatment option for HER2 positive ABC, with response rates and time to progression depending mainly on line of treatment; a schedule which consists of intravenous Vinorelbine on day 1 and oral Vinorelbine on day 8 and Trastuzumab has also been studied144 and results showed high antitumor efficacy, with overall response rate 62%, and excellent tolerability in 1st-line treatment of HER2 overexpressing ABC. Conclusions The increasing evidence that anthracyclines and taxanes improve the survival of patients with breast cancer in the adjuvant setting has led to a restricted use of these drugs in women with metastatic disease.145 Combination regimens of Vinorelbine with anthracyclines or taxanes have been demonstrated to have same efficacy of the single agent (anthracycline or taxanes), in some cases improving the overall response rate, but usually at the price of increased toxicity that does not justify the use of such combinations. On the contrary, association with newer drugs such as Gemcitabine or Capecitabine have shown increased efficacy over 1722 the single agent, with manageable toxicity profile. Although Vinorelbine is clearly an active and well tolerated agent in BC, its use is currently limited by the lack of properly designed controlled trials. Generally, Vinorelbine as a single agent is not recommended in patients who are anthracycline naïve though it may be considered a reasonable option for patients willing to prioritize quality of life over maximum chance of tumor response. Single agent Vinorelbine or combinations of Vinorelbine and Capecitabine can be considered an alternative to the use of anthracyclines and taxanes in special populations of patients, such as the elderly and/or frail patients or in those willing to avoid alopecia and/or to prioritize other aspects of quality of life. The new oral formulation of Vinorelbine is particularly indicated for patients with disease characterized by low aggressiveness with or without visceral metastasis, or slowly progressing disease. In addition, recently Vinflunine, a novel fluorinated Vinca alkaloid, has become available and is currently under study for treatment of breast cancer progressing after anthracycline- and taxanebased chemotherapy. The availability of Vinorelbine and other novel, well tolerated and effective treatments provides greater potential to tailor treatment to meet individual patient needs and, therefore, also provide the potential to improve patient outcomes. Disclosures The authors report no conflicts of interest. References 1. Nicolini A, Giardino R, Carpi A, et al. Metastatic breast cancer: an updating. Biomed Pharmacother. 2006;60:548–56. 2. Jassem J, Carroll C, Ward SE, et al. The clinical efficacy of cytotoxic agents in locally advanced or metastatic breast cancer patients pretreated with an anthracycline and a taxane: A systematic review. Eur J Cancer. 2009. [Epub ahead of print]. 3. Toso C, Lindley C. Vinorelbine a novel vinca alkaloid. Am J Health Syst Pharm. 1995;52(12):1287–304. 4. Feigal EG, Christian M, Cheson B, et al. New chemotherapeutic agents in non-small cell lung cancer. Semin Oncol. 1993;20:185–201. 5. Jehl F, Quoix E, Leveque D, et al. Pharmacokinetic and preliminary metabolic fate of Navelbine in humans as determined by high performance liquid chromatography. Cancer Res. 1991;51:2073–6. 6. Marquet P, Lachatre G, Debord J, et al. Pharmacokinetics of vinorelbine in man. Eur J Clin Pharmacol. 1992;42:545–7. 7. Sorio R, Robieux I, Galligioni E, et al. Pharmacokinetics and tolerance of vinorelbine in elderly patients with metastatic breast cancer. Eur J Cancer. 1997;33(2):301–3. 8. Fazeny B, Zifko U, Meryn S, et al. Vinorelbine-induced neurotoxicity in patients with advanced breast cancer pretreated with paclitaxel—a phase II study. Cancer Chemother Pharmacol. 1996;39(1–2):150–6. Clinical Medicine: Therapeutics 2009:1 Vinorelbine in ABC 9. Zelek L, Barthier S, Riofrio M, et al. Weekly vinorelbine is an effective palliative regimen after failure with anthracyclines and taxanes in metastatic breast carcinoma. Cancer. 2001;92(9):2267–72. 10. Udom DI, Vigushin DM, Linardou H, et al. Two weekly vinorelbine: administration in patients who have received at least two prior chemotherapy regimes for advanced breast cancer. Eur J Cancer. 2000;36(2):177–82. 11. Keller AM, Mennel RG, Georgoulias V, et al. A randomized phase III trial of Pegylated Liposomal Doxorubicin versus vinorelbine or mitomycin C plus vinblastine in women with taxane-refractory advanced breast cancer. J Clin Oncol. 2004;22(19):3893–901. 12. Gregory RK, Smith IE. Vinorelbine—a clinical review. Br J Cancer. 2000;82:1907–13. 13. Vogel C, O’Rourke M, Winer E, et al. Vinorelbine as first-line chemotherapy for advanced breast cancer in women 60 years of age or older. Ann Oncol. 1999;10(4):397–402. 14. Addeo R, Faiola V, Guarrasi R, et al. Liposomal Pegylated Doxorubicin plus vinorelbine combination as first-line chemotherapy for metastatic breast cancer in elderly women /= 65 years of age. Cancer Chemother Pharmacol. 2008;62(2):285–92. 15. Burstein HJ, Kuter I, Campos SM, et al. Clinical activity of trastuzumab and vinorelbine in women with HER2-overexpressing metastatic breast cancer. J Clin Oncol. 2001;19(10):2722–30. 16. Martin M, Ruiz A, Munoz M, et al. Gemcitabine plus vinorelbine versus vinorelbine monotherapy in patients with metastatic breast cancer previously treated with anthracyclines and taxanes: final results of the phase III Spanish Breast Cancer Research Group (GEICAM) trial. Lancet Oncol. 2007;8: 219–25. 17. Jones S, Winer E, Vogel C, et al. Randomized comparison of vinorelbine and melphalan in anthracycline-refractory advanced breast cancer. J Clin Oncol. 1995;13(10):2567–74. 18. Fumoleau P, Delgado FM, Delozier T, et al. Phase II trial of weekly intravenous vinorelbine in first-line advanced breast cancer chemotherapy. J Clin Oncol. 1993;11(7):1245–52. 19. Garcia-Conde J, Lluch A, Martin M, et al. Phase II trial of weekly IV vinorelbine in first-line advanced breast cancer chemotherapy. Ann Oncol. 1994;5(9):854–7. 20. Romero A, Rabinovich MG, Vallejo CT, et al. Vinorelbine as first-line chemotherapy for metastatic breast carcinoma. J Clin Oncol. 1994;12(2):336–41. 21. Weber BL, Vogel C, Jones S, et al. Intravenous vinorelbine as first-line and second-line therapy in advanced breast cancer. J Clin Oncol. 1995;13(11): 2722–30. 22. Bruno S, Puerto VL, Mickiewicz E, et al. Phase II trial of weekly i.v. vinorelbine as a single agent in first-line advanced breast cancer chemotherapy. The Latin-American experience. Am J Clin Oncol. 1995;18(5): 392–6. 23. Terenziani M, Demicheli R, Brambilla C, et al. Vinorelbine: an active, non-cross-resistant drug in advanced breast cancer. Results from a phase II study. Breast Cancer Res Treat. 1996;39(3):285–91. 24. Twelves CJ, Dobbs NA, Curnow A, et al. A phase II, multicentre, UK study of vinorelbine in advanced breast cancer. Br J Cancer. 1994;70(5):990–3. 25. Degardin M, Bonneterre J, Hecquet B, et al.Vinorelbine (navelbine) as a salvage treatment for advanced breast cancer. Ann Oncol. 1994;5(5):423–6. 26. Langkjer ST, Ejlertsen B, Mouridsen H, et al. Danish Breast Cancer Co-operative Group. Vinorelbine as first-line or second-line therapy for advanced breast cancer: a Phase I–II trial by the Danish Breast Cancer Co-operative Group. Acta Oncol. 2008;47(4):735–9. 27. Toi M, Saeki T, Aogi K, et al. Late phase II clinical study of vinorelbine monotherapy in advanced or recurrent breast cancer previously treated with anthracyclines and taxanes. Jpn J Clin Oncol. 2005;35(6):310–5. 28. Winer EP, Chu L, Spicer DV. Oral vinorelbine (Navelbine) in the treatment of advanced breast cancer. Semin Oncol. 1995;22(2 Suppl 5):72–8. 29. Amadori D, Koralewsky P, Tekiela A. Efficacy and safety of navelbine oral (NVBo) in first line metastatic breast cancer (MBC). Eur J Cancer. 2001;37:22. Abstr. 713 30. Romero AL, Langhi M, Perez J, et al. Vinorelbine and Paclitaxel as firstline chemotherapy in metastatic breast cancer. J Clin Oncol. 1999;17(1): 74–81. Clinical Medicine: Therapeutics 2009:1 31. Martin M, Lluch A, Casado A, et al. Paclitaxel plus vinorelbine: an active regimen in metastatic breast cancer patients with prior anthracycline exposure. Ann Oncol. 2000;11(1):85–9. 32. Michelotti A, Gennari A, Salvadori B, et al. Paclitaxel in combination with vinorelbine in pretreated advanced breast cancer patients. Semin Oncol. 1996; 23(5 Suppl 11):38–40. 33. Polyzos A, Tsavaris N, Kosmas C, et al. Full dose Paclitaxel plus vinorelbine as salvage chemotherapy in anthracycline-resistant advanced breast cancer: a phase II study. J Chemother. 2003;15(6):607–12. 34. Cocconi G, Mambrini A, Quarta M, et al. Vinorelbine combined with Paclitaxel infused over 96 hours (VI-TA-96) for patients with metastatic breast carcinoma. Cancer. 2000;88(12):2731–8. 35. Vici P, Amodio A, Di Lauro L, et al. First-line chemotherapy with vinorelbine and Paclitaxel as simultaneous infusion in advanced breast cancer. Oncology. 2000;58(1):3–7. 36. Bouillet T, Saintigny P, Levy E, et al. Weekly Paclitaxel (P) combined with biweekly vinorelbine (V) in metastatic breast cancer (MBC): final results of a clinical phase II study. ASCO annual meeting proceedings (post-meeting edition), J Clin Oncol. 2004;22(14S):783 [July 15 Supplement]. 37. Ellis GK, Gralow JR, Pierce HI, et al. Infusional Paclitaxel and weekly vinorelbine chemotherapy with concurrent filgrastim for metastatic breast cancer: high complete response rate in a phase I–II study of Doxorubicintreated patients. J Clin Oncol. 1999;17(5):1407–12. 38. Kornek GV, Ulrich-Pur H, Penz M, et al. Treatment of advanced breast cancer with vinorelbine and Docetaxel with or without human granulocyte colony-stimulating factor. J Clin Oncol. 2001;19(3):621–7. 39. Paz LDA, Lluch A, Martin M, et al. A phase II study of Docetaxel (D) and vinorelbine (V) in metastatic breast cancer (MBC). Proc Am Soc Clin Oncol. 1999; [abstract 452]. 40. Vassilomanolakis M, Koumakis G, Drufakou S, et al. Vinorelbine and Docetaxel as first-line chemotherapy in metastatic breast cancer. Cancer Chemother Pharmacol. 2003;51(2):179–83. [Epub 2000]. 41. Marti JL, Bueso P, Mayordomo JI, et al. Combination chemotherapy with Docetaxel plus vinorelbine in metastatic breast cancer patients with prior exposure to anthracyclines. Ann Oncol. 2001;12(8):1061–5. 42. Pectasides D, Dimopoulos MA, Aravantinos G, et al. First line combination chemotherapy with Docetaxel and vinorelbine in advanced breast cancer. A phase II study. Anticancer Res. 2001;21(5):3575–80. 43. Mayordomo JI, Milla A, Morales S, et al. Biweekly Docetaxel and vinorelbine as first-line chemotherapy in metastatic breast cancer. Clin Breast Cancer. 2004;5(2):131–5. 44. Gomez-Bernal A, Cruz JJ, Garcia-Palomo A, et al. Biweekly Docetaxel and vinorelbine in anthracycline-resistant metastatic breast cancer: a multicenter phase II study. Am J Clin Oncol. 2003;26(2):127–31. 45. Airoldi M, Cattel L, Pedani F, et al. Clinical data and pharmacokinetics of a Docetaxel-vinorelbine combination in anthracycline resistant/relapsed metastatic breast cancer. Acta Oncol. 2003;42(3):186–94. 46. Rodriguez J, Calvo E, Cortes J, et al. Docetaxel plus vinorelbine as salvage chemotherapy in advanced breast cancer: a phase II study. Breast Cancer Res Treat. 2002;76(1):47–56. 47. Spielmann M, Dorval T, Turpin F, et al. Phase II trial of vinorelbine/ Doxorubicin as first-line therapy of advanced breast cancer. J Clin Oncol. 1994;12(9):1764–70. 48. Alvarez A, Balbiani L, Block J, et al. Phase II study: navelbine (NVB) + adriamycin as first line chemotherapy in advanced breast cancer (ABC). Ann Oncol. 1994;5(Suppl 8). [Abstract 161]. 49. Hochster HS, Vogel CL, Burman SL, White R. Activity and safety of vinorelbine combined with Doxorubicin or fluorouracil as first-line therapy in advanced breast cancer: a stratified phase II study. Oncologist. 2010;6(3): 269–77. 50. Pawlicki M, Rolski J, Zaluski J, et al. A phase II study of intravenous navelbine and Doxorubicin combination in previously untreated advanced breast carcinoma. Oncologist. 2002;7(3):205–9. 51. Hegg R, Costa MA, Perdicaris M, et al. A phase II trial of fractionated vinorelbine/Doxorubicin as first-line therapy for advanced breast cancer. Curr Med Res Opin. 2001;16(4):225–34. 1723 Brunello et al 52. Baldini E, Tibaldi C, Chiavacci F, et al. Epirubicin/vinorelbine as first line therapy in metastatic breast cancer. Breast Cancer Res Treat. 1998;49(2): 129–34. 53. Vici P, Colucci G, Gebbia V, et al. First-line treatment with Epirubicin and vinorelbine in metastatic breast cancer. J Clin Oncol. 2002;20(11):2689–94. 54. Frontini L, Ardizzoia A, Giordano M, et al. Epirubicine-vinorelbine (EV) intravenous combination followed by oral vinorelbine (VNR) as first-line treatment in advanced breast cancer (ABC) patients: A POLONORD Group study, Proc Am Soc Clin Oncol. 2005;23. [Abstract 770]. 55. Llombart-Cussac A, Pivot X, Rhor-Alvarado A, et al. First-line vinorelbineMitoxantrone combination in metastatic breast cancer patients relapsing after an adjuvant anthracycline regimen: results of a phase II study. Oncology. 1998;55(5):384–90. 56. Adenis A, Vanlemmens L, Fournier C, et al. Does induction chemotherapy with a Mitoxantrone/vinorelbine regimen allow a breast-conservative treatment in patients with operable locoregional breast cancer? A French Northern Oncology Group trial in 105 patients. French Northern Oncology Group. Breast Cancer Res Treat. 1996;40(2):161–9. 57. Onyenadum A, Gogas H, Markopoulos C, et al. Mitoxantrone plus vinorelbine in pretreated patients with advanced breast cancer. Proc Am Soc Clin Oncol. 2005;23(16):93S. [Abstract 863]. 58. Rimassa L, Carnaghi C, Garassino I, et al. Unexpected low efficacy of stealth liposomal Doxorubicin (Caelyx) and vinorelbine in metastatic breast cancer. Breast Cancer Res Treat. 2003;77(2):185–8. 59. Martin M, Garcia-Donas J, Casado A, et al. Phase II study of Pegylated Liposomal Doxorubicin plus vinorelbine in breast cancer with previous anthracycline exposure. Clin Breast Cancer. 2004;5(5):353–7. 60. Gebbia V, Mauceri G, Fallica G, et al. Pegylated liposomal Doxorubicin with vinorelbine in metastatic breast carcinoma. A phase I–II clinical investigation. Oncology. 2002;63(1):23–30. 61. Mlineritsch B, Schabel-Moser R, Andel J, et al. Multicenter phase II study of Pegylated Liposomal Doxorubicin in combination with vinorelbine as first-line treatment in elderly patients with metastatic breast cancer. Onkologie. 2009;32(1–2):18–24. 62. Hortobagyi GN. Gemcitabine in combination with vinorelbine for treatment of advanced breast cancer. Clin Breast Cancer. 2002;3(Suppl 1):34–8. 63. Donadio M, Ardine M, Berruti A, et al. Gemcitabine and vinorelbine as second-line treatment in patients with metastatic breast cancer: a phase II study. Cancer Chemother Pharmacol. 2003;52(2):147–52. 64. Rossi E, Perrone F, Labonia V, et al. Is Gemcitabine plus vinorelbine active in second-line chemotherapy of metastatic breast cancer? a single-center phase 2 study. Oncology. 2003;64(4):479–80. 65. Morabito, Filippelli G, Palmeri S, et al. The combination of Gemcitabine and vinorelbine is an active regimen as second-line therapy in patients with metastatic breast cancer pretreated with taxanes and/or anthracyclines: a phase I–II study. Breast Cancer Res Treat. 2003;78(1):29–36. 66. Lobo F, Virizuela JA, Dorta FJ, et al. Spanish Group for Research in Breast Cancer. Gemcitabine/vinorelbine in metastatic breast cancer patients previously treated with anthracyclines: results of a phase II trial. Clin Breast Cancer. 2003;4(1):46–50. 67. Nicolaides A, Dimopoulos MA, Samantas E, et al. Gemcitabine and vinorelbine as second-line treatment in patients with metastatic breast cancer progressing after first-line taxane-based chemotherapy: a phase II study conducted by the Hellenic Cooperative Oncology Group. Ann Oncol. 2000;11(7): 873–875. 68. Stathopoulos GP, Rigatos SK, Pergantas N, et al. Phase II trial of biweekly administration of vinorelbine and Gemcitabine in pretreated advanced breast cancer. J Clin Oncol. 2002;20(1):37–41. 69. Haider K, Kornek GV, Kwasny W, et al. Treatment of advanced breast cancer with Gemcitabine and vinorelbine plus human granulocyte colonystimulating factor. Breast Cancer Res Treat. 1999;55(3):203–11. 70. Sanal SM, Gokmen E, Karabulut B, Sezgin C. Gemcitabine and vinorelbine combination in patients with metastatic breast cancer. Breast J. 2002; 8(3):171–6. 71. Gennatas A, Mouratidou D, Tsavaris N, et al. Gemcitabine in combination with vinorelbine for heavily pretreated advanced breast cancer. Proc Am Soc Clin Oncol. 2005;23(16):63S. [Abstract 741]. 1724 72. Gokmen AC, Sezgin CB, Karabulut B, et al. Gemcitabine plus vinorelbine as first-line treatment of metastatic breast cancer. Proc Am Soc Clin Oncol. 2005;23(16):85S. [Abstract 830]. 73. Basso U, Fratino L, Brunello A, et al. Which benefit from adding Gemcitabine to vinorelbine in elderly ( or = 70 years) women with metastatic breast cancer? Early interruption of a phase II study. Ann Oncol. 2007;18(1): 58–63. 74. Lombardi A, Magri MD, Crivellari D, et al. Combination chemotherapy with navelbine and continuous infusion of 5-Fluorouracil in metastatic, chemotherapy refractory breast cancer. Ann Oncol. 2000;11(8):1041–3. 75. Berruti A, Sperone P, Bottini A, et al. Phase II study of vinorelbine with protracted fluorouracil infusion as a second- or third-line approach for advanced breast cancer patients previously treated with anthracyclines. J Clin Oncol. 2000;18(19):3370–7. 76. Zambetti M, Mariani G, Demicheli R, et al. Five-day infusion fluorouracil plus vinorelbine in women with breast cancer previously treated with anthracyclines and paclitaxel. Breast Cancer Res Treat. 2000;62(2):135–9. 77. Zambelli A, Robustelli della Cuna FS, Ponchio L, et al. Four-day infusion of fluorouracil plus vinorelbine as salvage treatment of heavily pretreated metastatic breast cancer. Breast Cancer Res Treat. 2000;61(3):241–7. 78. Dieras V, Extra JM, Bellissant E, et al. Efficacy and tolerance of vinorelbine and fluorouracil combination as first-line chemotherapy of advanced breast cancer: results of a phase II study using a sequential group method. J Clin Oncol. 1996;14(12):3097–104. 79. Pienkowski T, Jagiello-Gruszfeld A. Five-day infusion of fluorouracil and vinorelbine for advanced breast cancer patients treated previously with anthracyclines. Int J Clin Pharmacol Res. 2001;21(3–4):111–7. 80. Vassilomanolakis M, Koumakis G, Barbounis V, et al. Vinorelbine and cisplatin in metastatic breast cancer patients previously treated with anthracyclines. Ann Oncol. 2000;11(9):1155–60. 81. Chehal A, Taher A, Khalil M, Shamseddine A. Cisplatin plus vinorelbine (PVn) as a salvage regimen for refractory breast cancer. Breast. 2004;13(5):421–4. 82. Shamseddine AI, Taher A, Dabaja B, et al. Combination cisplatin-vinorelbine for relapsed and chemotherapy-pretreated metastatic breast cancer. Am J Clin Oncol. 1999;22(3):298–302. 83. Mustacchi A, Muggia M, Milani S, et al. A phase II study of cisplatin and vinorelbine in patients with metastatic breast cancer. Ann Oncol. 2002;13(11):1730–6. 84. Estevez LG, Batista N, Sánchez-Rovira P, et al. Phase II study with the combination of Capecitabine (C) and vinorelbine (V) in metastatic breast cancer (MBC) previously treated with anthracyclines and taxanes. J Clin Oncol. 2004;22(14S):748 85. Ghosn M, Kattan J, Farhat F, et al. Phase II trial of Capecitabine and vinorelbine as first-line chemotherapy for metastatic breast cancer patients. Anticancer Res. 2006;26(3B):2451–6. 86. Nolè F, Crivellari D, Mattioli R, et al. Phase II study of an all-oral combination of vinorelbine with Capecitabine in patients with metastatic breast cancer. Cancer Chemother Pharmacol. 2009;64(4):673–80. 87. Delcambre C, Veyret C, Levy C, et al. A phase I/II study of Capecitabine combined with oral vinorelbine as first or second line therapy in locally advanced or metastatic breast cancer. Breast Cancer Res Treat. 2005;94:S67. (Abstract 1061). 88. Stuart N, Bishop JL, Johnson SRD, et al. Vinorelbine and Capecitabine (VX) for advanced breast cancer—a phase II study showing good activity and potential for further development. Proc Am Soc Clin Oncol. 2003;22. [Abstract 183] 89. Garrone O, Principe E, Occelli M, et al. A phase II study of Epirubicin, vinorelbine and cisplatin in advanced breast cancer. Anticancer Drugs. 2004;15(1):23–7. 90. Frasci A, D’Aiuto G, Comella P, et al. Cisplatin–Epirubicin–Paclitaxel weekly administration in advanced breast cancer: a phase I study of the Southern Italy Cooperative Oncology Group. Breast Cancer Res Treat. 1999;56(3): 239–52. 91. Nole F, Munzone E, Mandala M, et al. Vinorelbine, cisplatin and continuous infusion of 5-Fluorouracil (ViFuP) in metastatic breast cancer patients: a phase II study. Ann Oncol. 2001;12(1):95–100. Clinical Medicine: Therapeutics 2009:1 Vinorelbine in ABC 92. Esteban E, de Sande G, Puertas J, et al. A phase II trial of cyclophosphamide, Epirubicin and vinorelbine in the treatment of advanced breast cancer. Breast Cancer Res Treat. 2000;62(2):127–33. 93. Bonneterre J, Roché H, Monnier A, et al. Docetaxel vs. 5-Fluorouracil plus vinorelbine in metastatic breast cancer after anthracycline therapy failure. Br J Cancer. 2002;87(11):1210–5. 94. Namer M, Soler-Michel P, Turpin F, et al. Results of a phase III prospective, randomised trial, comparing Mitoxantrone and vinorelbine (MV) in combination with standard FAC/FEC in front-line therapy of metastatic breast cancer. Eur J Cancer. 2001;37(9):1132–40. 95. Blajman C, Balbiani L, Block J, et al. A prospective, randomized Phase III trial comparing combination chemotherapy with cyclophosphamide, Doxorubicin, and 5-Fluorouracil with vinorelbine plus Doxorubicin in the treatment of advanced breast carcinoma. Cancer. 1999;85(5):1091–7 96. Norris A, Pritchard KI, James K, et al. A phase III comparative study of vinorelbine combined with Doxorubicin versus Doxorubicin alone in disseminated metastatic/recurrent breast cancer: National Cancer Institute of Canada Clinical Trials Group Study MA8. J Clin Oncol. 2000;18(12): 2385–94. 97. Ejlertsen A, Mouridsen HT, Langkjer ST, et al. Phase III study of intravenous vinorelbine in combination with Epirubicin versus Epirubicin alone in patients with advanced breast cancer: a Scandinavian Breast Group Trial (SBG9403). J Clin Oncol. 2004;22(12):2313–20. 98. Pajk B, Cufer T, Canney P, et al. Anti-tumor activity of Capecitabine and vinorelbine in patients with anthracycline- and taxane-pretreated metastatic breast cancer: findings from the EORTC 10001 randomized phase II trial. Breast. 2008;17(2):180–5. 99. Debled M, Madranges M, Mertens C, et al. Retrospective analysis of chemotherapy choices and overall survival according to treatment in 96 patients 75 years old with metastatic breast cancer, Eur J Cancer. 2008;6:174. [Abst. 415]. 100. Verma S, Wong NS, Trudeau M, et al. Survival differences observed in metastatic breast cancer patients treated with Capecitabine when compared with vinorelbine after pretreatment with anthracycline and taxanes. Am J Clin Oncol. 2007;30:297–302. 101. Lee M, Wei W, Morandi N, Harris L. Capecitabine is associated with lower chemotherapy-related expenditures than those associated with vinorelbine in women with metastatic breast cancer. Cancer Res. 2009;69(Suppl):391s. [Abstract 6107]. 102. Sawada N, Fujimoto-Ouchi K, Ishikawa T, et al. Antitumour activity of combination therapy with Capecitabine plus vinorelbine, and Capecitabine plus Gemcitabine in human tumor xenograft models. Proc Am Assoc Cancer Res. 2002;43:1088a. [Abstr 5388]. 103. Elghazaly A, Tawfik H, Mahrous M, et al. Vinorelbine and Capecitabine combination as first-line treatment in patients with metastatic breast cancer: final results of a multicentric trial in Egypt. J Clin Oncol. 2008;26(15S):72s. [Abstract 1125]. 104. Ghosn M, Kattan J, Farhat F, et al. For the Cancer Research Group/ Collaborative Group (CRG/CG), Beirut–Lebanon. Sequential vinorelbineCapecitabine followed by Docetaxel in advanced breast cancer: longterm results of a pilot phase II trial. Cancer Chemother Pharmacol. 2008;62:11–8. 105. Köhler U, Luhn B, Kleine-TebbeA, et al. Capecitabine (C) and vinorelbine (V) in elderly patients (pts) with metastatic breast cancer (MBC) as 1st line treatment: a prospective multicentre phase II study of the NOGGO breast cancer study group, Breast Cancer Res Treat. 2006;100(Suppl 1):S285. [Abst 6089]. 106. Hess A, Koberle D, Thurlimann B, et al. Swiss Group for Clinical Cancer Research. Capecitabine and vinorelbine as first-line treatment in elderly patients (or =65 years) with metastatic breast cancer. A phase II trial (SAKK 25/99). Oncology. 2007;73:228–37. 107. Iodice GD, Aiuto G, Costanzo R, et al. Dose-escalated Capecitabine/ vinorelbine for elderly patients with metastatic breast cancer (MBC). A SICOG phase II study. Ann Oncol. 2006;17(Suppl 9):p. ix73. [Abstract 155P]. 108. Palumbo R, Bernardo A, Strada MR, et al. Activity and safety of vinorelbine and Capecitabine as first-line treatment in patients with metastatic breast cancer—a phase II trial, Eur J Cancer Suppl. 2008;6:177. [Abstract 425]. Clinical Medicine: Therapeutics 2009:1 109. Davis AJ, Brew S, Gebski VJ, et al. Multicenter phase II study of combination chemotherapy with Capecitabine and intravenous vinorelbine in patients with pretreated metastatic breast cancer. Asia–Pacific J Clin Oncol. 2007;3:37–43. 110. Orphanos G, Alexopoulos A, Ioannidis G, et al. High efficacy and low toxicity of the combination of vinorelbine and Capecitabine as second line treatment in metastatic breast cancer previously treated with taxanes and/or anthracyclines. Proc Am Soc Clin Oncol. 2006;24(18S): 10719. 111. Estévez LG, Batista N, Sánchez-Rovira P, et al. A phase II study of Capecitabine and vinorelbine in patients with metastatic breast cancer pretreated with anthracyclines and taxanes. Clin Breast Cancer. 2008;8: 149–54. 112. Lorusso V, Forcignano R, Leo S, et al. Vinorelbine plus Capecitabine in salvage therapy of breast cancer. Comparison of intravenous vs. oral administration of Vinorelbine. J Clin Oncol. 2008;26(15S):69s. [Abstract 1114]. 113. Xu B, Wu Q, Zhou M, et al. Capecitabine plus vinorelbine as secondline therapy in Chinese patients with metastatic breast cancer (MBC). Ann Oncol. 2006;17(Suppl 9):ix75. [Abstract 163P]. 114. Ahn JH, Kim SB, Kim TW, et al. Capecitabine and vinorelbine in patients with metastatic breast cancer previously treated with anthracycline and taxanes. J Korean Med Sci. 2004;19:547–53. 115. Jassem J, Kosmidis P, Ramlau R, et al. Oral vinorelbine in combination with cisplatin: a novel active regimen in advanced non-small-cell lung cancer. Ann Oncol. 2003;14(11):1634–9. 116. Marty M, Fumoleau P, Adenis A, et al. Oral vinorelbine pharmacokinetics and absolute bioavailability study in patients with solid tumors. Ann Oncol. 2001;12(11):1643–9. 117. Lush RM, McCune JS, Tetteh L, et al. The absolute bioavailability of oral vinorelbine in patients with solid tumors. Cancer Chemother Pharmacol. 2005;56:578–84. 118. Depierre A, Freyer G, Jassem J, et al. Oral vinorelbine: feasibility and safety profile. Ann Oncol. 2001;12(12):1677–81. 119. Freyer G, Delozier T, Lichinister M, et al. Phase II study of oral vinorelbine in first-line advanced breast cancer chemotherapy. J Clin Oncol. 2003; 21(1):35–40. 120. Baweja M, Suman VJ, Fitch TR, et al. Phase II trial of oral vinorelbine for the treatment of metastatic breast cancer in patients 65 years of age an NCCTG study. Ann Oncol. 2006;17:623–9. 121. Lotz A, Husseini F, Finck M, et al. French experience of patient management when receiving oral vinorelbine chemotherapy (NVBO) for metastatic breast cancer: Final results of a prospective observational survey on practices. J Clin Oncol. 2009;(Suppl 27). [Abstr e12013]. 122. Gil-Delgado M, Rocher M, Boostandoost E, Khayat D. First step of oral vinorelbine and Capecitabine combination in advanced breast cancer patients: Feasibility study. J Clin Oncol. 2008;26:1135(15S). 123. Tubiana-Mathieu N, Bougnoux P, Becquart D, et al. All-oral combination of oral vinorelbine and Capecitabine as first-line chemotherapy in HER2negative metastatic breast cancer: an International Phase II Trial. Br J Cancer. 2009;101(2):232–7. 124. Addeo R, Faiola V, Cennamo G, et al. A novel metronomic schedule of oral vinorelbine for the treatment of metastatic breast cancer in elderly patients: A phase II trial. J Clin Oncol. 2009;27:15s. [Abstr 1085]. 125. Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J Clin Oncol. 1999;17(9):2639–48. 126. Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol. 2002;20(3):719–26. 127. Pegram MD, Konecny GE, O’Callaghan C, et al. Rational combinations of trastuzumab with chemotherapeutic drugs used in the treatment of breast cancer. J Natl Cancer Inst. 2004;96:739–49. 128. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–92. 1725 Brunello et al 129. Kaufman PA, Schwartz G, Dragnev K, et al. Phase I trial of Herceptin and Navelbine for patients with HER-2/neu (+) advanced breast cancer. In: Poster 431 presented at the 25th San Antonio Breast Cancer Symposium San Antonio TX U S A. 2002 December. 11–14. 130. Burstein HJ, Keshaviah A, Baron A, et al. Trastuzumab plus vinorelbine or taxane chemotherapy for HER2-overexpressing metastatic breast cancer:the trastuzumab and vinorelbine or taxane study. Cancer. 2007; 110(5):965–72. 131. Jahanzeb M, Mortimer JE, Yunus F, et al. Phase II trial of weekly vinorelbine and trastuzumab as first-line therapy in patients with HER2+ metastatic breast cancer. Oncologist. 2002;7:410–7. 132. Bernardo G, Palumbo R, Bernardo A, et al. Final results of phase II study of weekly trastuzumab and vinorelbine in chemonaive patients with HER2-overexpressing metastatic breast cancer. Proc Am Soc Clin Oncol. 2004;23:59. [Abstr 731]. 133. Burstein HJ, Harris LN, Marcom PK, et al. Trastuzumab and vinorelbine as first-line therapy for HER2-overexpressing metastatic breast cancer: multicenter phase II trial with clinical outcomes, analysis of serum tumor markers as predictive factors, and cardiac surveillance algorithm. J Clin Oncol. 2003;21:2889–95. 134. Chan A, Martin M, Untch M, et al. Vinorelbine plus trastuzumab combination as first-line therapy for HER2-positive metastatic breast cancer patients: an international phase II trial. Br J Cancer. 2006;95:788–93. 135. Bayo-Callero JL, Mayordomo JI, Sanchez-Rovira P, et al. A phase II study of weekly vinorelbine and trastuzumab in patients with HER2-positive metastatic breast cancer. Clin Breast Cancer. 2008;8(3):264–8. 136. Porta VG, Martin M, Gil M, et al. Evaluation of Vinorelbine (N) and trastuzumab (H) as first-line therapy for patients (pts) with HER2-positive metastatic breast cancer (HER2 + MBC): impact on clinical response and cardiac function. ASCO annual meeting proceedings (post-meeting edition). J Clin Oncol. 2004;22(14S):636. 137. Schilling G, Bruweleit M, Harbeck N, et al. Phase II trial of vinorelbine and trastuzumab in patients with HER2-positive metastatic breast cancer. A prospective, open label, non-controlled, multicenter phase II trial. Invest New Drugs. 2009;27(2):166–72. 138. Franquesa RM, Centelles M, Villadiego K, et al. A multicenter study of trastuzumab (H) and vinorelbine (N) as first and second line therapy for patients (pts) with HER2-positive metastatic breast cancer (HER2 + MBC). J Clin Oncol. 2005;23:94s. [Abstr 868]. 139. Brunello A, Monfardini S, Crivellari D, et al. Multicenter analysis of activity and safety of trastuzumab plus chemotherapy in advanced breast cancer in elderly women (70 years). J Clin Oncol. 2008;26 (Suppl). [Abstr 1096]. 140. Papaldo P, Fabi A, Ferretti G, et al. A phase II study on metastatic breast cancer patients treated with weekly vinorelbine with or without trastuzumab according to HER2 expression: changing the natural history of HER2-positive disease. Ann Oncol. 2006;17:630–6. 141. Lal A, Alidina A. Interim analysis of a phase II study of biochemotherapy in metastatic breast cancer (MBC). Eur J Cancer. 2005;3(Suppl):131. [Abstr 470]. 142. De Maio E, Pacilio C, Gravina A, et al. A single-centre phase 2 study of vinorelbine plus 3-weekly trastuzumab in metastatic breast cancer. Ann Oncol. 2004;15(Suppl 3):37. [Abstr 139P]. 143. Bartsch R, Wenzel C, Altorjai G, et al. Results from an observational trial with oral vinorelbine and trastuzumab in advanced breast cancer. Breast Cancer Res Treat. 2007;102(3):375–81. 144. Laessig D, Vehling-Kaiser U, Harich HD, et al. Oral and intravenous vinorelbine plus trastuzumab for 1st-line treatment of HER2-overexpressing metastatic breast cancer (MBC). A trial of the german AIO breast cancer group. J Clin Oncol. 2008;26(May 20 Suppl). [Abstr 1061]. 145. Estevez LG, Tusquets I, Munoz M, et al. Advanced breast cancer: Chemotherapy phase III trials that change a standard. Anti Cancer Drugs. 2007;18:843–59 Publish with Libertas Academica and every scientist working in your field can read your article “I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.” “The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I’ve never had such complete communication with a journal.” “LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.” Your paper will be: • Available to your entire community free of charge • Fairly and quickly peer reviewed • Yours! You retain copyright http://www.la-press.com 1726 Clinical Medicine: Therapeutics 2009:1