Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Adipose tissue wikipedia , lookup
Body mass index wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Human nutrition wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Thrifty gene hypothesis wikipedia , lookup
Obesity and the environment wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
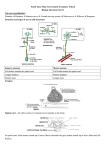
Chous & Richer Obesity Related Eye Disease and Patient Communication American Pie Meets American Idle: Nutritional and Nutraceutical Management of Obesity Related Eye Disease A. Paul Chous, MA, OD, FAAO Stuart P. Richer, OD, PhD, FAAO A. Paul Chous, MA, OD, FAAO 25300 Lake Wilderness CC Drive SE Maple Valley, WA 98038 [email protected] Stuart Richer, OD, PhD, FAAO Eye Clinic 112e DVA Medical Center North Chicago, IL 60064 [email protected] ABSTRACT Surveys indicate that patients place high value on Primary Care Providers who discuss lifestyle issues such as weight maintenance, exercise and supplementation. Given the obesity and diabetes epidemic, ODs have a Public Health responsibility to proactively address these issues. We discuss the biologic rationale for specific macronutrients, micronutrients and exercise with respect to weight maintenance and loss, insulin resistance, inflammation, oxidative stress, and obesity related cardiovascular and eye disease. Scientific rationale and effective Patient-Doctor communication are stressed, with patient recommendations integrated within the presentation and handout. I. Course Considerations a. Why is obesity associated with ophthalmic (and systemic) disease? b. Clinical Entities c. Epidemiology and Definitions d. Biological Rationale for Specific Macronutrients 1. Dietary Fat 2. Dietary Carbohydrate & Fiber Carbohydrate Metabolism: a link between AMD & Diabetes 3. Dietary Protein e. Biological Rationale for Specific Micronutrient and Nutraceutical Supplements h. Some Recommendations 1. Dietary 2. Supplementation 3. Patient communication i. Conclusion 1 Chous & Richer Obesity Related Eye Disease and Patient Communication II. Why is obesity associated with ophthalmic (and systemic) disease? An Unholy Triumvirate: Inflammation, Hypertension and Hypoxia a. Inflammation, Insulin Resistance and Oxidative stress (see Figure 1) Inflammation - Fat cells are endocrine cells, secreting hormones that regulate insulin sensitivity and satiety (‘fullness’) & inflammatory proteins - Visceral fat surrounding internal organs, in particular, worsens insulin sensitivity and increases appetite leading to a vicious cycle of high caloric intake, insulin resistance and increasing adiposity - visceral and subcutaneous fat are associated with elevated markers of inflammation, including C-reactive protein (CRP), intracellular adhesion molecules (ICAMs) and fibrinogen CRP destabilizes atherosclerotic plaques ICAMs cause white blood cell adhesion to blood vessel walls Fibrinogen promotes formation of platelet clots inflammation causes endothelial dysfunction and increased insulin resistance, leading to vascular diseases, including eye disease Insulin Resistance - Obesity without inflammation does not cause insulin resistance - Some tissues do NOT require insulin to get glucose inside of cells: liver kidney aorta retina - insulin resistance leads to high levels of intracellular glucose within these insulin independent tissues - mitochondrial exposure to high levels of glucose causes over-production of reactive oxygen species (ROS) - in addition, visceral fat mobilizes serum free fatty acids (FFAs) that are also oxidized by mitochondria within vascular endothelium to generate ROS Oxidative Stress - increased ROS lead to vascular complications via four distinct biochemical pathways 1. 2. 3. 4. Polyol Hexosamine Advanced Glycation Endproducts Protein Kinase C 2 Chous & Richer Obesity Related Eye Disease and Patient Communication - Free iron is locally toxic to body tissues, which have developed a host of serologic mechanisms to capture and sequester iron - Iron overload may result from metabolic defects, diet or specific genes - Iron metabolism is adversely affected by hyperglycemia, leading to inflammation, insulin resistance and oxidative stress in type 2 diabetes and the metabolic syndrome - Stores of the iron-sequestering plasma protein, haptoglobin (Hp) are elevated in diabetes and Hp genotype appears to confer increased/decreased risk of diabetic retinopathy in T1DM and cardiovascular events in T2DM* * Haptoglobin PCR genotyping is available through ARUP Laboratories @ http://www.aruplab.com/guides/ug/tests/0040116.jsp Iron Overload Metabolic Defects Inflammatory Cytokines Figure 1 TNF-a PAI-1 ICAMs CRP Haptoglobin Genotype Diet Free Fatty Acids Adipokines Obesity Visceral Fat Insulin Resistance Increased Oxidative Stress Skeletal muscle Liver Hypothalamus Hunger & Increased Caloric Intake Blunted Satiety Receptors Disease 3 Chous & Richer Obesity Related Eye Disease and Patient Communication b. Hypertension - Obesity and body mass index (BMI) are clear and continuous risk factors for HTN - risk of hypertension increases linearly with VAT - weight loss clearly results in reduced BP in large clinical trials - HTN is a definitive risk factor for myriad posterior segment diseases (e.g. hypertensive retinopathy, retinal vascular occlusions, diabetic retinopathy, AION) c. Obstructive Sleep Apnea Syndrome (OSAS) - increased BMI and type 2 diabetes are the two most common, independent systemic risk factors associated with OSAS - OSAS activates the renin-angiotensin system, increasing blood pressure - OSAS causes hypoxic stress, endothelial dysfunction, increased platelet aggregation and adhesion of inflammatory proteins that significantly increase the risk of vascular disease, including eye disease (glaucoma, NAION, pseudotumor cerebri) III. Clinical Entities a. Cataract – risk of Cataract is 30% to 40% higher in patients with Metabolic Syndrome - risk of posterior subcapsular cataract is 4x greater for women with diabetes and 2x greater for women with BMI > 30 (versus <25) and increased waist circumference (>89cm versus <80cm) - BMI > 30 associated with increased risk of cortical cat and PSC in the Blue Mountains Eye Study b. Glaucoma, NAION, Floppy Eyelid Syndrome (FES) and pseudotumor cerebri (PTC) are each associated with OSAS and obesity - higher IOP is associated with obesity and metabolic syndrome - the prevalence of glaucoma in patients with OSAS is estimated to be 27% - multiple studies show that OSAS is the most frequent disorder associated with NAION - 25% of patients with OSAS have FES - 15-40% of patients with PTC have OSAS c. Macular Degeneration - risk of advanced AMD higher with diabetes and obesity (5% increase in risk for every 1kg/m2 increase in BMI) - AREDS showed that greater BMI doubled risk of Neovascular-AMD - Waist circumference and diabetes were related to lower macular pigment optical denisity (MPOD) in the Women’s Health Initiative 4 Chous & Richer Obesity Related Eye Disease and Patient Communication d. Diabetic Retinopathy - Obesity and weight gain are the primary risk factor for type 2 diabetes mellitus (T2DM) - BMI and older age best screen for pre-diabetes (50 million Americans) - Marked obesity increases risk of retinopathy in T2DM - 7% of patients with prediabetes have diabetic retinopathy - You don’t develop diabetic retinopathy if you don’t have diabetes! - The risk of developing retinal microvascular disease is directly and continuously related to increasing levels of both insulin resistance and blood glucose e. Hypertensive Retinopathy/Venous Occlusive Disease - The risk of retinal venous occlusion and arterial emboli is 3.8 fold higher for patients with a BMI > 30 - Risk of CRVO highest in HTN, DM and POAG patients - Risk of BRVO is highest if the BMI @ 20 years of age > 25 km/m2, preexisting cardiovascular disease, HTN and/or glaucoma IV. Epidemiology & Definitions of Overweight/Obesity - In 2005, 60.5% of Americans were overweight, 23% were obese, and 3% were morbidly obese Obesity by Gender: males 24.2% and females 23.5% Obesity by Age: 18% ages 18-29 and 30% ages 50-59 Obesity by Race: 34% non-hispanic blacks versus 23% non-hispanic whites Classic Definitions of Overweight & Obesity by Body Mass Index (BMI): BMI = Weight (pounds)/Height (inches)2 x 703 ( kg/m2 ) BMI = Weight (kg)/Height (m) 2 BMI > 25 BMI > 30 BMI > 35 BMI > 40 overweight obese severely obese morbidly obese Adults For children & teens, overweight > 85th percentile; obese > 95th percentile: Other Measures of Obesity: -Abdominal Adiposity - Waist circumference > 102 cm (40 inches) in men - Waist circumference > 88 cm (35 inches) in women (Slightly higher for non-Europeans) 5 Chous & Richer Obesity Related Eye Disease and Patient Communication - Waist to Hip Ratio - W/H > 0.8 for women and > 1.0 for men Increased risk of cardiovascular disease - Magnetic Resonance Imaging (MRI) - visceral adipose tissue (VAT) versus subcutaneous adipose tissue (SCAT) - VAT > SCAT predicted the risk of Metabolic Syndrome in the Framingham Heart Study - VAT may explain the ‘paradox’ of the thin patient with type 2 diabetes V. Biological Rationale for Specific Macronutrients Dietary Fat - Saturated Fat: high intake unquestionably linked to increased cardiovascular risk & increased inflammation SFA intake > 10% of calories increases insulin resistance and LDL-C However, SFA < 7% of total calories has little effect on LDL-C and significantly decreases protective HDL-C, especially in insulin resistant patients - Trans Fats consist of multiple isomers have varying effects on metabolism trans-10, cis-12 conjugated linoleic acid from hydrogenated oils (animal fat, margarine, palm oil, coconut oil) significantly increases inflammation and cardiovascular risk and induces endothelial dysfunction - Monounsaturated fatty acids - MUFA (olive oil, nuts avocadoes) decrease triglycerides, LDL-C and oxidized LDL without decreasing HDL MUFA decrease soluble inflammatory adhesion molecules and improve endothelial function The high arginine content of nuts (especially walnuts) decreases C-reactive protein levels - - Polyunsaturated fatty acids – PUFA include n-6 and n-3 subtypes Humans lack the enzymes necessary to produce two essential fatty acids: the n-3 PUFA, -linolenic acid and the n-6 PUFA, linoleic acid N-3 PUFA tend to decrease inflammation, whereas n-6 PUFA increase inflammation The rate of heart disease declines when PUFA are substituted for SFA The n-3 PUFA, alpha-linolenic acid (found in flax seed, canola, walnut & linseed oils) is a precursor to the long-chain n-3 fatty acids DHA & EPA but may not be sufficiently synthesized in optimal quantities, so higher dietary intake of DHA & EPA are recommended (high concentrations in cold water, oily fish like salmon, sardines and herring, as well as dietary fish oil) 6 Chous & Richer Obesity Related Eye Disease and Patient Communication - - - - DHA and EPA decrease plasma triglycerides, FFAs, glucose and insulin, reduce peripheral insulin resistance, and decrease visceral fat and concomitant production of inflammatory cytokines The ratio of n-6 to n-3 PUFA appears to determine effects on lipid and inflammatory indices, and a 2:1 to 6:1 ratio has been suggested to maximize cardiovascular benefit; the ratio in the typical American diet is > 15:1 Low fat diets may drive increased consumption of carbohydrate and worsening insulin resistance energy-restricted low-fat and low-carbohydrate diets both significantly decreased biomarkers of inflammation, suggesting that weight loss may be the driving force underlying reductions in inflammatory biomarkers modest weight loss (<5%) preferentially decreases visceral fat, resulting in improved insulin sensitivity and reduction in the risk of type 2 diabetes Take Home Message on Fats for Patients: keep SFA between 7% and 10% of calories eliminate trans fats increase consumption off MUFA increase consumption of n-3 PUFA, including DHA and EPA caloric restriction and moderate physical activity reduces weight, inflammation & blood pressure Dietary Carbohydrate & Fiber - - - - Refined Carbohydrates and Simple Sugars: high consumption of the simple sugars -fructose, glucose and sucrose – promotes release of free fatty acids and increased intravascular oxidative stress high dietary intake of refined carbohydrates leads to rapid elevation of blood glucose and insulin, reduces nitric oxide and impairs endothelium-dependent vasodilation, increasing risk of vascular occlusion short-term acute hyperglycemia may increase circulating levels of free radicals and proinflammatory cytokines, such as IL-6, IL-18, and TNF-alpha by its mass effect, post-prandial hyperglycemia increases cellular glucose uptake and metabolism within insulin independent tissues, resulting in production of ROS and vascular insult The Case for Fiber, Fruits & Vegetables: high fiber, low carbohydrate diet results in increased insulin sensitivity and reduced inflammation increased dietary fiber is associated with a significant 6mm/4mm reduction in blood pressure in hypertensive patients, based on meta-analysis 7 Chous & Richer Obesity Related Eye Disease and Patient Communication - - - - addition of psyllium fiber and guar gum both reduced BMI, fasting blood glucose and LDL-C in hypertensive, overweight subjects, but only psyllium resulted in significant decreases in triglycerides, systolic and diastolic blood pressure notwithstanding their effects on blood glucose, diets with high intake of fruits and vegetables are consistently associated with lower cardiovascular risk The case for alcohol – a derivative of fermentable carbohydrate moderate intake of all alcoholic beverages (beer, wine and liquor) lowers hs-CRP and is associated with a lower risk of fatal and nonfatal cardiovascular disease 0.5 to 1 drink per day confers cardiovascular protection primarily by increasing insulin sensitivity and HDL-C Resveratrol, a polyphenolic component of red grapes and wine, enhances insulin sensitivity by activating the enzyme SIRT1 and has been shown to extend lifespan in invertebrates and mammals unrelated, super-potent SIRT1 activators have been recently identified that improve glucose homeostasis in adipose, muscle and liver tissue Carbohydrate Metabolism: A Link between Diabetes and AMD a. glycemic index (GI) refers to the incremental area under the blood glucose response curve of a 50g carbohydrate portion of a test food expressed as a percent of the response to the same amount of carbohydrate from a standard food (white bread or glucose) taken by the same subject over a two hour period b. glycemic load (GL) considers blood glucose response to any given food in light of the consumed portion size, and is the product of the glycemic index times consumed carbohydrate in grams, divided by 100. c. criticisms - many foods have prolonged glycemic effects (up to ten hours) - there are wide variations in glycemic response among normal individuals - GI measurements represent averages amongst normals, not those with decreased insulin sensitivity, IGT and/or diabetes, so the results may not be generalizable d. what evidence is there for the utility of GI and/or GL? - high dietary GL (dGL) increases CRP & triglycerides and lowers HDL-C - dGL predicts cardiovascular risk in obese patients - multiple trials show that low GI foods delay hunger and reduce caloric intake and short term studies suggest that low GL diets result in significantly more weight loss that high GL diets - higher dietary GI (dGI) increases risk of advanced AMD ( large drusen, geographic atrophy, CNVM) and the risk of developing T2DM - long-term clinical trials are lacking at this time, but basic science strongly suggests that a lower dGI/dGL decreases inflammation & insulin resistance - the most comprehensive listing of GI/GL may be accessed at http://www.ajcn.org/cgi/content/full/76/1/5/T1 8 Chous & Richer Obesity Related Eye Disease and Patient Communication Take Home Message on Carbohydrates & Fiber for Patients decrease intake of refined carbohydrate reduce & diffuse the glycemic load (smaller, more frequent meals) eat a variety of lower GI/GL fruits & vegetables and increase intake of dietary fiber to > 25 grams/day consider moderate alcohol consumption (1 drink QOD), preferably red wine Dietary Protein - - - both reduced calorie high protein (HP) and reduced calorie high carbohydrate (HC) diets result in significant weight loss and improve all components of Metabolic Syndrome (save HDL-C), but HP better decreased blood pressure and triglycerides Increasing dietary protein results in heightened satiety and weight loss possibly by triggering release of satiety enhancing gut hormones, as well as by increasing thermogenesis Dietary protein may also, however, promote insulin resistance and hyperglycemia, as well as contribute to overt kidney disease in the at-risk, obese population - An increasing body of literature suggests that soy protein may have a beneficial role in obesity - soy reduces total cholesterol (TC), LDL-C and triglycerides by reducing intestinal cholesterol absorption and hepatic cholesterol synthesis - soy appears to reduce production of free fatty acids and improve peripheral insulin sensitivity - Both dietary iron overload (high consumption of red meat) and defects of iron metabolism (as a function of haptoglobin genotype) are common in DM Iron overload has been implicated in the pathogenesis of AMD, whereas haptoglobin genotype has not - Take Home Message on Protein for Patients increased protein consumption decreases appetite and assists in weight loss, but these benefits must be weighed against the possibility of kidney dysfunction and increased insulin resistance 9 Chous & Richer Obesity Related Eye Disease and Patient Communication increased consumption of fatty fish and soy protein preferred avoid red meat VI. Biological Rationale for Specific Micronutrient and Nutraceutical Supplements reduce inflammation, improve insulin sensitivity, block generation and/or harmful effects of reactive oxygen species (see below) VII. Recommendations For Overweight and Obese Patients Dietary: eat an anti-inflammatory, calorie restricted diet consisting of a variety of low glycemic load fruits and vegetables, nuts, whole grains and plentiful fiber, favoring cold water, fatty fish and soy protein, with minimal regular alcohol consumption (red wine) The so-called “Mediterranean Diet” fulfills all of these criteria In the Nurses’ Health Study, Mediterranean diet was associated with lower concentrations of biomarkers of inflammation and endothelial dysfunction The Lyon Diet Heart Study showed a 70% reduction in heart attack and unstable angina with the Mediterranean Diet, whereas the European Prospective Investigation into Cancer and Nutrition study (EPIC) showed an inverse correlation between greater adherence to a Mediterranean-style diet and death Though few studies evaluate the ocular effects of a Mediterranean Diet, one study showed the lowest incidence of AMD in a rural Italian farming community. The strong connection between cardiovascular and obesityrelated ocular disease suggests a probable benefit Supplements: basic and clinical science supports the position that overweight and obese patients, as well as patients with any degree of insulin resistance, may benefit from supplementation. However there is no consensus, beyond fish oil supplementation, even in the integrative medicine community, about what constitutes comprehensive supplementation. * Fish oil – prevents diabetic arrythmias, MIs, reduces inflammation & triglycerides, and lowers C reactive protein. Various herbs listed below are also used among different world cultures where medical care is scant or non-existent. As for conventional anti-oxidant supplements, although there seems to be scant evidence of supplement use and ocular outcomes, there are a plethora of small studies and testimonials suggesting the benefits of various nutrients. Those at high risk of developing advanced AMD reduced that risk by 25% with an antioxidant supplement plus zinc, AND….. Age-Related Eye Disease Study II (AREDS II) will further evaluate the ocular benefits of lutein, zeaxanthin and n-3 PUFA (accessed 11/28/07 at http://www.nei.nih.gov/neitrials/viewStudyWeb.aspx?id=120) 10 Chous & Richer Obesity Related Eye Disease and Patient Communication Andrew Weil’s Top 4 Supplement recommendations • • • • GTF (glucose tolerance factor) chromium (picolinate) – 200 mcg – 1000mcg / day – Helps insulin transport glucose into cells Alpha Lipoic Acid – 600 – 1200 mg the R- isoform of ALA (R-ALA) is preferentially distributed to mitochondria and is unique among anti-oxidants because it is regenerated by glycolytic flux (a so-called ‘catalytic antioxidant’) rather than being consumed on a molecule-for-molecule basis by free radical oxidants, making it an ideal candidate for neutralizing ROS generated by mitochondria – Helps insulin transport glucose into cells – Inhibits glycosylated attachment of sugar to protein – Maintains eye and nerve health (↓peripheral neuropathy) – Reduces diabetic cataract • Also Acetyl-L-Carnosine (2 recent studies)- 500 & 1000mg Magnesium (citrate or taurate) – 400mg – Insulin production COQ10- 100 mg – Maintains cardiac function – Protects against high dose statins, AMD & Parkinson’s Dz – 31% drop in blood sugar in 1 study Bills Sardi’s www.KnowledgeofHealth.com Supplement Recommendations IP6 phytate* (Rice bran, chia seed powder or flaxseed meal) – binds FE++ Resveratrol – chief source is red wine (www.longevinex.com) Quercetin – onions, apples - prevents sorbitol BV damage Taurine – supports cellular membrane structure Additional Supplements: • • • Vitamin E (natural d-alpha & mixed isomers) – Lipid soluble antioxidant; against heart disease & nerve damage Vitamin C – 500 mg – 2500 mg serially dosed – BV health & ↓ insulin resistance, cataract & cancer with multiple MOAs Flavonoids @70% of vitamin C dose- normalize blood vessel permeability and reduce hyperglycemia. – Bilberry (160-320 mg 25% stnd xtract)– Genistein blocks protein tyrosine kinase and has been shown to prevent vascular leakage in an animal model of diabetic retinopathy – Ginkgo Biloba – Pycnogenol 11 Chous & Richer Obesity Related Eye Disease and Patient Communication • • • • • • • improves fasting glucose, post-prandial glucose and HbA1c in T2DM reduces inflammatory biomarkers associated with obesity and appears to retard vascular leakage in diabetic retinopathy Lutein (6-20 mg) Theoretically Protects the macula and circulation i.e AREDS 2 study Improved visual function (LAST, LAST II and multiple subsequent studies) Low levels associated with insulin resistance B Vitamin Complex – B1 Thiamin or benfotiamine – for carbohydrate metabolism benfotiamine is a fat soluble analog of B1 totally prevented diabetic retinopathy in an animal model by blocking activity in the polyol, hexosamine, AGE and PKC pathways – B3 Niacin – to increase HDL cholesterol – B6 Pyridoxine(s) – for protein metabolism – Folic acid – for healing; ↓homocysteine – B12 Methylcarbolamine –for improved nerve cell function – Biotin – for fatty acid metabolism Zn/Cu & manganese – immune system, healing; cofactor for SOD Vanadyl Sulfate – mimics the action of insulin Selenium – cofactor for GSH peroxidase, a major antioxidant enzyme GLA/ALA – additional anti-inflammatory essential fatty acids Curcumin –multiple MOAs, improves response to insulin Herbs (various ethnic groups and cultures) • • • • • • • • Gymnema Sylvestre (leaf extract from India) – Improve insulin sensitivity w/o hypoglycemia – Beta Fast GXR ® & other Indian Herbs (Jambolan, Pterocarpus Marsupium) Psyllium Mormordica Extract or Karela (Bitter Lemon- Asia /Ayurvedic) -Assists glucose pathways in liver – plant insulin like peptide Fenugreek seed extract – stimulates pancreatic function and improves glucose tolerance Konjac Mannon Nopal (Prickly pear cactus- Mexico) Cinnamon- ancient greek / latin writings Banaba (Philippines) -others, garlic, ginseng, dandelion, burdock Take Home Message on Supplements The science is emerging and not definitive. Omega III fatty acid consumption can save patients with diabetes from sudden death. 12 Chous & Richer Obesity Related Eye Disease and Patient Communication Lipoic acid, the subject of European Meta-analyses is an effective adjunct for peripheral polyneuropathy, beyond Neurotin® and antidepressants which are effective in perhaps 50 to 60% of patients. Complex DM metabolic dysfunction requires multiple nutrients – but there is no current consensus on which are most important. There is a new formulation for Diabetic Eye Health: B&L Ocuvite® DF that contains lipoic acid, genistein and various other nutrients. Physical Activity: get 30 minutes of moderate exercise most (at least 5) days of the week Exercise with or without weight loss results in substantial reductions in total and abdominal adiposity both the Finnish Diabetes Study and the Diabetes Prevention Program demonstrated that increased physical activity significantly lowers the risk of type 2 diabetes in high-risk patients (58% reduction in the DPP over 3 years) exercise training significantly promotes SIRT1 activity that improves insulin sensitivity and may also extend human lifespan Communication: 1. Set an effective tone for communication by asking about your patient’s comfort discussing weight status, by being careful to distinguish between the weight problem and the person, and by focusing on the specific health risks (AMD, diabetes and diabetes-related eye disease. cataract, etc.) 2. Assess the patient’s motivation to lose weight and current dietary and exercise status 3. Build a partnership by helping the patient set just a few realistic goals (e.g. lose 7% of body weight, walk 2000 steps daily, lower blood pressure by 10/5 mm Hg) and methods to achieve them (adopt the Mediterranean Diet, buy a pedometer, etc.) physicians face numerous barriers to effectively counseling patients on weight loss, including how, when and with whom to have these discussions language is power - obese patients find the terms “fat” and “obese” highly derogatory in their conversations with health care providers, overwhelmingly preferring the terms “weight,” “excess weight,” or “high BMI” the vast majority of patients who are overweight (84%) and obese (27%) believe they need to lose weight, but a minority had discussed weight loss with their current physicians; the same survey found that what these patients most wanted from their PCPs is dietary advice, help setting weight loss goals, and exercise recommendations VIII. Conclusion (FIGURE 2) 13 Chous & Richer Obesity Related Eye Disease and Patient Communication Battling ocular (and systemic complications) of obesity is analogous to keeping an overflowing bathtub from ruining the bathroom floor (figure 2). 1. “Turn Off the Faucet” by reducing dietary calories, increasing physical activity, controlling blood glucose and blood pressure 2. “Bail Excess Water Out of the Tub” by losing weight, particularly visceral adiposity that drives abnormal glucose metabolism, hypertension, production of reactive oxygen species and inflammation 3. “Mop Up the Floor” with an anti-inflammatory diet, as well as synergistic antioxidants and micronutrients that broadly target the metabolic abnormalities associated with obesity How to Prevent the Overflowing Bathtub From Ruining the Bathroom Floor Caloric Restriction Increase Energy Expenditure Blood Glucose Control Blood Pressure Control CPAP for OSAS TURN OFF the FAUCET Weight Loss AntiInflammatory Diet Targeted Antioxidants Targeted micronutrients BAIL the BATHTUB MOP UP the FLOOR - caloric restriction - exercise - pharmacotherapy (sibutramine, orlistat, rimonabant) & bariatric surgery References: 172 removed to accommodate AAO document size submission guidelines 14