Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
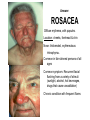
“THE SKIN SHOW” Aging Dermatology and Disease Module #3 Ed Vandenberg, MD, CMD Geriatric Section OVAMC & Section of Geriatrics 981320 UNMC Omaha, NE 68198-1320 [email protected] Web: geriatrics.unmc.edu 402-559-7512 All photos were reprinted with permission from the American Academy of Dermatology. All rights reserved. Slides adapted with permission from GRS 5th edition: Dermatologic diseases and disorders PROCESS Series of 4 modules and questions on Etiologies, Evaluation, & Management Step #1 Power point module with voice overlay Step #2 Case-based question and answer Step #3 Proceed to additional modules or take a break Objectives Upon completion the learner will be able to; 1) List the normal age related skin changes 2) Identify and treat the common skin disorders of aging 3) Identify malignant versus non malignant skin conditions in aged What’s this? Eighty-year-old female with persistent “itchy” feeling in legs. Answer: XEROSIS Dry, erythematous, scaly, fissured, most commonly on extremities Diagnosis: history, associated with generalize dry skin ( “sand paper”). Causes: reduced water content & reduced epidermal lipid production Risk factors: Decreased skin hydration from low humidity, diuretics, excessive bathing, hot water, harsh soaps, incomplete drying Differential diagnosis: Irritant contact dermatitis Eczemas Statis dermatitis Psoriasis Dermatophyte TREATMENT OF XEROSIS • Reduce bathing frequency, soap to “critical” areas only • Moisturizing agents containing lactic acid or α-hydroxy acids • Tepid, not hot, showers • Mild topical corticosteroids episodically for irritation or inflammation • Emollients immediately after bathing when skin moist • Use moisturizer instead of itching • Increase humidity and fluid intake Avoid: Bath oils Systemic anti-pruritics NEURODERMATITIS Alias: lichen simplex chronicus • Chronic, pruritic conditions of unclear cause • Severe, paroxysmal, before sleep • Most common: women, Asian • signs of chronic scratching • Location: lower extremeties • Exclude irritant or allergic contact dermatitis • Treatment: • Potent topical corticosteroids (often under occlusion) • Emollients • Behavioral modification Avoid: systemic anti-pruritics What’s this? Seventy-seven-year-old female, non pruritic, slowly progressive eruption, surrounding edema. Answer: Stasis dermatitis Location: lower extremity, associated with venous insufficiency Prevention: leg elevation, compression stockings, muscle contraction, moisturize skin Venous insufficiency ulcers: Debride: (wet-dry, Hibclens whirlpool, hydrocolloid nonadhesive) Heal: Unna boot, change no more than 2x/wk, Correct associated factors: CHF, malnutrition, constricting garments, Evaluate arterial flow (ABI) What’s in the scalp? Answer: SEBORRHEIC DERMATITIS Common chronic dermatitis Erythema and greasy-looking scales Typical locations: hairline, nasolabial fold, midline chest Dandruff is often a precursor More common in men Cause unclear: normal yeast flora may cause inflammation TREATMENT OF SEBORRHEIC DERMATITIS • Can be suppressed but not cured • Mild topical corticosteroids useful for acute forms (1% to 2% hydrocortisone) • Once controlled, maintenance with medicated shampoos that act against yeast, eg, selenium sulfide, ketoconazole, tar shampoos What’s this? Sorry, no clues for you!! Answer: Bullous Pemphigoid Tense, large, clear fluid or hemorrhagic filled bullaeon an erythematous base were seen on the trunk and extremities. Bullae rupture and leave a scab with crusting. • • Autoimmune Most often in adults in 60s and 70s • Condition may last from months to years, but often is self-limited • Diagnosis by biopsy and immunofluorescence TREATMENT OF BULLOUS PEMPHIGOID • Dependent on severity • For localized disease, use topical corticosteroids • For more extensive disease, use • Systemic corticosteroids • Other immunosuppressant (azathioprine or cyclophosphamide) • Tetracycline and niacinamide combination therapy What’s this? Answer: PSORIASIS Well-demarcated, erythematous papules & plaques with silverywhite scales. May have pustular component. Location: knees, elbows, scalp, back genitalia, intergluteal folds, nails Exacerbated by: trauma (physical or psychological), inflammation of skin, low humidity, sunburn, drugs: digoxin, clonidine, lithium, propranolol, antimalarial drugs Differential diagnosis: Tinea corporis Pityriasis rosea Nummular eczema Seborrheic dermatitis TREATMENT OF PSORIASIS • Topical treatments: • may control mild disease but may be irritating or messy • include corticosteroids, vitamin D derivatives (calcipotriene), topical retinoids (tazarotene), salicylic acid, tar compounds • long-term use of topical corticosteroids is limited by cutaneous atrophy and tachyphylaxis TREATMENT OF PSORIASIS • Systemic treatment: • if no response to topicals • phototherapy • immunosuppressive agents (cyclosporine, methotrexate) • UV therapy: • can be used with topical therapy • PUVA (psoralen with UVA light) and UVB • Evaluate risks, benefits of all therapies for older adults What’s this? Answer: ROSACEA Diffuse erythema, with papules. Location: cheeks, forehead & chin Nose: thickended, erythematous rhinophyma. Common in fair-skinned persons of all ages Common symptom: Recurrent facial flushing from a variety of stimuli (sunlight, alcohol, hot beverages, drugs that cause vasodilation) Chronic condition with frequent flares TREATMENT OF ROSACEA Avoid skin irritants, strong soaps Reduce sun exposure: use sunscreens For moderate to severe flares: oral antibiotics (tetracyclines, eg, doxycycline, minocycline) or erythromycin For mild cases and maintenance: topical antibiotics (erythromycin, clindamycin, metronidazole) TREATMENT OF SEVERE ROSACEA • Severe or refractory rosacea: Oral isotretinoin • Erythema and telangiectasias: • Difficult to treat • Lasers provide option to reduce redness and improve cosmetic appearance • Rhinophyma: • Less common • Can be treated with surgical excision or CO2 laser ablation The End of “Skin Show” Module Three Post-test • A 78-year-old man has greasy, yellow scales over the central chest, nasolabial folds, scalp, eyebrows, and in the ears. The rash developed last year, after the patient was placed in a skilled nursing facility following a stroke. Which of the following is the most likely diagnosis? Which of the following is the most likely diagnosis? A. Actinic keratoses B. Seborrheic dermatitis C. Psoriasis D. Scabies E. Eczema Used with permission from: Murphy JB, et. al. Case Based Geriatrics Review: 500 Questions and Critiques from the Geriatric Review Syllabus. AGS 2002 New York, NY. Answer:B. Seborrheic dermatitis Seborrheic dermatitis is a chronic, superficial, inflammatory process affecting the hair- bearing areas of the body. It has been associated with neurologic conditions such as Parkinson’s disease and as a sequela to stroke with motor function impairment. It also affects approximately one third of patients with AIDS. It is thought to be a reaction to the yeast Pityrosporum ovale. Therapeutic options include nonprescription ketoconazole and selenium sulfide shampoos, as well as 1.0% to 2.5% hydrocortisone cream. • Actinic keratoses are precancerous skin lesions that are erythematous, with a rough surface. They usually are found in sun-exposed areas. Typical psoriatic lesions are erythematous plaques with a silvery-white, micaceous, firmly adherent scale on extensor surfaces. Scabies infestation usually is accompanied by severe itching. Erythematous excoriated papules can be found on inspection of the nipples, axillae, genitalia, wrists, and fingers. Burrowing may be visible, and a black dot, the causative mite, can be seen. The greasy appearance and distribution (chest and ears) of this rash make eczema very unlikely. end