Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
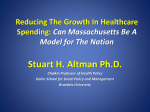
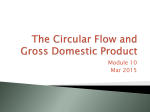
Health Care Reform in 2009: Expanding Coverage and Reforming Health Care Delivery Aaron McKethan, Ph.D. The Engelberg Center for Health Care Reform The Brookings Institution May 28, 2009 2 Presentation Overview • Context of national health care reform • Common options to expand coverage and fill financing gaps • Reforming health care delivery, moving toward accountable care • One promising model: accountable care organizations 3 Context for Reform • Government already plays a huge role in health care » Local, state, and federal government spending accounted for 46% of the estimated $2.4 trillion spent on health care in 20081 – » • $461 billion on Medicare, $361 billion on Medicaid Medicare and Medicaid spending alone is projected to account for as much as 13% of GDP by 2040, if these program continue on current trajectory Income and payroll tax exclusions for employer-provided health insurance accounted for another $250 billion per year in foregone federal revenues2 » Health care spending has risen about 2.7% faster than the overall economy for the past half century4,5 » Total health care costs are projected to increase from 16% to nearly 20% of GDP in the next decade Sources: 1. Keehan, Sean et al, “Health Spending Projections Through 2017: The Baby-Boom Generation Is Coming To Medicare,” Health Affairs 27 (2008): w145–w155 (published online 26 February 2008).; 2. Steuerle, C. Eugene, “Is Health Spending Out of Control?” National Center for Policy Analysis Brief Analysis No. 586, 17 May 2007.; 3. Office of Management and Budget, Analytical Perspectives: Budget of the United States Government, Fiscal Year 2009 (2008).; 4. Centers for Medicare and Medicaid Services. “National Health Expenditure Projections 2007-2017.” 5. Congressional Budget Office. “The Long-Term Outlook for Health Care Spending.” November 2007. 4 Projected Health Care Spending as a Percentage of GDP, 2007 – 2082 Source: Congressional Budget Office, “The Long-Term Outlook for Health Care Spending” (November 2007). 5 Context for Reform • • • Coverage and payment/delivery system reforms together » Failure to realize improvements in both cost and quality will render efforts to expand coverage neither feasible nor sustainable. » Incremental delivery reforms not enough; must be integrated around accountability for results/ Tentative bipartisan approach, “engagement” among stakeholders » Emphasis on “tentative” » Including but not limited to recent “agreement” for 1.5 percent slowdown/10 yrs Bipartisan concern about long-term fiscal impacts » First, do no harm; “paygo” within 10-year window » Second, steps to bend the curve over time 6 Emerging Reforms/Packages • Senate Finance Committee • Congressional Budget Office/Joint Committee on Taxation • President’s Budget • American Recovery and Reinvestment Act of 2009 • Patients’ Choice Act 7 Common Infrastructure Reforms • Health information technology » • Improve quality measurement infrastructure » • Needed to: (a) support providers in improving care; (b) move toward payments for value; and (c) evaluate payment/delivery system reforms Comparative effectiveness research » • Build on HIT provisions in ARRA to ensure that “meaningful use” is meaningful Beyond head-to-head treatment studies; including practice patterns and analysis on subpopulations Infrastructure subtotal: ~($20-$30B) over ten years Note: Numbers are illustrative based on a range of reforms being discussed. 8 Common Components of Coverage Reform • Individual responsibility/mandate for health insurance » • • • Medicaid/SCHIP Policy » Interactions with insurance exchanges » Expansions of mandatory or optional populations up to ~100-250% FPL Insurance Exchanges » Non-group and small groups get a range of plan options via actuarial equivalence, possibly including public plan » Risk adjustment, modified community rating with age bands, no pre-existing condition restrictions, etc. Targeted Subsidies » Range of definitions of “minimum creditable coverage” and enforcement strategies Ideas: Low-income subsidies/tax credits, subsidies for max spending-to-income thresholds, small firm tax credits, early retiree credits, etc. Coverage reform subtotal: ~($1,000B-$1,400) over ten years Numbers illustrative 9 Common Financing Options • Changes to tax treatment of employer-sponsored insurance » • Employers must make a creditable commitment (pay or play) » • Range of options, including caps, exceptions, income but not payroll taxes, etc. Most firms must offer/contribute to insurance coverage Other revenues or offsets » Alcohol, cigarettes, sugar-sweetened beverages, etc. » Re-directing some DSH payments Financing subtotal: ~$500-$700B over ten years Note: Numbers are illustrative based on a range of reforms being discussed. 10 Health Reform Subtotals Category Budget range (10-year estimates) Infrastructure ~($20-$30B) Coverage ~($1,000-$1,400B) Financing ~$500-$700B Gap ~($520-$730B) Note: Numbers are illustrative based on a range of reforms being discussed. 11 Filling the Gap: Common Payment/ Delivery Reform Options • Prevention/wellness • Reduce payments for lower-value care • More bundled payments • Targeted pay-for-performance • Coordinated care programs, benefits • Transitioning to accountability-based payments Delivery system reform subtotal: ~$300-350B Remaining gap: ~($220-380B) Note: Numbers are illustrative based on a range of reforms being discussed. 12 Key Elements of Delivery System Reform • Local accountability for quality and cost across the care continuum » • Feasible across diverse practice types/organizational settings » • Reforms should be flexible to allow for variation in the structure and strategies of local health systems Shift payments from rewarding volume and intensity to increasing value » • Reforms should “build in” expectations of cost containment and quality improvement Payments should encourage collaboration and shared responsibility among providers and consistent incentives/measures from payers Help consumers make better decisions » With increased accountability on the part of providers must come greater transparency and decision support for consumers 13 Accountable Care Organizations • ACOs are collaborations to assume responsibility for overall patient care, across providers and care settings. • Key features of ACOs: » Voluntary provider participation » Local accountability for cost, quality, and capacity across the continuum of care » Payment incentives (e.g., shared savings) and related organizational support gives providers the support needed to improve care and slow cost growth » Performance measurement to ensure that appropriate care is being delivered and that cost savings are not attributable to limitations on necessary or appropriate care 14 Some ACO Issues • ACO Structure: Established governance structure and broad (voluntary) physician and payer participation. Ideally participation by Medicare. • Measures: Well-established performance measures relevant to multiple payers/populations. Included measures become more sophisticated over time. • Payment Incentives: Participating payers agree to adopt their own provider payment incentives that at a minimum involve QI and may include cost savings and efficiency; incentives based on performance across specified populations. » Over time, ACO payment incentives can transition from “one-sided” shared savings to two-sided risk, partial capitation, and further reforms » Beneficiary incentives also possible (e.g., differential copays) • Performance reporting: Providers, payers, and consumers receive regular, risk-adjusted reports about performance with benchmarks. • Complementary reforms: ACOs are compatible with, and can be reinforced by, other reforms including bundled payments, care coordination, chronic disease management, pay-for-performance, incentives to prevent re-hospitalizations, etc. 15 Initial Shared Savings Derived from Spending Below Benchmarks Projected Spending ACO Launch Spending Benchmark Shared Savings Spending Actual Spending Time 16 Steps for Initial ACO Implementation 1. Local providers and payers agree to pilot ACO reform 2. ACO provides list of participating providers to payers 3. Patients are “assigned” to ACOs (e.g., based on preponderance of E&M codes) 4. Actuarial projections about future spending are based on last 3 years 5. Determine/negotiate spending benchmark and shared savings 6. ACO implements capacity, process, & delivery system improvement strategies • e.g., reducing avoidable hospitalizations, coordinating care, health IT 7. Progress reports on cost and quality are developed for ACO beneficiaries 8. At year end, total and per capita spending are measured for all patients (regardless of whether they received care from ACO providers) 9. Savings under the benchmark is shared between providers and payers