Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
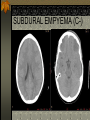
EVERYTHING A MEDICAL STUDENT SHOULD KNOW ABOUT A CT SCAN OF THE HEAD By Thanh Binh Nguyen Neuroradiologist Ottawa Hospital Last updated July 2007 What is a CAT scan? CAT scan stands for Computed Assisted Tomography Cross sectional images are obtained by multiple measurements of the x-rays attenuation from several projections. What are we measuring? The attenuation coefficient reflects the reduction in the x-ray intensity by the material relative to water. The Hounsfield Unit is the scale used. (HUwater=0, HUbone >500, HUlung=-500) CT and radiation Effective dose takes into account which tissue has absorbed what radiation dose (expressed in Sievert) We can decrease the effective dose in CT by reducing the tube current but image noise will be increased Radiation and risk of cancer 1. 2. 3. Lifetime risk of developing fatal cancer from radiation exposure in a population is 0.005% per milliSievert(mSv) Exposure from mSV Natural background 3 /yr CT head 2 CT spine 10 STROKE Canadian Stroke Facts* 40,000-50,000 new stroke’s /year 65% of survivors have disability 4th leading cause of death Longest length-ofstay for any diagnosis (37 d) Leading cause of transfer to long term care Leading cause of neuro disability in adults Cost >$2.7 billion/year $27,500 / acute stroke $46,000-$122,000 / patient for chronic care *Canadian Heart and Stroke Foundation Stroke denotes a persistent loss of neurologic function with sudden onset diverse etiologies... Ischaemic Cerebrovascular Stroke Venous Congestion / Stroke Hemorrhagic Stroke Anatomy Arterial Territories Anterior Cerebral Middle Cerebral Posterior Cerebral Basilar Superior Cerebellar Anterior Inferior Cerebellar Posterior Inferior Cerebellar Supratentorial Territories From Osborne, A: Neuroradiology Left PCA MCA ACA Anterior choroidal infarct Watershed (between ACA and MCA) Ischaemic CV Stroke Thromboembolic most common Hemodynamic Atherosclerotic Dissection Vasospasm Hypotensive /asphyxia (watershed) Migraine Vasculitis Thrombotic: hypercoagulable states Hemorrhagic Stroke Primary Intracerebral bleed Hypertensive Amyloid angiopathy Arteriovenous malformations Neoplasms Trauma Subarachnoid hemorrhage Aneurysm AVM’s Trauma Hypertensive Hemorrhage Classically involves the deep nucleii Amyloid angiopathy Hyperdense vessel sign Hyperdense vessel sign & loss of gray/white junction... Left insular ribbon sign & effacement of sulci NEOPLASM APPROACH TO BRAIN TUMOR Intra-axial(from the brain) versus Extra-axial (from the meninges or skull) Location (supratentorial vs infratentorial) Age of patient Imaging characteristics Could you this be something other than neoplasm (infarction, abscess, etc…)? CT with contrast or MRI is often needed. EDEMA Vasogenic edema: Involves white matter primarily with sparing of gray matter Seen with brain tumors, abscess Cytotoxic edema Involves both white matter and gray matter Seen with infarction BRAIN TUMORS Extraaxial: meningioma Intraaxial: Primary Glial tumors: low grade to high grade astrocytoma (glioblastoma multiforme) Non glial tumor (lymphoma, hemangioblastoma, etc…) Metastasis (lung, breast, colon, etc…) Unenhanced CT of the head shows a mass in the left frontal lobe with vasogenic edema Ring enhancing lesion (GBM) Vasogenic edema GLIOMAS Astrocytomas 85% of cerebral gliomas Young to middle-aged adults (20-50 years) Varying degree of malignancy. Highest grade is glioblastoma multiforme which presents as a mass with ill-defined margins, variable enhancement and extensive vasogenic edema. Oligodendrogliomas Young, middle-aged adult Solid, well-defined mass with calcification 70 year old gentleman complaining of dizziness and off balance for one week with associated nausea and vomiting. He also had attack of left facial numbness and left arm numbness for a week. Cerebellar exam showed nystagmus of lateral gaze and left-sided incoordination C- C+ Left tonsillar herniation C- C+ C- C+ Hyperdense cerebellar mass seen on plain CT scan which enhances homogeneously and causes compression of the 4th ventricle and hydrocephalus C- C+ DIAGNOSIS BURKITT LYMPHOMA Ct scan of the head with contrast in patient with renal cell carcinoma Enhancing nodule at corticomedullary junction Vasogenic edema: involves whiter matter more than gray matter DIAGNOSIS METASTASES Hematogenous seeding to corticomedullary junction Usually in MCA territory Usually the degree of edema is out of proportion to the size of the lesion Ct scan of the head without contrast Hyperdense mass Enhances homgeneously and appears extraaxial Thickening of the adjacent bone (hyperostosis) DIAGNOSIS MENINGIOMA INFECTION INTRACRANIAL INFECTION Intraaxial: Encephalitis Cerebritis Abscess Extraaxial: Subdural empyema Epidural abscess Meningitis CEREBRAL INFECTION Encephalitis: generalized and difuse infection of the brain. Often of viral origin (ex.herpes simplex) Cerebritis: localized but poorly demarcated area of parenchymal softening. Abscess: follows cerebritis. Occurs when a central zone of necrosis becomes encapsulated. MODE OF SPREAD Hematogenous spread: could reach the corticomedullary junction or leptomeninges. Direct extension: ex.sinusitis leading to epidural abscess or subdural empyemas Spread along the nerves (ex.herpes encephalitis along the trigeminal nerve) ABSCESS (could look similar to metastatic lesion on CT) Ring enhancing lesion Vasogenic edema SUBDURAL EMPYEMA (C-) SUBDURAL EMPYEMA (C+) TUBERCULOSIS Basal leptomeningitis (seeding of the subarachnoid space) TUBERCULOSIS Multiple tuberculomas seen on MRI exam with contrast THE END