Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
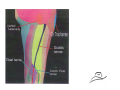
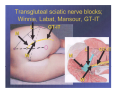
Maverick Regional Anesthesia Education, LLC Sciatic is largest nerve of body, nearly 2cm in width Formed from L4 to S3 nerve roots Can be used by itself, but most often combined with Femoral nerve block to cover tourniquet pain or surgical involvement of medial foot/ankle. By itself: procedures of foot with an ankle tourniquet In combination with Lumbar plexus or Femoral blocks can be used for all procedures of the leg In combination with Saphenous nerve block, it can be used for all procedures distal to knee There are no absolute contraindications to the sciatic nerve block. Use this block with caution in presence of a fresh Tibial/Fibula fracture (first 24 hrs…24‐72 hrs consult with surgeon) Formed from L4‐S3 roots Exits pelvis through greater sciatic foramen, anterior to piriformis muscle Descends between Greater Trochanter of femur and Ischial Tuberosity Its course can be estimated by drawing a line from midpoint of a line between GT‐IT and apex of popliteal fossa In lower 1/3 of thigh, it forms two divisions: Tibial and Common Peroneal nerves (15% of cases this division occurs at level of piriformis muscle) Division may take place at any point between sacral plexus and lower 1/3 of thigh Typically division occurs at or above 7cm from popliteal crease Cutaneous: Anterio‐lateral and posterio‐lateral part of leg Ankle except for medial malleolous Foot except for its medial boder Muscular: All hamstring muscles Part of adductor magnus All muscles of lower leg and foot Joints: Hip: Posterio‐superior compartment Knee: Posterior and infero‐lateral compartment Ankle: All except medial Foot: All joints of the foot Bone: Femur: Posterior portion Tibia and Fibula: All of both except anteriomedial portion of tibial plateau All tarsal, metatarsal, and phalanges of foot Anterior: Van Elstraete, Beck, Chelly Lateral (popliteal) Lithotomy: Raj Posterior: Mansours parasacral, Labat’s classic and DiBenedetto’s subgluteal Position: Sim’s with operative side up Landmarks: Posterior Superior Iliac Spine, Greater Trochanter and Sacral Hiatus Needle Insertion: 4cm caudad from midpoint of a line drawn from PSIS and GT A line drawn from Sacral Hiatus and GT should pass through insertion point (Winnie’s line) Plantar flexion: stimulation of Tibial nerve Dorsiflexion/Eversion: stimulation of Common Peroneal nerve Inversion: combined stimulation of Tibial and Common Peroneal nerves (Most Desirable). Isolated contraction of hamstring muscles Rhythmic and brisk contraction of gluteal muscles ▪ Stimulation of inferior gluteal nerve ▪ Needle too superficial ▪ Advance needle until sciatic nerve is located Position: Sim’s with operative side up Landmarks: Greater Trochanter (GT) Ischial Tuberosity (IT) Needle Insertion: 4cm caudally from midpoint of a line drawn from GT‐IT. Plantar flexion: stimulation of Tibial nerve Dorsiflexion/Eversion: stimulation of Common Peroneal nerve Inversion: combined stimulation of Tibial and Common Peroneal nerves (Most Desirable). Isolated contraction of hamstring muscles Postion: Supine with leg in neutral position Landmarks: Lateral Femoral Condyle OR Superior aspect of Patella Groove between Vastus Lateralis (superiorly) and Biceps Femoris (inferiorly). Needle Insertion: 7cm cephelad from lateral femoral condyle ( or Superior aspect of Patella) in groove between vastus lateralis and biceps femoris. Superior aspect of patella Plantar flexion: stimulation of Tibial nerve Dorsiflexion/Eversion: stimulation of Common Peroneal nerve Inversion: combined stimulation of Tibial and Deep Peroneal nerves (Most Desirable). First described by Beck in 1963 Chelly & Delaunay later described it using easier landmarks uses bony landmarks and dissecting lines; all three have needle insertion points obscured by lesser trochanter Van Elstraete then described it using inguinal crease and femoral artery as landmarks Landmarks are very simple and distinct in most patients Lesser trochanter does not obstruct path of needle toward sciatic nerve Useful for patients unable to assume lateral decubitus position Allows one prep area when combined with Femoral nerve block and thus decreases time required for both blocks. Deep block…may require generous sedation and local infiltration of underlying tissues Slow onset: allow 30‐45 min Femoral crease Femoral artery palpated at femoral crease Mark femoral artery along thigh (line 1) Draw line parallel to femoral artery 2.5cm medially (line 2) Needle insertion is 2.5‐4cm distal to femoral crease along line 2. Femoral Crease Line 2 2.5‐4cm Line 1 150mm insulated needle (19g) for catheter insertion; 22g 150mm insulated “b” bevel for single shot Inserted in a posterior and lateral direction 10‐15 degrees from vertical Sciatic nerve typically contacted at 10‐12 cm Plantar flexion: stimulation of Tibial nerve Inversion: combined stimulation of Tibial and Common Peroneal nerves (Most Desirable). Isolated contraction of the hamstring muscles ▪ Indicates stimulation of motor branch of hamstring Contraction of adductor muscles of thigh ▪ Indicates direct stimulation of adductor longus and adductor magnus muscles (advance the needle) Demand Tibial nerve response at <0.4mA ▪ Sensory innervation of knee and ankle arises from Tibial nerve. Dorsiflexion or Eversion stimulation: Common Peroneal nerve; use for orientation to find Tibial nerve Use doppler to locate femoral pulse if necessary Deep block: be generous with local and sedation