Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
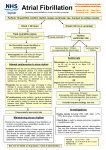
Guideline for the management of arrhythmias The following guideline is approved only for use at University College London Hospitals NHS Foundation Trust. It is provided as supporting information for the UCLH Injectable Medicines Administration Guide. Neither UCLH nor Wiley accept liability for errors or omissions within the guideline. Wherever possible, users of the Guide should refer to locally produced practice guidelines. UCLH’s guidelines represent the expert opinion of the clinicians within the hospital and may not be applicable to patients outside the Trust. Adapted from UCLH Guidelines for the management of common medical emergencies and for the use of antimicrobial drugs Reviewed by: Dr Martin Lowe, Consultant Cardiologist UCLH Amended July 06 Remember - treat the patient, not the ECG! SINUS BRADYCARDIA Treatment: none unless hypotensive, then atropine 600 micrograms IV. Repeat up to total of 2.4mg, then pace. If you have the experience, consider atrial pacing if AV nodal conduction is normal. Ventricular pacing may actually worsen cardiac output and blood pressure. SINUS PAUSES (pause > 2 Sec) Treatment: atropine or transvenous pacing if prolonged or symptomatic. FIRST DEGREE AV BLOCK (PR Interval > 0.20 Sec) Treatment: None. Observe and check drug treatment for beta-blockers, calciumchannel blockers etc. SECOND DEGREE HEART BLOCK (a) Mobitz type I (Wenckebach) AV block (PR increasing then dropped beat) Treatment: If symptoms, then atropine and if after anterior MI then temporary transvenous pacemaker. (b) Mobitz type II (2:1, 3:1, etc) Treatment: Consider temporary transvenous pacemaker if symptomatic. Atropine injection and isoprenaline infusion may be tried in the interim: 2mg isoprenaline in 500ml 5% glucose (4mcg/ml). Start at a rate of 1 July 2006 ‘Common medical emergencies – arrhythmias’ microgram/minute (15ml/hr) titrating up in steps of 1microgram/minute at intervals of 2-3minutes, until a satisfactory heart rate is achieved or adverse effects such as hypotension or ventricular arrhythmias occur (Usual max: 10 micrograms/min). COMPLETE HEART BLOCK Treatment: Temporary transvenous pacemaker or external pacemaker if severely bradycardic, hypotensive and reduced consciousness (almost always required if complete heart block after anterior MI). NEW BIFASCICULAR BLOCK - (RBBB + L axis deviation; LBBB + R axis deviation) OR TRIFASCICULAR BLOCK - bifascicular block and long PR Treatment: If these develop in the context of acute myocardial infarction, consider temporary transvenous pacing. TEMPORARY PACING IN ACUTE MI Rate/conduction disturbance Sinus bradycardia without hypotension, ventricular ectopics, angina, LVF, syncope Sinus bradycardia with any of the above despite atropine Accelerated idioventricular rhythm Idioventricular rhythm with rate <45 bmp and/or hypotension Recurrent sinus pauses >2 sec Torsade de pointes First degree AV block Wenckebach (unless hypotension) Wenckebach with hypotension/bradycardia Mobitz II (dropped beats) Complete heart block Isolated left anterior hemiblock, left posterior hemiblock or RBBB New LBBB New bifascicular block (alternating RBBB and LBBB, RBBB and LAD, or RBBB with RAD) Trifascicular block (BBB with PR prolonged) Asystole Indication + + + + + + + + + + + If pacing is anticipated (rhythm disturbance on presentation), someone with wide experience of central lines should gain central venous access via the external jugular (ask ITU team) before thrombolysis. The alternative is access through a July 2006 ‘Common medical emergencies – arrhythmias’ femoral or antecubital vein. 2D echo localisation of great veins is now recommended. Consider the use of external pacing in an emergency until transvenous pacing can be established. ATRIAL FLUTTER "Saw-tooth" baseline rate about 300/minute. Variable degree of block. If ventricular response is fast, carotid massage or IV adenosine (see below) may increase block and unmask the flutter waves. Treatment: If hypotensive and unwell then urgent DC cardioversion. If the ventricular rate is fast (> 100/minute), rate control may be achieved with beta blockers and/or digoxin. The patient should be heparinised/given treatment dose low molecular weight heparin (LMWH)* and then anticoagulated with warfarin. If flutter persists, DC cardioversion may be performed electively. For recurrent flutter, discuss the possibility of catheter ablation with cardiologists. ATRIAL FIBRILLATION (see algorithm of >48 hours or <48 hours AF) • If haemodynamically compromised and of recent onset then consider DC cardioversion (+ heparinisation/treatment dose LMWH*) • If well tolerated then heparinise/give treatment dose LMWH*, arrange 2D echo and plan elective cardioversion (DC or pharmacological, eg. flecainide if ventricular function is good, amiodarone if not) after 48 hours. • If chronic and well tolerated then control ventricular response with digoxin ± verapamil or a beta-blocker. • Anticoagulate for all but emergency cardioversion. • Avoid digoxin and verapamil in Wolff-Parkinson-White syndrome (suspect if ventricular response > 200/minute and broad, variable QRS morphology). *UCLH trust often uses treatment doses of dalteparin (i.e. 100 units/kg BD, maximum 10,000 units BD) instead of unfractionated heparin infusions for AF. This is an unlicensed indication. Digitalisation: For long standing AF. (If haemodynamically unstable, then IV verapamil OR beta-blocker). Digoxin loading dose: 500 micrograms orally, then 250 micrograms after 4 hours. If rate still poorly controlled, discuss with cardiology. Maintenance digoxin dose is 125-250micrograms OD and will need to be reduced in renal failure. July 2006 ‘Common medical emergencies – arrhythmias’ ATRIAL FIBRILLATION - duration > 48 hours Anticoagulation for cardioversion (no previous thrombembolism) Full anticoagulation with warfarin Transthoracic echocardiography* (to exclude undiagnosed cardiac pathology, to identify thrombus, to determine left atrial and left ventricular size and to assess left ventricular function)** If thrombus identified, 6-8 weeks of anticoagulation with warfarin If no thrombus identified, 4 weeks of anticoagulation with warfarin DC cardioversion (full anticoagulation with warfarin) Transoesophageal echocardiography, to ensure left atrial and left appendage thrombus does not preclude cardioversion Atrial fibrillation Consider long-term anticoagulation with warfarin. Control ventricular rate. Stop antiarrhythmic drugs Sinus rhythm Continue warfarin for at least 4 weeks but consider anticoagulation for longer if recurrent AF (antiarrhythmic also). * Initial results suggest that, where available, transoesophageal echocardiography can be used to guide cardioversion, obviating the need for prolonged anti-coagulation precardioversion. Pending further studies, the above algorithm may be appropriate in selected cases where reducing either the overall duration of anticoagulation or delay before cardioversion is deemed of paramount importance. These patients will require full anticoagulation at the time of cardioversion and following cardioversion as elsewhere. ** If mitral stenosis is found, cardioversion should only be undertaken after a transoesophageal study, in consultation with a cardiologist, since cardioversion may not be appropriate. Long term warfarin is required. July 2006 ‘Common medical emergencies – arrhythmias’ July 2006 ‘Common medical emergencies – arrhythmias’ *this assumes early cardioversion. If delay occurs and overall duration of atrial fibrillation approaches 1 week, advise full anticoagulation for 4 weeks with warfarin. ** if mitral stenosis is found, cardioversion should only be undertaken after transoesophageal study in consultation with a cardiologist, since cardioversion may not be appropriate. Long term warfarin will be required. SUPRAVENTRICULAR TACHYCARDIA: Regular, narrow complex tachycardia, rate usually in the range 140-220 beats per minute. Includes: - sinus tachycardia - focal atrial tachycardia - atrial flutter - atrial fibrillation (almost regular response) - paroxysmal AV nodal tachycardia (AVNRT) - AV re-entrant tachycardia (AVRT) through accessory pathway Diagnosis: By ECG ± carotid sinus massage, valsalva, or IV adenosine. - It is especially useful to record a rhythm strip of all 12 ECG leads during vagotonic manoeuvres or adenosine administration. - AVNRT, AVRT and some focal atrial tachycardias will terminate with adenosine. - Other focal atrial tachycardias, atrial flutter and atrial fibrillation will continue but the atrial activity will be unmasked Treatment as appropriate for diagnosis (AF etc) or by interrupting re-entrant circuit: - If patient shocked or haemodynamically compromised then DC cardioversion, 50, 200, 360 J, less if patient digoxin toxic. - Adenosine IV: Monitor ECG and give fast boluses of incremental doses every 1-2 mins, eg. 3mg, 6mg, then 12mg. Avoid in asthmatics. If essential to give to patients who have taken dipyridamole within the past 24 hours, then reduce the incremental doses to 0.5-1mg, 1.5mg then 3mg every 2mins (dipyridamole potentiates plasma levels of adenosine and slows its clearance). - Verapamil IV: Boluses of 5mg over 2 mins (3 mins in elderly), at 15minute intervals to maximum of 20mg (10mg in patients with IHD or aged > 60 years). May aggravate hypotension. Avoid in patients already on a beta-blocker. If adenosine and verapamil are ineffective then reconsider the diagnosis. Is patient septic or haemorrhaging? Other drugs: July 2006 ‘Common medical emergencies – arrhythmias’ • Esmolol IV: short acting. Maintenance infusion dose of 50-200 micrograms/kg/minute by IV infusion • Dilute 2.5g esmolol ampoule to 250ml 5% glucose or NaCl 0.9% (final concentration of 10mg/ml). Infuse peripherally (large cannula if possible as irritant). • Assuming an infusion concentration of 10mg/ml: Pump setting* (ml/hr) = dose (micrograms/kg/min) x pt weight (kg) x 6 1000 (*Pump to run at above calculated rate for desired duration, i.e. 1 minute, 4 minutes or as maintenance infusion) e.g. Pump setting for a 70kg patient, for an initial loading dose of 500mcg/kg/min for 1 min: 500 x 70 x 6 = 210ml/hour for 1 minute 1000 Load: 500mcg/kg/min for 1 minute THEN Maintenance infusion: 50mcg/kg/min for 4 minutes** Response: Maintain infusion at 50mcg/kg/min Inadequate response within 5minutes: Repeat 500mcg/kg/min for 1 minute THEN Increase maintenance infusion to 100mcg/kg/min for 4 minutes** Response: Maintain infusion at 100mcg/kg/min Inadequate response within 5minutes: Repeat 500mcg/kg/min for 1 minute THEN Increase maintenance infusion to 150mcg/kg/min for 4 minutes** Inadequate response within 5minutes: Repeat 500mcg/kg/min for 1 minute THEN Increase maintenance infusion to 200mcg/kg/min for 4 minutes** and maintain • Response: Maintain infusion at 150mcg/kg/min **Note: As the desired heart rate and BP are reached, OMIT the loading infusion and reduce the incremental dose in the maintenance infusion from 50mcg/kg/min to 25mcg/kg/min or lower. Intervals between titration steps may be increased from 5 to 10minutes The safety of maintenance doses greater than 200mcg/kg/min has not been demonstrated July 2006 ‘Common medical emergencies – arrhythmias’ • Infusions of esmolol can constitute a substantial volume load; vasodilators may also be required if the volume load is problematic but the desired antihypertensive effect can not be reached with esmolol alone. Discuss other intervention/drugs with cardiology team, eg. • Flecainide IV 2mg/kg over 30 minutes (max. of 150mg) then if required an infusion of 1.5mg/kg/hour for 1hour, then 100 to 250 micrograms/kg/hour for up to 24 hours if good LV (maximum cumulative dose in first 24 hours 600mg). VENTRICULAR ARRHYTHMIAS ISOLATED VE’S (Ectopics): These are broad QRS complexes, not preceded by P-waves. Treatment: None usually needed. + - check serum K . - treat ischaemia and heart failure. MONOMORPHIC VT: More than 5 consecutive broad QRS complexes, regular rate (> 100/minute, if 60 to 100/minute = accelerated idioventricular rhythm). Treatment: - If shocked/hypotensive with sustained VT, then DC cardioversion. - Correct electrolyte abnormalities, eg. potassium and magnesium Drugs: • Lidocaine: - 50 to 100mg IV bolus (use the lower dose in lighter patients or in those whose circulation is severely impaired). NB: short duration of action (1520mins) – see BNF re repeat dosing. - If recurrent, consider a continuous lidocaine infusion after the bolus, of 4mg/minute for 30mins, then 2mg/minute for 2 hours then 1mg/minute – reduce dose further if infusion continued beyond 24hours. No more than 200-300mg lidocaine should be administered during a 1hour period - Decrease infusion regimen by half if patient has heart failure or cirrhosis. - Patients on concurrent beta-blockers (especially propranolol), should be monitored closely for signs of lidocaine toxicity (e.g. dizziness, nausea, drowsiness, speech disturbance, numbness, confusion, respiratory depression, convulsions and rarely, sinus arrest or severe bradycardia) and the infusion dose reduced accordingly. - Toxicity may be more likely to occur in the elderly (may therefore require lower infusion doses). July 2006 ‘Common medical emergencies – arrhythmias’ • If ineffective then IV amiodarone by central line (to avoid phlebitis). Load with 300mg over 60 minutes (BP may fall), then give 900mg/24 hours. NB. Incompatible with NaCl 0.9% If resistant to both drugs and recurring after DC cardioversion then consult cardiologist. Other drugs to consider include the following but may get into problems with pro-arrhythmic polypharmacy: - Flecainide (see previous page for dose) - Mexiletine: Loading dose: 100 to 250mg IV at 25mg/minute followed by infusion of 250mg over 1 hour, then 125mg/hour for 2 hours (use dilution of 500mg in 500ml of 5% glucose or NaCl 0.9%). Maintenance dose: 500 micrograms/minute (use a dilution of 250mg in 500ml of 5% glucose or NaCl 0.9%). - Sotalol 20 to 60mg IV over 10 minutes POLYMORPHIC VT / TORSADE DE POINTES - Frequently, the patient has an underlying bradycardia. It is often initiated by "late” ventricular ectopics (VE). Often self-terminating but recurrent. QT prolongation may predispose. Treat hypokalaemia, and give magnesium. Pace bradycardic patients and stop drugs which may predispose to QT prolongation. Treatment: Isoprenaline IV may be useful initially i.e. 2mg isoprenaline in 500ml 5% glucose (4mcg/ml). Start at a rate of 1 microgram/minute (15ml/hr) titrating up in steps of 1microgram/minute at intervals of 2-3minutes, until a satisfactory heart rate is achieved or adverse effects such as hypotension or ventricular arrhythmias occur (Usual max: 10micrograms/min). July 2006 ‘Common medical emergencies – arrhythmias’ DIFFERENTIAL DIAGNOSIS OF BROAD COMPLEX TACHYCARDIAS If there is a history of ischaemic heart disease then > 95% of broad complex tachycardias are VT. If in doubt treat as VT. Do not try verapamil. If an SVT with aberrant conduction (usually RBBB and < 160 msec duration) is strongly suspected, then IV adenosine should be tried. Patient unwell Yes No No history of IHD History of IHD RBBB, QRS < 160msec Adenosine IV Cardioversion or increased block Yes No Treat as SVT Treat as VT DC cardioversion July 2006 ‘Common medical emergencies – arrhythmias’