Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
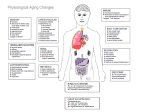
1 Running head: Young Aging Young Aging Hannah Holladay Nursing 444 10-31-13 2 Running head: Young Aging Introduction On Tuesday, September 24th, 2013 I took care of 21 year old male A.M. on the Thoracic Surgery Care Unit (TSCU). He was transferred from the Brian Center in Low Moor, VA with a chief complaint of rapid heart rate. He was diagnosed with Amyotrophic Lateral Sclerosis (ALS) at age 18, also known as Lou Gehrig’s Disease. A.M. had a tracheostomy and was on a Pressure Regulated Volume Control (PRVC) ventilator. He was also a quadriplegic. Due to his tracheostomy, ventilator, and inability to move his skeletal muscles; A.M. was unable to speak. Upon arrival to Roanoke Memorial Hospital (RMH), A.M. presented with a rapid heart rate, extreme hypotension, and respiratory failure. He was diagnosed with Tachycardia, Supraventricular Tachycardia (SVT), and Septic Shock. A.M. was being treated for Pneumonia at the Brian Center for 3 days before coming to RMH. He was NPO with a G tube on continuous tube feeding (TPN). He had been on continuous Diltazem for SVT and Norepinephrine for Chronic Hypotension. A.M. is a young adult in the Intimacy vs. Isolation Stage of Development. In this stage, it is crucial that young adults form relationships with others that are filled with love and strength (Mauk, 2013). It was evident that A.M. was experiencing extreme isolation because of the extent of his ALS. He also did not have any visitors the whole day. Family resources were inaccessible due to lack of family presence or history in the chart. A.M. was not a Carilion patient before being admitted to RMH, so he did not have any previous history in the electronic medical record. It was reported that his mother was his primary caregiver. Presenting Symptoms and Impact Even though A.M. was only 21 years old, he did have some chronic diseases. ALS was his main diagnosis, a terminal illness resulting in neuromuscular decline. He also had Chronic Running head: Young Aging 3 Hypotension, Chronic Respiratory Failure (CRF), Sinus Tachycardia, Pneumonia, and Constipation. There is no proof of definite risk factors for his main diagnosis of ALS, but some are being researched. A mutated gene SOD1 has been found in many cases of ALS throughout the world. Toxins that could cause this mutation are being investigated as possible risk factors. Other possible risk factors that need more research are minerals in the diet, toxic metal exposure, pesticides, and the poliovirus. None of these risk factors have been confirmed, but research is being done to better pinpoint possible causes of ALS (The ALS Association, 2013). If it were proven that these risk factors related to ALS, causes of the disease would be known. They would cause a decrease in neuromuscular function and lead to death. Maintenance of this disease includes making the patient as comfortable as possible. Because there is no cure, there is no drug that will make the patient’s status improve (Porth, 2011). However, there are treatments that can better quality of life for A.M. Examples of these treatments for him include medications for muscle weakness and spasms, helping psychological issues, addressing communication problems, maintaining nutritional status (Porth, 2011). The main focus behind the obvious physical symptoms would be A.M.’s psychosocial decline. Due to the nature of his disease, he probably struggles with the emotions of being a 21 year old with terminal illness. If these are managed, A.M. will have a better quality of life while battling this horrific disease. Because A.M.’s problems come from his diagnosis of ALS, this disease is the main risk factor for his other chronic diseases. He had neuromuscular decline, which causes muscle weakness. This eventually causes the muscles of the chest to deteriorate, resulting in the inability to breathe alone, causing CRF. Because of the respiratory failure, he developed Pneumonia. This 4 Running head: Young Aging infection is detrimental to his already weakened immune system. He developed Septic Shock, another infection associated with Tachycardia and Hypotension. The patient’s lack of mobility is what causes Constipation (Porth, 2011). Although A.M. has chronic diseases, he did not develop them because of his lifestyle choices. A.M.’s respiratory failure must be managed so he can adequately ventilate and perfuse his lungs in order to be more comfortable. His heart function must also be under control in order to regulate blood flow and perfuse the body. A low blood pressure and high heart rate result in decreased cardiac output. If these are managed, his cardiac function may be regulated, and his anxiety about his condition could be at ease His constipation is treated with an array of medications. Quality of life will be promoted by reducing gastrointestinal discomfort. Managing these chronic conditions for this young patient will help him be more comfortable as he nears death. Changes of Aging A.M. is currently battling Septic Shock and Pneumonia. These are both serious, acute illnesses. They could both cause death because of A.M.’s neuromuscular and immune system decline due to ALS. They have an impact on aging in an obvious way with fatal consequences. They both come with physical manifestations that are characteristic of this patient’s chronic diseases. These systemic characteristics from CRF and Chronic Hypotension are what could cause his demise. Although they are acute illnesses and do not directly affect aging, they could cause A.M.’s chronic illnesses to worsen. If he were able to manage these acute illnesses and be discharged to a long-term care facility, A.M. would require constant care and life support. ALS is A.M.’s main problem as it is the root of every other issue. ALS can cause trouble swallowing, breathing, moving extremities, talking, and expressing emotions (Porth, 2011). Running head: Young Aging 5 Worsening of CRF and Chronic Hypotension can decrease respiratory and metabolic perfusion. If respiratory and metabolic perfusion decrease, multi-system failure can result. A.M.’s inability to swallow impairs his nutrition. Without adequate nutrition, the patient cannot supply his body with the proper proteins, carbohydrates, and fats that it needs. Without these crucial nutrients, his muscles and bones will not be able to maintain strength and function. Musculoskeletal decline results in an inability to move, walk, exercise, etc. Improper nutrition and impaired mobility go hand in hand with the development of constipation. Osteoporosis and muscle atrophy are common in the aging/elderly population. A.M. already has atrophy and risk factors for osteoporosis such as inadequate nutrition or lack of mobility. These problems affect aging by affecting A.M.’s current health status. Prevention of Exacerbation of Chronic Diseases There is nothing that can be done to prevent ALS, but respiratory failure, hypotension, and further constipation exacerbations can be avoided. A.M. is on a PRVC ventilator to assist with the work to breathe. With this assistance, there will be less respiratory failure exacerbation because the ventilator compensates if the patient’s respiratory strength declines further. According to The European Respiratory Journal, by using a monitoring system called “Respicard”, there were fewer exacerbations of respiratory failure in mechanically ventilated patients. The score helped nurses determine whether or not further care was needed. This also helped reduce costs of unnecessary care in patients who already have chronic illnesses that require heavy healthcare costs (Vitacca, Blanchi, Guerra, Fracchia, Spanevello, Balbi & Scalvini, 2009). This type of monitoring system would be beneficial by helping to prevent exacerbations of CRF while minimizing the cost of A.M’s extensive healthcare. Running head: Young Aging 6 Prevention of Chronic Hypotension for this patient is maintenance of blood pressure by administering continuous norepinephrine. This medication keeps A.M.’s blood pressure from dropping too much. He is unable to make lifestyle choices to affect his blood pressure due to his quadriplegia, but adequate fluid and electrolyte intake would be something that could be managed by someone with Chronic Hypotension. In order to prevent constipation, ambulation is needed because physical mobility promotes peristalsis. Since A.M. cannot move; he is given Milk of Magnesia, Colace, and Pericolace for Constipation. Interventions: End of Life Anticipated A.M.’s mother decided to make his code status “Do not Resuscitate” (DNR) on 9-23-13. This is the type of decision for his mother that comes with the heavy burden of letting a child go. She had to accept the fact that his condition was rapidly worsening. A.M. has been struggling with ALS since he was 18 therefore, has likely accepted the fact that it will contribute to his death. In order to help A.M. and his mother reach full acceptance, counseling sessions may be needed. These sessions could help the mother with the grief of loss while helping the son accept death. In this situation, acceptance is hard because the son is so young and his mother is losing her child. A referral for a Palliative Care meeting was made in the electronic medical record. Interdisciplinary team meetings are necessary to discuss cases like this in order to determine the plan of care (Mauk, 2013). According to the International Journal of Nursing Studies, “Case management can be helpful in meeting patient needs and ensuring continuity and quality of care across settings…This is done by advocating the patient’s needs to other care providers…”, (van der Plas, Deliens, van de Watering, Jansen, Vissers & Onwuteaka-Philipsen, 2013). 7 Running head: Young Aging End-of-Life care would be beneficial to help the patient and family become more comfortable with accepting death. The physician, nurses, case manager, mother, and A.M. must communicate about all options of care. The goal of possible End-of-Life care for A.M. would be to ensure the best quality of life while comforting the mother as well (Mauk, 2013). As it says it Gerontological Nursing Competencies for Care, “The goal of palliative care is to achieve the best possible quality of life for patients and their families. Control of pain, other symptoms, and of psychological, social, and spiritual problems is paramount”, (Mauk, 2013). When dealing with a patient who is a candidate for Palliative Care, the nurse must be professional when interacting with the patient and family. The nurse must also be a valuable part of an interdisciplinary team that includes the family that makes the ultimate decision. The nurse must advocate for the patient by referring for proper physical and psychosocial support (Mauk, 2013). Psychosocial Interventions A referral to grief counseling would be beneficial for the mother. She is the primary caregiver for A.M., meaning she has exhausted herself with countless trips to the hospital, household modifications for quadriplegia, and exponential healthcare bills for 3 long years. This impact has certainly been tremendous on her physical and psychological health. The mother must release herself from the drive to care for her son physically. She now needs to realize that emotional support is more important. Hopefully anticipatory grief for the patient and mother began at the time of diagnosis in order to forestall the patient’s eventual loss of independence. The mother’s probable feelings of lost hope and helplessness need to be addressed so she can better deal with losing her son (Mauk, 2013). Running head: Young Aging 8 Because A.M. was unable to speak and the mother was not present during the shift, it was hard to assess emotional status. A probable psychosocial intervention for A.M. would be having a counselor come to the bedside and talk to him. Having someone just talk to him and support him emotionally would help him be at ease with death, even if he is unable to talk back. A prudent nurse would also give emotional support to the patient by using soothing tones, giving comforting touch, and keeping him as comfortable as possible. Financial resources must also be considered when treating psychosocial issues. A.M. has had ALS for 3 years and is a quadriplegic. He has had many expensive hospitalizations and medications. He was also in long-term care at the Brian Center. Before that, A.M. probably lived at home with his mother. Modifications to the home would be needed such as wheelchair ramps and special bathroom essentials as his condition worsened. All of these necessities add up in cost. A.M. qualifies for Medicare/Medicaid, which provides three types of health protection: health insurance, long-term care, and supplemental coverage of expenses for people with disabilities who come from a low-income family (Mauk, 2013). As A.M.’s disease progressed, and the expenses grew, his ability to self-care diminished. He may have been able to work non-strenuous jobs during the early stages of ALS, but as the disease progressed, his neuromuscular status declined causing him to lose the ability to work. A.M.’s mother has possibly cut down on work time to care for her son, decreasing income as well. Discharge Planning/Consultations/Referrals Discharge planning begins at admission. The focus for A.M. upon admission would have been his acute state. Discharge back to long-term care would be the only option for A.M. because of his extensive needs. Plans for discharge can include a switch to Palliative Care or 9 Running head: Young Aging discharge to Hospice. If A.M. is stable enough to be discharged to Hospice care, he would have comfort and quality of life promoted. Quality of life and comfort would be the main priorities upon possible discharge for A.M. Promotion of psychological needs while dealing with impending death would come before treating physical needs in Hospice Care. Referrals needed for A.M. are mostly aimed at quality of life and end-of-life care. However, physical needs before Palliative Care is initiated are important as well. Physical Therapy would be beneficial to help A.M. prevent the development of contractures in his joints due to paralysis. He has a Stage II decubitus ulcer on his sacrum that would need a Wound Care consult. Respiratory Therapy would help maintain the PRVC settings and assess A.M.’s respiratory status. If the patient’s Palliative care consult results in the decision to go ahead with Comfort Care, psychosocial referrals would be necessary. Social Work would need to be contacted to help the mother find ways to cope with her son’s condition. They also may need to determine family involvement in A.M.’s care. The Case Manager will help organize the plan of care whether it be Hospice or Comfort Care in the hospital. It has been proven that Case Managers are not only involved with the patient but educate other healthcare professionals about palliative care and other consultations (van der Plas, Deliens, van de Watering, Jansen, Vissers & Onwuteaka-Philipsen, 2013). Summary Analysis of this patient helped me realize the intensity of End-of-Life care. When I received report that day, I was excited to care for a patient my age. I did not know much about ALS and quickly discovered the severity. A.M was under a blanket of extreme isolation that no 21 year old should experience. He had the chronic diseases of an elderly person nearing death Running head: Young Aging 10 but should be a senior in college. A.M. had most likely already accepted the fact that his illness would kill him. That day, I encountered a huge reality check that will forever impact my nursing practice. I will always consider the big picture, not only physical ailments; but the family, psychological issues, and quality of life. Caring for this patient while feeling so helpless showed me that even the slightest emotional support translates indefinitely…even when there is nothing else that can be done. 11 Running head: Young Aging References Mauk, K. L. (2013). Gerontological nursing competencies for care. (3rd ed.). Burlington, MA: Jones & Barlett Learning, LLC. Porth, C. (2011).Essentials of Pathophysiology: Concepts of Altered Health States. 3rd Edition. Philadelphia, PA: Lippincott Williams & Wilkins. The ALS Association. (2013, January 25). Als association fighting lou gehrig's disease: Environmental factors. Retrieved from http://www.alsa.org/research/about-alsresearch/environmental-factors.html van der Plas, A. G. M., Deliens, L., van de Watering, M., Jansen, W. J., Vissers, K. C., & Onwuteaka-Philipsen, B. D. (2013). Palliative care case management in primary care settings: A nationwide survey. International Journal of Nursing Studies, 50, 1504-1512. Vitacca, M., Blanchi, L., Guerra, A., Fracchia, C., Spanevello, A., Balbi, B., & Scalvini, S. (2009). Tele-assistance in chronic respiratory failure patients: a randomised clinical trial. European Respiratory Journal, 33(2), 411-418.