Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
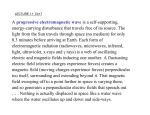
Students’ material Medical Imaging – The Glass Patient Nuclear Medicine Scientific/Technological fact sheet Introduction Suppose we want to find bone tumours. These are difficult to detect with a CT scanner, as those tumours have virtually the same density as the surrounding bone. However, tumours are very active and rapidly growing tissues. Technetium (Tc) is chemically very similar to calcium. If we administer radioactive Tc in the bloodstream of the patient, the bone tumours will uptake this rapidly, after which it can be imaged with a special camera. The imaging technique using such radioactive ‘tracers’ is called Nuclear Medicine (NM). Radioactive isotopes are commonly used in medical imaging as tracers. A given compound is artificially synthesised using a radioactive isotope such as 14C or 3H. Such ‘tagged’ molecules can then be traced as they move through the body or as they undergo chemical reaction. The presence of these tagged molecules (or parts of them, if they undergo chemical change) can be detected by a Geiger or scintillation counter, which detects emitted radiation. For medical diagnosis, the radionuclide commonly used today is 99mTc, a long-lived excited state of technetium99 (the ‘m’ in the symbol stands for ‘meta stable’ state). It is formed when 99Mo decays. The great usefulness of 99m Tc derives from its convenient half-life of 6 h (short, but not too short) and the fact that it can combine with a large variety of compounds. The compound to be Figure 1 – Whole body bone scan with labelled with the radionuclide is so chosen because it extensive bone metastases, shown by concentrates in the organ or region of the body to be the degree of uptake of Tc by the bone studied. Detectors outside the body then record, or tumours (dark spots in the image). image, the distribution of the radioactively labelled compound. The detection can be done by a single detector (Figure 2) which is moved across the body, measuring the intensity of radioactivity at a large number of points. The image represents the relative intensity of radioactivity at each point. The relative radioactivity is a diagnostic tool. For example, high or low radioactivity may represent overactivity or underactivity of an organ or part of an organ, or in another case may represent a lesion or tumour. More complex gamma cameras make use of many detectors which simultaneously record the radioactivity at many points. The measured intensities can be displayed on a computer monitor, and allow ‘dynamic’ studies (that is, images that change in time) to be performed. The images formed using the standard techniques of nuclear medicine, as outlined above, are produced from radioactive tracer sources within the volume of the body. It is also possible to image the radioactive emissions in a single plane or slice through the body using computed tomography techniques (see: Scientific/Technological fact sheet – Computed Tomography). A basic gamma camera is moved around the patient to measure the radioactive intensity from the tracer at many points and angles. The data are processed in much the same way as for X-ray CT scans. This technique is referred to as Single Photon Emission Computed Tomography (SPECT). Another important technique is Positron Emission Tomography (PET), which makes use of positron emitters such as 11C, 13N, 15O and 18F. These isotopes are incorporated into molecules that, when inhaled or injected, accumulate in the organ or region of the body to be studied. When such a nuclide β decays, the emitted positron (β+ or e+) travels at most a few millimetres before it collides with a normal electron (β– or e–). In this collision, the positron and electron are annihilated, producing two γ rays (e+ + e– → 2γ), each having an energy of 511 keV. The two γ rays (or γ photons) fly off in opposite directions (180° ± 0.25°) since they must have almost exactly equal and opposite momentum to conserve momentum (the momentums of the e+ and e– are essentially zero compared to the momentums of the γ rays). Because the photons travel along the same line in opposite directions, their detection in coincidence by rings of detectors surrounding the patient (Figure 3) readily establishes the line along which the emission took place. If the difference in time of arrival of the two photons could be determined accurately, the actual position of the emitting nuclide along that line could be calculated. Present-day electronics can measure times to at best ±300 ps, so at the γ ray’s speed (c = 3⋅108 m/s), the actual position could be determined to an accuracy on the order of about v⋅t ≈ (3⋅108 m/s)⋅(300⋅10–12 s) ≈ 10 cm, which is not very useful. Although there may be future potential for time-of-flight measurements to determine position, today computed tomography techniques are used instead, similar to those for X-ray CT, which can reconstruct PET images with a resolution on the order of 3-5 mm (see: Scientific/Technological fact sheet – Computed Tomography). One big advantage of PET is that no collimators are needed (as for detection of a single photon – see Figure 2). Thus, fewer photons are ‘wasted’ and lower doses can be administered to the patient with PET. Figure 2 – Collimated gamma-ray detector for scanning (moving) over patient. The collimator is necessary to select those γ-rays coming in a straight line from the patient. Without the collimator, γ-rays from all parts of the body could strike the scintillator, producing a very poor image. Figure 3 – Positron emission tomography (PET) system showing a ring of detectors to detect the two annihilation γ rays (e+ + e– → 2γ) emitted at 180° to each other. Both PET and SPECT systems can give images related to biochemistry, metabolism, and function. This is to be compared to X-ray CT scans, whose images reflect shape and structure – that is, the anatomy of the imaged region. Reference – Adapted from Giancoli, Douglas C. (1998), Physics: principles with applications (5th edition, pp. 963-966). Upper Saddle River, NJ: Prentice Hall. Tracer isotopes Instead of radiating the body from the outside, in nuclear medicine γ radiation from the inside of the body is used to visualise not anatomy, but physiological function. The tracer molecules are typically brought into the body by intravenous injection. The distribution of these tracer molecules over the body is determined by the way they are administered, but also by blood flow, blood volume and various metabolic processes. The unstable isotopes produce γ rays, for which the body is transparent. This enables the precise measurement of the concentration of tracer molecules in the body as a function of time and position. Consequently, as said before, nuclear medicine measures function or metabolism instead of just anatomy. Such functional images can also be obtained with CT, MRI and Ultrasound, but nuclear medicine provides images with much higher signal to noise ratios. In the late 1930s, 131I (iodine) was first used to detect thyroid diseases. Nowadays, a large variety of radiopharmaceuticals (tracer molecules) is used in diverse applications. A radionuclide is a molecule carrying an unstable isotope that releases γ rays during radioactive decay. Whereas PET requires an annihilation process in which two γ photons are released in opposite directions, planar imaging and SPECT only require a decay in which a single γ photon is produced. As the transmission through the patient should be sufficiently high, the energy of the γ photon has to be large enough. But it must not exceed certain levels, since the absorption in the detector cannot be too low. Another important feature is the half-life of the radionuclide, which has to fit in with the kind of examination. The effective half-life in the tissues is the result of radioactive decay and the extraction of the substance from the blood by the kidneys of the patient. The ‘production’ of γ photons by a radionuclide inside the body results from three different modes of radioactive decay: electron emission, electron capture and positron emission. Electron emission (β– decay) – In this decay mode electrons (β– particles) are emitted by the nucleus. An excess of neutrons in the nucleus of an unstable isotope causes a neutron to be converted into a proton and an electron: n → p+ + e–. There is no change in mass number, but the atomic number of the nucleus is increased by one. Nearly always the ‘daughter nucleus’ is produced with excess energy. Usually it loses this immediately by the emission of one or more γ photons, leaving the daughter nucleus with minimum energy in the ground state. In some other cases the γ photon is not emitted until a certain time after the emission of the β particle. The β particles do not come far in tissues, at most a few centimeters. Electron capture – The nucleus captures an orbital electron, which is combined with a proton to produce a neutron: p+ + e– → n. Then electrons from higher states fall down to fill the vacancies, emitting X-ray photons. If the daughter product is in an excited state, it can immediately decay to a lower energy state by emitting additional γ photons. The daughter nucleus may also be meta-stable, decaying later. An example used in imaging is 123I (with a half-life of 13 hours), which emits 28keV X-ray photons and 160keV γ photons. Positron emission (β+ decay) – Nuclides with a shortage of neutrons may lose energy and become stable by changing a proton within the nucleus into a neutron and a positron (positive electron): p+ → n + β+. This positron is ejected from the nucleus with high energy. The daughter nucleus, if left in an exited state, loses its excess energy by the emission of one or more γ photons until it reaches the ground state. After a very short time (on the order of 10–9 s) and within a few millimetres of the site of its origin the positron hits an electron and annihilates, because the positron is the anti-matter equivalent of the electron (Figure 4). A small explosion takes place: the mass of the two particles is converted into energy, which is emitted as two γ photons in opposite directions. Each photon has an energy of 511 keV, which is equivalent to the mass of an electron or positron (E = m⋅c2). This physical principle is the basis of PET. An example of a positron emitter used in imaging is 18F with a half-life of 109 minutes. Figure 4 – Schematic representation of positron-electron annihilation. When a positron comes near an electron, both particles are converted into a pair of 511 keV photons, each going in opposite directions. Gamma ray detectors The gamma camera for the detection of the emitted γ photons outside the body is widely used for almost half a century now (Figure 5). Most gamma cameras use a single large sodium-iodide (NaI) crystal (Figure 6). A lead collimator is positioned in front of the crystal to ban scattered photons and to protect the fragile and very expensive crystal. The γ photons that travel right through the collimator interact with the NaI crystal. This results in a small light flash. Behind the crystal an array of light-sensitive photomultiplier tubes (PMT’s) is attached. They produce digital pulses proportional to the intensity of the light flashes. The front-end electronics link the information to the computer, where an image can be reconstructed. Image formation Gamma Imaging, also called planar imaging, is the application used most often in nuclear medicine (Figure 7). During a certain period of time, the detector (gamma camera) receives emitted γ photons from radionuclides in the patient’s body. Higher levels of detected photons are visualised as darker spots on the image (Figure 1). Figure 5 – Gamma camera. In order to detect as many photons as possible, two cameras are used – and sometimes even more. Figure 6 – Schematic representation of a gamma camera with a single large scintillation crystal (52 × 37 cm) and parallel hole collimator. Figure 7 – Schematic representation of the planar imaging technique with a gamma camera. Such a planar image is a 2D projection image, in which depth information is lost. It can therefore be compared with an X-ray photograph (see: Scientific/Technological fact sheet – X-ray Photography). The spatial resolution is rather low because the source produces radiation in all directions. Because of the fact that only the detection position is known and not the exact source position, a collimator is necessary. Changes over time can be measured too. For example, in the case of a certain kidney malfunction a series of kidney scans can be taken in order to compare the condition of both kidneys. One of the kidneys has a failure if the concentration of the tracer only rises in that kidney, while the other shows the normal decrease after the increase (Figure 8). SPECT: Single Photon Emission Computed Tomography Since the development of Computed Tomography (CT) in the early 1970s, the base for Single Photon Emission Computed Tomography (SPECT) was set. This technique often uses the technetium isotope 99mTc, from which a single photon is emitted for every nuclear disintegration. These photons enter (two, sometimes three) gamma detectors that are rotated around the patient. The detector units must be as close to the patient as possible, since the spatial resolution decreases with the distance from the collimator. The image reconstruction is along the lines of CT. However, it should be noted that with SPECT this is more difficult. The reason for this is that the SPECT imaging technique not only deals with an unknown attenuation coefficient (as in CT), but also with an unknown source intensity. Figure 8 – Overlay of CT and DMSA SPECT scans. Possibly a tumour in the right kidney. Figure 9 – SPECT scan showing increased uptake of radionuclide-labelled leukocytes in the patient’s left knee joint, indicating an infection. The advantage of SPECT over planar imaging lies in the improvement of contrast between regions with various functions, better spatial resolution, and most important: a much better quantification. However, SPECT imaging is inferior to PET due to a somewhat lower resolution and sensitivity. Also the use of the necessary collimator results in a substantial decrease in detection efficiency as compared to PET. However, the availability of SPECT radiopharmaceuticals and the economic and practical aspects of SPECT instrumentation make this mode of emission tomography attractive for clinical studies of tissue function. PET: Positron Emission Tomography In 1975 Ter-Pogossian built the first PET scanner, in which PET stands for Positron Emission Tomography. This imaging technique is based on the use of β+ emitters (or positron emitters), such as 11C, 13N, and 15O isotopes. These basic biological elements are prepared in a cyclotron, which is a very expensive device. Unfortunately they have short half-lives of 20, 10 and 2 minutes, respectively. The two γ photons from the annihilation of the positron and the electron enter a gamma camera, which actually forms a ring around the patient (Figure 10). This ring is composed of a large number (e.g. 90 or 180) photomultiplier tubes. If two opposite detectors receive a photon at the same time, they produce coincident pulses. Temporal resolution of these detectors has to be very high indeed. Noncoincident detected photons from other interactions are ignored. Therefore, only photons of annihilation processes are measured to construct the PET image. The lines on which the annihilation interactions took place are now known, and from the signals of each of the many pairs of detectors at different angles the computer can reconstruct the tomographic image of the slice, as in CT. Statistical probability calculation is necessary to determine on which location on the lines the annihilation most likely took place. Some three million counts are acquired in an overall scanning time of 30 Figure 10 – Schematic representation of the PET minutes. scanner. One of the advantages of PET is that the metabolism in certain tissues can be measured by adapting the tracer molecule. For example, cancer tissue can be detected in an early stage – earlier than is possible with CT or MRI. In addition to that, PET can also measure functional activity of the heart and brain (Figures 11 and 12). Figure 11 – A PET image of the heart. Figure 12 – Brain imaging with PET reveals the different regions of the brain that are active while performing specific tasks. A disadvantage of PET is the need for very expensive cyclotron facilities to produce positron-emitting pharmaceuticals. That is why the number of PET scanners in a country is relatively limited. In addition, the hospital has to be directly near the cyclotron because of the radionuclides’ half-life of only several minutes. A solution to that is the use of a socalled tracer cow. An example of such a tracer cow is a container filled with the radioactive isotope radium. The radium decays to krypton, which can be used as a tracer. This decay product is then tapped off – or ‘milked’ – from the container whenever it is needed. The spatial resolution of a PET scan is not very high due to the relatively large detector units. Moreover, annihilation takes place at a distance of about 2-5 mm from the actual tracers. The radiation dose is a problem too, although it can be reduced by using tracers with a short half-life. Physics principles • Radioactivity: isotopes, radiation (α, β–, β+, γ), radiation absorption, decay, half-life, radiation detection, radiation dose, annihilation, photon energy in eV • Bohr model of the atom: electron energy levels, photon energy, emission of X-ray photons Additional links http://science.howstuffworks.com/nuclear-medicine.htm