Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adipose tissue wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Cigarette smoking for weight loss wikipedia , lookup
Calorie restriction wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Human nutrition wikipedia , lookup
Abdominal obesity wikipedia , lookup
Wilson's disease wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
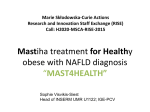
RESEARCH Review The Role of Diet and Nutrient Composition in Nonalcoholic Fatty Liver Disease Erin Marie McCarthy, MS, RD, LDN; Mary E. Rinella, MD ARTICLE INFORMATION ABSTRACT Article history: Nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in the developed world. NAFLD is tightly linked to insulin resistance and considered to be the hepatic manifestation of the metabolic syndrome. The cornerstone of any treatment regimen for patients with NAFLD is lifestyle modification focused on weight loss, exercise, and improving insulin sensitivity. Here we review the literature and discuss the role of diet and nutrient composition in the management of NAFLD. Because there are currently no specific dietary guidelines for NAFLD, this review proposes a dietary framework for patients with NAFLD based on the available evidence and extrapolates from dietary guidelines aimed at reducing insulin resistance and cardiovascular risk. J Acad Nutr Diet. 2012;112:401-409. Accepted 30 September 2011 Keywords: Nutrition Obesity NAFLD/NASH Fatty liver Copyright © 2012 by the Academy of Nutrition and Dietetics. 2212-2672/$36.00 doi: 10.1016/j.jada.2011.10.007 N ONALCOHOLIC FATTY LIVER DISEASE (NAFLD) IS THE most common cause of chronic liver disease in the developed world (1). NAFLD is a significant health problem and affects 70 million adults in the United States (⬃30% of the adult population). NAFLD encompasses a spectrum of liver disease that ranges from simple steatosis to nonalcoholic steatohepatitis (NASH), its progressive subtype. An estimated 20% of patients with NAFLD have NASH, which can progress to cirrhosis necessitating liver transplantation. NAFLD in both forms represents the hepatic manifestation of the metabolic syndrome that also includes dyslipidemia, central obesity, hypertension, and insulin resistance (IR) (2). Most patients with fatty liver have excess body weight. Although promising pharmacologic therapies are emerging, sustained weight loss is the most effective treatment for NAFLD and should be the foundation of any treatment plan. A thorough discussion of the pathophysiology of NAFLD is beyond the scope of this review; however, how obesity and dietary composition affects hepatic fat accumulation and inflammation will be briefly discussed. Obesity itself represents a chronic, inflammatory condition resulting from the failure of the normal homeostatic regulation of energy intake, storage, and use (3,4). In the setting of obesity, particularly central obesity, there is an expansion of active visceral adipose tissue. This adipose tissue compartment becomes infiltrated by inflammatory cells that lead to a milieu in which proinflammatory cytokines such as tumor necrosis factor ␣ and interleukin-6 increase while adiponectin, which counteracts the effects of tumor necrosis factor ␣, decreases (1). This leads to hepatic steatosis and a state of heightened IR and increased oxidative injury. Weight loss can change the activity of adipose tissue Meets Learning Codes 5000, 5240, 5370, 9000, and 9020. To take the Continuing Professional Education quiz for this article, log in to www.eatright.org, click the “My Profile” link under your name at the top of the homepage, select “Journal Quiz” from the menu on your myAcademy page, click “Journal Article Quiz” on the next page, and then click the “Additional Journal CPE Articles” button to view a list of available quizzes, from which you may select the quiz for this article. © 2012 by the Academy of Nutrition and Dietetics. and reverse many of these consequences as can, potentially, dietary macronutrient content (see the Figure). In the setting of excessive nutrient intake, diets rich in fat or carbohydrate can decrease insulin sensitivity and increase serum free fatty acid levels, leading to hepatic steatosis. A critical review of diets for the metabolic syndrome and popular diets as they might relate to NAFLD is discussed elsewhere (5). This review discusses the existing data on the effects of diet-induced weight loss and dietary composition and proposes a rational dietary approach that promotes slow and controlled weight loss designed to improve insulin sensitivity and reduce cardiovascular risk in patients with NAFLD. METHODS Articles featured in this review were identified through an electronic database search using PubMed with dates ranging from 1990 through 2011. Randomized controlled trials, case control studies, and observational studies of adult patients were included. The search terms used for this review included: fatty liver disease, fatty liver nutrition, NASH nutrition, NASH diet, fructose NAFLD, saturated fat liver, carbohydrate metabolic syndrome, insulin resistance and diet, antioxidants, and bariatric surgery. Effects of Weight Loss on NAFLD Although the liver is not meant to store fat, excess energy and unmatched energy expenditure can result in the accumulation of fat in the liver. Weight management, dietary macronutrient composition, physical activity, and behavior therapy all play a critical role in successful weight loss. Patients with NAFLD have been shown to have higher energy intake when compared with healthy controls (6). Long-term wellcontrolled dietary intervention studies are limited; however, the preponderance of the evidence suggests that it is effective in improving liver disease related to NAFLD because it improves insulin sensitivity, hypertension, and dyslipidemia. Several studies show that diet-induced weight loss reduces liver enzymes and hepatic steatosis, with less consistent effects on other components of liver histology (7-9). In patients with NASH, some studies have shown that a 1,400 kcal/day diet and weight loss of ⬃3.5 kg improve histology on liver biopsy and liver enzyme levels (10). In the largJOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 401 RESEARCH Figure. Adipose tissue undergoes significant transformation during weight gain that is characterized by adipocyte hypertrophy and infiltration by macrophages. These changes lead to an increased rate of adipocyte apoptosis and the secretion of a host of proinflammatory cytokines from both adipocytes and macrophages. This chronic inflammatory state then promotes insulin resistance. Hepatic steatosis develops as a result of increased adipose tissue lipolysis and an adipocytokine profile that promotes insulin resistance, lipogenesis, and impairs fatty acid oxidation and export. Weight loss can reverse this process and thereby restore insulin sensitivity and reduce hepatic fat accumulation and inflammation. est randomized controlled trial of lifestyle intervention in NASH, patients were randomized 2:1 to a combination of diet, exercise, and behavior modification (lifestyle intervention group) or a control group, with a goal of 7% to 10% weight reduction (11). The primary outcome measure was an improvement in the NAFLD activity score after 48 weeks of treatment. Subjects in the lifestyle intervention group (n⫽21) were assigned an energy goal based on their starting weight (1,000 to 1,200 kcal/day if baseline weight ⬍200 lb or 1,200 to 1,500 kcal/day if baseline weight ⬎200 lb) and were instructed to consume a 25% fat diet. Participants in the control group (n⫽10) attended group sessions providing basic education about NASH and principles of healthy eating and physical activity. The lifestyle intervention group had an average weight loss of 9.3% of their weight compared with only 0.2% in the control arm (P⫽0.005). Furthermore, after treatment, NAFLD activity score was lower in the lifestyle intervention group compared with the control group (P⫽0.05). Those who lost ⱖ7% of their body weight had significant improvements in steatosis (P⬍0.001), lobular inflammation (P⫽0.03), and NAFLD activity score (P⬍0.001). Although weight loss is the most effective treatment for NAFLD, excessive energy restrictions and sudden weight loss may worsen liver injury (12). In fact, rapid weight loss (⬎2.5 lb/week) as seen in antiquated bariatric procedures such as the jejunoileal bypass often worsened steatohepatitis or resulted in cirrhosis and liver failure (13,14). In patients with NAFLD, particularly those with advanced liver disease, slow and controlled weight loss over time is the goal. Short-term and pilot studies have shown that a 25 kcal/kg/day diet or a reduction of ⬃200 kcal/day produces significant decreases in aspartate aminotransferase, alanine aminotransferase (ALT), fasting glucose, body mass index, and the degree of hepatic steatosis (9,15). Modest weight loss, ⬍2 lb (1 kg) per week, is associated with a decrease in the incidence of the metabolic syndrome and improvement in the histologic features of NASH in ⬎80% of cases (16). As little as 5% weight loss can have beneficial effects on NAFLD, although an initial 10% weight loss is typically recommended and supported by the National Heart, Lung, and Blood Institute–National Institute of Diabetes and Digestive and Kidney Diseases clinical guidelines (17). To avoid rapid weight fluctuations, the recommended rate of weight loss is 1 to 2 lb/week (17). 402 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS Influence of Dietary Macronutrients Aside from the possibility of achieving weight loss through caloric restriction as a treatment of NAFLD, dietary composition can directly influence the development of NAFLD. Various types of diets (either low in carbohydrates or low in fats) are equally effective for long-term weight reduction (18). However, there is evidence that manipulation of either micronutrient or macronutrient content can affect hypertension, levels of inflammation, serum lipids, and IR independent of weight loss (19-21). This is illustrated by the differences in recommended macronutrient content by various societies (Table 1). Animal data and observational studies suggest that a diet high in carbohydrates worsens liver injury related to NAFLD. Although no prospective study has compared the effects of popular fad diets on patients with NAFLD, this is thoroughly reviewed elsewhere (5). Carbohydrate Extrapolating from the diabetes literature and available data on NAFLD, the percentage of carbohydrate in the diet and the Glycemic Index (GI) value of the carbohydrates is likely to have an important influence on NAFLD (22). Diets enriched in carbohydrate lead to increased circulating insulin concentrations, which contribute to elevated fasting triglyceride concentrations even under isocaloric conditions (23,24). A low-fat, high-carbohydrate diet promotes the development of fatty liver via increased de novo fatty acid synthesis (25). In patients with the metabolic syndrome and NAFLD, a diet containing more carbohydrate and less fat has been associated with greater histologic severity (26). In one study, patients consuming ⬎54% of energy from carbohydrates compared with those consuming ⬍35% had a 6.5-fold increased risk of hepatic inflammation (27). Ryan and colleagues (28) randomized patients to hypocaloric diets containing either 60% carbohydrate/25% fat or 40% carbohydrate/45% fat (15% protein in both) of equal energy deficit (750 kcal/day) for 16 weeks. Patients receiving the lower carbohydrate diet had lower ALT concentrations compared with those given a high-carbohydrate/ low-fat diet, despite equal weight loss. This suggests that a hypocaloric, lower carbohydrate diet may be beneficial to patients with NAFLD, independent of weight loss (28). In another study (29), patients with NAFLD following an energy-restricted (1,200 March 2012 Volume 112 Number 3 RESEARCH Table 1. Diets for a healthy lifestyle,a as recommended by authoritative groups in the United States Group Component American Heart Association Academy of Nutrition and Dietetics US Department of Agriculture Fruits 4 servings 2-4 servings 1.5-2 c Vegetables 3-4 servings 3-5 servings 2-3 c Whole grains 6 servings 6 servings 6 oz grains Lean meat 3-6 oz (cooked) 2-3 servings 5.5-6.5 oz Low-fat dairy 2-3 servings 2-3 servings 3c Fat/oils 2 servings Avoid trans & saturated 5-6 tsp 3 oz whole grains Nuts, seeds 3-4 servings/wk Sweets 0 servings Cut back on snacks Include Weight Loss 2500 kcal/d No fad diets 1 lb/wk Count kilocalories 150-200 kcal/d Discretionary energy Physical activity 2 h 30 min/wk moderate-intensity cardio Exercise regularly ⱖ2 d/wk resistance training Energy balance Nutrient-dense foods ⱖ30 min/d moderate-intensity 60 min/d prevent weight gain 60-90 min/d maintenance weight loss a All dietary recommendations represent servings per day based on a 1,600 kcal/d diet. to 1,500 kcal/day) diet were compared with patients with NAFLD following a carbohydrate-restricted (⬍20 g/day) diet. Both groups had similar weight loss. Weight loss resulted in a reduction in hepatic fat by magnetic resonance spectroscopy; however, patients following the low carbohydrate diet had a more dramatic reduction in hepatic triglyceride level (55%) compared with the control group (28%) (P⫽0.008) (29). Simple Carbohydrates. Consumption of simple carbohydrates has increased during the past few decades and the role of fructose and sucrose (which is 50% fructose) in metabolic disorders has been reviewed extensively (30,31). Dietary fructose consumption in industrialized countries has increased in parallel with the increase in NAFLD, obesity, and diabetes and some studies have suggested a direct association (32,33). The increased consumption of high fructose corn syrup, primarily in the form of soft drinks, is linked with complications of the metabolic syndrome and an increase in liver enzymes (34,35). Unlike glucose, fructose stimulates de novo fatty acid synthesis directly and promotes weight gain. Interestingly, unlike glucose, fructose does not stimulate insulin or leptin secretion, effectively bypassing normal satiety signals that are integral to the regulation of food intake and body weight. Moreover, a recent study compared 16 healthy men who received a high-energy, high-fructose diet to eight subjects following an isocaloric diet for 7 days. Those receiving fructose had an increase in hepatic fat deposition and decreased hepatic insulin sensitivity (36). Thus, ingestion of sweetened beverages with fructose or sucrose may lead to changes in long-term energy balance in the central nervous system that favor increased energy consumption and weight gain. Furthermore, fructose consumption may be proinflammatory and activate cellular stress pathways such as the unfolded protein response directly (37). shown to decrease total cholesterol levels (38,39). Although there are no studies in human beings examining the effects of GI specifically in patients with NAFLD, the effects of the GI on other comorbidities associated with NAFLD suggest that GI may be an important factor to consider when giving dietary recommendations to patients with NAFLD (22). A low-GI diet alone does not improve hepatic insulin sensitivity but in conjunction with exercise it does reduce post-prandial hyperinsulinemia (40). A randomized controlled trial by Fraser and colleagues (41) found that ALT levels decreased by 35% in patients following a low-carbohydrate/low-GI diet when compared with those following a highcarbohydrate/high-GI diet (P⬍0.05). Given the available evidence it is reasonable to favor the incorporation of lower GI foods into a diet for patients with NAFLD. However, the GI is a gross measurement whose direct influence on NAFLD remains unknown. Fat Increased fat intake has been linked to insulin resistance and impaired postprandial lipid metabolism. Western diets contain more saturated fat, vegetable oil rich in n-6 polyunsaturated fatty acid (PUFA), and less n-3 PUFA. Patients with NASH ingest a higher percentage of their energy from fat (37%) and this may be an independent nutritional risk factor for the development or progression of NAFLD (odds ratio [OR]⫽2.51) (42,43). In a study by Yamamoto and colleagues (15) the reduction of fat consumption from 27% to 19% for 6 months decreased aspartate aminotransferase and ALT from 68 IU/L and 104 IU/L to 33 IU/L and 42 IU/L, respectively. Although few studies on fat intake exist on which to base recommendations for NAFLD, evidence supports the benefits of a Mediterranean diet for patients with the metabolic syndrome, through improving insulin sensitivity and reducing cardiovascular risk, both of which would be beneficial to patients with NAFLD (44-46). GI Low-GI foods, also called slow release carbohydrates exert a second meal effect whereby the glycemic response to the subsequent meal is enhanced. Furthermore, such foods (eg, oats) have been March 2012 Volume 112 Number 3 Saturated/Trans-Fatty Acids. Saturated fatty acids (SFA) have adverse effects on lipid and glucose homeostasis, which in turn worsen the progression of metabolic syndrome and possibly NAFLD (47). JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 403 RESEARCH Two studies in patients with fatty liver further support this association, and have shown that NAFLD patients consume more SFA while consuming less PUFA, fiber, and antioxidants (33,48). However, whereas diets containing ⬍10% SFA are likely to be beneficial, extreme reductions in SFA may have deleterious effects on plasma lipid levels. In a double blind randomized controlled trials of two reduced-fat diets (30% fat with 9% SFA or 25% fat with 6% SFA) compared with a control (38% fat with 14% SFA) in healthy men, both reduced-fat diets reduced low-density lipoprotein cholesterol levels. Interestingly, high-density lipoprotein cholesterol levels also decreased and triglyceride levels increased after the 6-week intervention. This effect was most pronounced in insulin resistant or overweight subjects in whom low-density lipoprotein cholesterol level benefits were less pronounced and unfavorable changes in high-density lipoprotein cholesterol and triglyceride were more prominent (49). This suggests that although reduced SFA intake (⬍10%) might be beneficial to patients with NAFLD, intake of ⬍6% may have counterproductive effects on plasma lipid levels. Although no studies in human beings have made a direct link between NAFLD and diets high in SFA, experimental evidence in rodents demonstrates that high dietary SFA consumption worsens IR, NAFLD, and cardiovascular disease in rats (50-52). Monounsaturated Fat. Compared with high-carbohydrate diets, diets high in monounsaturated fat (MUFA) may be preferable if they are not coupled with increased energy intake or contain higher quantities of cholesterol. An increase in MUFA intake, especially as a replacement for SFA, may offset the proinflammatory effects of SFA and decrease IR and hepatic steatosis. Epidemiologic studies have shown anti-inflammatory and cardiovascular benefits of a Mediterranean-style diet rich in MUFA (46,53). There appears to be a direct beneficial role of olive oil (73% MUFA) in improving plasma lipid levels in the treatment of the metabolic syndrome (54). An olive oil-rich diet decreases the accumulation of triglycerides in the liver as well as improves postprandial triglyceride level and glucose response in subjects with IR (55). Incorporating MUFA into Western dietary patterns, particularly at the expense of SFA, may reduce the risk of metabolic syndrome and NAFLD/NASH. PUFA. PUFAs of the n-3 and n-6 series are essential fatty acids that must be provided by the diet. Fish oils, rich in eicosapentaenoic and docosahexaenoic acids, are the most biologically active n-3 PUFAs and exhibit protective effects. They promote oxidation of fatty acids via peroxisome proliferator-activated receptor-␣ activation and downregulate fatty acid synthesis (56,57). In insulin resistant animal models, the consumption of a diet high in n-3 PUFA has favorable effects on the regulation of plasma lipid levels, cardiovascular disease, immune function, and insulin (58). Three recent clinical trials in human beings support these findings by showing that n-3 PUFA administration (1.0 to 2.7 g/day for 6 to 12 months) to patients with NAFLD improved hepatic steatosis, inflammation, and fibrosis (59-61). Capanni (59) and Spadaro (60) both demonstrated that triglyceride level decreased an average of 25 to 37 mg/dL (0.28 to 0.39 mmol/L) when supplemented with 1 g PUFA/day for 6 and 12 months, respectively. Furthermore, other studies have shown that increased n-3 PUFA consumption improves dyslipidemia related to the metabolic syndrome and cardiovascular disease (62,63). Supplementation with n-3 PUFA decreases plasma triglyceride levels by 25% and by 50% in individuals with normolipemia and hypertrigliceridemia, respectively (2,3). Specifically, because the dyslipidemia of NAFLD is characterized by high triglyceride level and low high-density lipoprotein cholesterol level, n-3 PUFA supplementation is likely to be beneficial. Alpha-linoleic acid, found in walnuts, may also be of benefit by reducing triglyceride levels and raising high-density lipoprotein cholesterol level (64). Low levels of circulating n-3 PUFA are associated with higher de novo lipogenesis (ie, increasing intrahepatic saturated fat content), increased hepatic uptake of circulating free fatty acids and decreased fatty acid oxidation, all of which can worsen hepatic steatosis (65). The available data suggest that decreased intake of n-3 fatty acids could have an 404 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS adverse effect on NAFLD and its associated comorbidities. Therefore, higher consumption of fish rich in n-3 PUFAs or walnuts may reduce the risk for NAFLD or improve the dyslipidemia that characteristically accompanies it (33). Protein Very few clinical studies have examined the effect of protein consumption in subjects with metabolic syndrome or NAFLD. Protein intake, expressed as the percentage of energy from protein, has generally not been reported to be altered in NAFLD, although ZelberSagi and colleagues (33) found significantly higher meat protein consumption in NAFLD after adjustment for age, sex, body mass index, and total energy intake. Animal data suggest that soy protein may reduce hepatic lipogenesis and improve insulin sensitivity (48,66). In human beings, there is only one study suggesting that the short-term consumption of soy protein as part of a low-energy diet may provide an additional benefit for weight reduction in subjects with obesity (67). Currently, conclusive evidence is lacking to make a definitive statement regarding the effect of dietary protein on NAFLD. Protein is well represented in the American diet, thus deficiency is unlikely. Excess protein intake can have untoward effects on renal function in susceptible individuals (68,69). Promoting Sustained Weight Loss Maintenance of weight loss is one of the biggest challenges of dietary interventions. Although the data are incomplete, most evidence suggests that the vast majority of people who lose weight regain it during the subsequent months or years (70,71). Several variables have been related to weight loss maintenance such as increased moderateintensity physical activity 60 min/day, eating breakfast daily, increases in emotional support, and less sugar-sweetened soft drink consumption (70,72). Also, improved weight loss maintenance is associated with creating long-term goals, taking personal responsibility for weight management, and self-monitoring (73). Obesity surgery provides the most effective therapy for sustained weight loss (74). The effects of bariatric surgery on NAFLD are encouraging and are reviewed extensively elsewhere (74,75). For weight maintenance, meal replacements in combination with regular physical activity can be used to get patients back on track if they start to regain weight (75,76). To date, it remains largely unknown how effective weight loss maintenance interventions are in clinical or community practice settings. Understanding Barriers to Maintaining Weight Loss. Maintenance of weight loss can be difficult to achieve due to physical, economic, or other barriers in patients’ lives. In patients with advanced liver disease, it is particularly important to achieve slow and sustained weight loss because large fluctuations in weight can exacerbate liver injury and result in liver dysfunction. Patients with NAFLD often have other medical conditions such as diabetes, heart disease, or immobility. Furthermore, economic limitations, work schedules, or limited access to good quality food can make maintaining healthy eating habits difficult. It is important to keep these limitations in mind when designing a weight loss plan for patients. Sustainable changes in lifestyle that naturally result in weight loss over time should be the goal, rather than weight loss itself through any specific dietary intervention. Behavior Modification. Dietary modification is most successful when accompanied by behavioral modification. Only a behavioral approach may give patients the practical instruments to achieve their dietary and exercise goals, incorporate them into their lifestyle, and maintain the results for a prolonged period. Cognitive-behavior treatment should be provided to patients at risk of advanced liver disease (77). Increased effectiveness is associated with increased contact frequency and using self-regulatory behavior change techniques (eg, goal setting and self-monitoring). Moscatiello and colleagues (78) examined NAFLD subjects and compared a cognitivebehavior treatment program to a prescriptive diet group. The cognitive-behavior treatment program consisted of 13 weekly sessions, 120 minutes each supported by the LEARN program for weight March 2012 Volume 112 Number 3 RESEARCH Table 2. The effects of nutrient supplements on nonalcoholic fatty liver disease Supplement Study Vitamins Type Sanyal and colleagues, RCTb 2010 (87) n⫽84 Liver histology Liver enzymes resulta resulta Duration Dose 96 wk 800 IU vitamin E daily vs 2* placebo 2 Standard diet/exercise recommendations Foster and colleagues, RCT 2011 (91) N⫽1,005; nonalcoholic fatty liver disease n⫽80 3.6 y Sanyal and colleagues, Pilot study; RCT 2004 (89) n⫽20 6 mo 1,000 IU vitamin E, 1,000 2* mg vitamin C Atorvastatin Vitamin E 400 IU daily 2** 2 c NHLBI guidelines for diet Kugelmas and colleagues, 2003 (90) Pilot study n⫽16 6 wk Harrison and colleagues, 2003 (92) RCT n⫽45 6 mo 2** 800 IU vitamin E daily Step 1 AHA diet ⫹ exercise d Vitamin E 1,000 IU ⫹ vitamin C 1,000 mg 2 fibrosis ... Or placebo daily Low-fat diet (30 g/d) 20 g daily or placebo 2** NAe 6 mo NA NA 2 Observational n⫽5,944 6y NA NA 2 Control trial n⫽42 4 mo NA 2 Betaine Abdelmalek and colleagues, 2009 (97) RCT n⫽35 Caffeine Modi and colleagues, 2010 (107) Observational n⫽177 Ruhl and Everhart, 2005 (109) Loguercio and colleagues, 2005 (100) Probiotics 12 mo NHANES IIIf Probiotic VSL #3g a 2⫽Decreased/improved. RCT⫽randomized controlled trial. c NHLBI⫽National Heart, Lung, and Blood Institute. d AHA⫽American Heart Association. e NA⫽not applicable. f NHANES III⫽Third National Health and Nutrition Examination Survey. g VSL Pharmaceuticals, Inc. ©2011 Sigma-Tau Pharmaceuticals, Inc. *P⬍0.001. **P⬍0.05. b control. At 2 years, cognitive-behavior treatment was associated with increased weight loss (OR⫽2.56), normalization of liver enzymes (OR⫽3.57), and a higher probability of maintaining weight loss. Evidence for long-term effectiveness for weight loss and dietary interventions emphasizes the role of cognitive-behavior treatment in the treatment of NAFLD (79). Physical Activity. Exercise, in the absence of weight loss, improves skeletal muscle insulin sensitivity, which may improve IR in patients with NAFLD (80,81). On average, subjects who increased moderate-vigorous physical activity to a level of 150 minMarch 2012 Volume 112 Number 3 utes/week or more have the greatest improvements in liver enzymes independent of weight loss (82,83). There are clear benefits of exercise on NAFLD (84,85); however, a thorough discussion is beyond the scope of this review. Incorporating physical activity has many benefits and should be part of any healthy lifestyle. Nutrient and Antioxidant Treatments Oxidative injury is a well-accepted cause of liver injury in NASH. Vitamin E is the best-studied antioxidant for the treatment of JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 405 RESEARCH Table 3. Proposed lifestyle modification guidelines for persons with nonalcoholic fatty liver disease/nonalcoholic steatohepatitis Modification Guideline Weight loss Initial goal: 5-10% body weight lost over 1 y Long-term goal: ideal body weight Maintenance of weight loss Energy intake 1,200-1,500 kcal/d Total fat intake ⬍35% of total energy Monounsaturated fatty acid intake Up to 25% Polyunsaturated fatty acid intake Increase n-3 fatty acids Saturated fatty acid intake ⬍7% of total energy Carbohydrate intake ⱖ50% whole grain; avoid highfructose corn syrup Protein intake Lean animal- or vegetable-based protein Antioxidant intake Vitamin E 800 IU/d Fish oil 1 g/d (eicosapentaenoic ⫹ docosahexaenoic acids) Physical activity ⱖ150 min/wk at moderatevigorous intensity Cardiovascular 5 times/wk Resistance training ⱖ2 times/wk NAFLD. Many small studies have addressed the efficacy of various nutrient and antioxidant therapies, many of which are discussed below. Table 2 summarizes the largest studies of antioxidants in patients with NAFLD. The available evidence for other antioxidants requires further study before any conclusions can be drawn. Vitamin E. Patients with NASH have been shown to have lower intakes of the antioxidant vitamin E (48). Vitamin E supplementation suppresses lipid peroxidation and oxidative stress, which improves inflammation and fibrosis in patients with NASH (86). Several studies have shown significant improvements in hepatic steatosis with 800 and 1,000 IU/day (87-90). In the largest randomized controlled trial to date, Sanyal and colleagues (87) evaluated the effectiveness of vitamin E in 247 patients with NASH. After 96 weeks of treatment, vitamin E (800 IU/day) improved liver histology compared to placebo (87). Despite not improving insulin resistance, vitamin E met the primary endpoint of improving the NAFLD activity score. Others have looked at the combination of vitamins C and E (91). Harrison and colleagues (92) randomized 45 patients with NASH to 1,000 mg vitamin C and 1,000 IU vitamin E or placebo daily for 6 months. Fibrosis improved to a significant degree in those treated with vitamins C and E. There were no improvements in inflammation/necrosis scores or ALT levels with vitamin E and C supplementation. Although the risk is believed to be low, certain high-dosage (ⱖ400 IU/day) trials have shown an increase in all-cause mortality and clinicians should be mindful of this when considering supplementation with vitamin E (93). 406 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS Betaine. Betaine (trimethylglycine) is a precursor of S-adenosyl methionine, a hepatoprotective factor. Therapeutic effects of betaine on NAFLD have been reported in both clinical and experimental studies (94,95). Betaine may improve in adipose tissue function, which could have beneficial effects on the development of NAFLD (96). However, clinical data have not shown dramatic effects. In the only randomized placebo-controlled study of betaine (20 g daily) in 55 patients with NASH, betaine had no affect on liver enzymes or histology when compared with placebo (97). Therefore, although mechanistically one could foresee a benefit in NASH, larger clinical studies may be needed to show a benefit. Probiotics. Probiotics are live microbial food supplements or components of bacteria and may have beneficial effects on human health. Emerging data suggest that modifications of the gut microbiota may play a role in the development of NAFLD and progression to NASH (98). No randomized clinical trials have been done on probiotics and NAFLD. Preliminary data from two pilot nonrandomized studies suggested that probiotics may improve liver chemistry tests and may decrease markers of lipid peroxidation (99,100). Other Nutrients that May have Hepatoprotective Effects. Ginger (Zingiber officinale) has medicinal properties that could be beneficial to patients with NAFLD. Small, mostly animal, studies suggest it has antioxidant properties and can improve insulin sensitivity and reduce hepatic fat content (101). Genistein, a soy isoflavone, has been shown to improve insulin sensitivity in insulin resistant animal models and improved oxidative stress in animals with NASH (102-104). Studies in human beings have not been published and, thus, nutritional supplementation with genistein cannot be recommended. Animal data and several observational studies in human beings suggest that caffeine may have a hepatoprotective role (105-109). The mechanisms by which caffeine— specifically coffee, as suggested by some—protect the liver are not well understood. CONCLUSIONS NAFLD leads to substantial morbidity and mortality in the United States and other developed countries. Although pharmachologic therapies are lacking, sustained and gradual weight loss is the most effective treatment for NAFLD. Early identification and treatment could prevent the development of cirrhosis, cardiovascular disease, and diabetes mellitus in this population. Lifestyle modification through diet and exercise must be the cornerstone of any treatment plan for patients with NAFLD (see Table 3). Long-term, moderate weight loss through the reduction of energy intake and regular physical exercise is recommended for patients with NAFLD. The influence of the macronutrient composition of the diet is important and can help reduce hepatic fat and inflammation. The role of weight loss in the treatment of fatty liver is well established. Based on data from cardiovascular or diabetes trials and limited studies in patients with NAFLD, a diet that is lower in carbohydrates and saturated fat and higher in lean protein, fiber, and n-3 PUFA is likely to be beneficial. Vitamin E supplementation reduces liver enzymes and improves liver histology in patients with NASH but without diabetes; however, sufficient evidence for other antioxidants or nutritional supplements is lacking. Therefore, well-designed dietary intervention trials are needed to create definitive evidence-based dietary guidelines for patients with NAFLD. References 1. Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology. 1999;116(6): 1413-1419. 2. Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology. 2003;37(4): 917-923. March 2012 Volume 112 Number 3 RESEARCH diet in patients with 101(10):2247-2253. NAFLD. Am J Gastroenterol. 2006; 3. Dandona P, Aljada A, Bandyopadhyay A. Inflammation: The link between insulin resistance, obesity and diabetes. Trends Immunol. 2004;25(1):4-7. 27. 4. Kaplan LM. Leptin, obesity, and liver disease. Gastroenterology. 1998;115(4):997-1001. Solga S, Alkhuraishe AR, Clark JM, et al. Dietary composition and nonalcoholic fatty liver disease. Dig Dis Sci. 2004;49(10):1578-1583. 28. 5. Zivkovic AM, German JB, Sanyal AJ. Comparative review of diets for the metabolic syndrome: Implications for nonalcoholic fatty liver disease. Am J Clin Nutr. 2007;86(2):285-300. Ryan MC, Abbasi F, Lamendola C, Carter S, McLaughlin TL. Serum alanine aminotransferase levels decrease further with carbohydrate than fat restriction in insulin-resistant adults. Diabetes Care. 2007; 30(5):1075-1080. 6. Capristo E, Miele L, Forgione A, et al. Nutritional aspects in patients with non-alcoholic steatohepatitis (NASH). Eur Rev Med Pharmacol Sci. 2005;9(5):265-268. 29. 7. Park HS, Kim MW, Shin ES. Effect of weight control on hepatic abnormalities in obese patients with fatty liver. J Korean Med Sci. 1995; 10(6):414-421. Browning JD, Baker JA, Rogers T, Davis J, Satapati S, Burgess SC. Short-term weight loss and hepatic triglyceride reduction: Evidence of a metabolic advantage with dietary carbohydrate restriction. Am J Clin Nutr. 2011;93(5):1048-1052. 30. 8. Andersen T, Gluud C, Franzmann MB, Christoffersen P. Hepatic effects of dietary weight loss in morbidly obese subjects. J Hepatol. 1991;12(2):224-229. Bacon BR, Park CH, Fowell EM, McLaren CE. Hepatic steatosis in rats fed diets with varying concentrations of sucrose. Fundam Appl Toxicol. 1984;4(5):819-826. 31. 9. Ueno T, Sugawara H, Sujaku K, et al. Therapeutic effects of restricted diet and exercise in obese patients with fatty liver. J Hepatol. 1997; 27(1):103-107. Dekker MJ, Su Q, Baker C, Rutledge AC, Adeli K. Fructose: A highly lipogenic nutrient implicated in insulin resistance, hepatic steatosis, and the metabolic syndrome. Am J Physiol Endocrinol Metab. 2010; 299(5):E685-E694. 32. 10. Huang MA, Greenson JK, Chao C, et al. One-year intense nutritional counseling results in histological improvement in patients with non-alcoholic steatohepatitis: A pilot study. Am J Gastroenterol. 2005;100(5):1072-1081. Assy N, Nasser G, Kamayse I, et al. Soft drink consumption linked with fatty liver in the absence of traditional risk factors. Can J Gastroenterol. 2008;22(10):811-816. 33. 11. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51(1):121-129. Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, et al. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): A population based study. J Hepatol. 2007;47(5):711-717. 34. 12. Clark JM. Weight loss as a treatment for nonalcoholic fatty liver disease. J Clin Gastroenterol. 2006;40(suppl 1):S39-S43. Thuy S, Ladurner R, Volynets V, et al. Nonalcoholic fatty liver disease in humans is associated with increased plasma endotoxin and plasminogen activator inhibitor 1 concentrations and with fructose intake. J Nutr. 2008;138(8):1452-1455. 13. Luyckx FH, Desaive C, Thiry A, et al. Liver abnormalities in severely obese subjects: Effect of drastic weight loss after gastroplasty. Int J Obes Relat Metab Disord. 1998;22(3):222-226. 35. Ouyang X, Cirillo P, Sautin Y, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol. 2008;48(6):993-999. 36. 14. Cotler SJ, Vitello JM, Guzman G, Testa G, Benedetti E, Layden TJ. Hepatic decompensation after gastric bypass surgery for severe obesity. Dig Dis Sci. 2004;49(10):1563-1568. Le KA, Ith M, Kreis R, et al. Fructose overconsumption causes dyslipidemia and ectopic lipid deposition in healthy subjects with and without a family history of type 2 diabetes. Am J Clin Nutr. 2009; 89(6):1760-1765. 15. Yamamoto M, Iwasa M, Iwata K, et al. Restriction of dietary calories, fat and iron improves non-alcoholic fatty liver disease. J Gastroenterol Hepatol. 2007;22(4):498-503. 37. Collison KS, Saleh SM, Bakheet RH, et al. Diabetes of the liver: The link between nonalcoholic fatty liver disease and HFCS-55. Obesity (Silver Spring). 2009;17(11):2003-2013. 38. 16. Kim CH, Younossi ZM. Nonalcoholic fatty liver disease: A manifestation of the metabolic syndrome. Cleve Clin J Med. 2008;75(10): 721-728. Anderson JW, Randles KM, Kendall CW, Jenkins DJ. Carbohydrate and fiber recommendations for individuals with diabetes: A quantitative assessment and meta-analysis of the evidence. J Am Coll Nutr. 2004;23(1):5-17. 17. Executive summary of the clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. Arch Intern Med. 1998;158(17):1855-1867. 39. 18. Strychar I. Diet in the management of weight loss. Can Med Assoc J. 2006;174(1):56-63. Roach P, Trautmann M, Arora V, Sun B, Anderson JH Jr. Improved postprandial blood glucose control and reduced nocturnal hypoglycemia during treatment with two novel insulin lispro-protamine formulations, insulin lispro mix25 and insulin lispro mix50. Mix50 Study Group. Clin Ther. 1999;21(3):523-534. 19. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117-1124. 40. 20. Zhao G, Etherton TD, Martin KR, West SG, Gillies PJ, Kris-Etherton PM. Dietary alpha-linolenic acid reduces inflammatory and lipid cardiovascular risk factors in hypercholesterolemic men and women. J Nutr. 2004;134(11):2991-2997. Solomon TP, Haus JM, Kelly KR, et al. A low-glycemic index diet combined with exercise reduces insulin resistance, postprandial hyperinsulinemia, and glucose-dependent insulinotropic polypeptide responses in obese, prediabetic humans. Am J Clin Nutr. 2010;92(6): 1359-1368. 41. Fraser A, Abel R, Lawlor DA, Fraser D, Elhayany A. A modified Mediterranean diet is associated with the greatest reduction in alanine aminotransferase levels in obese type 2 diabetes patients: Results of a quasi-randomised controlled trial. Diabetologia. 2008;51(9):16161622. 42. Sathiaraj E, Chutke M, Reddy MY, et al. A case-control study on nutritional risk factors in non-alcoholic fatty liver disease in Indian population. Eur J Clin Nutr. 2011;65(4):533-537. 43. Vilar L, Oliveira CP, Faintuch J, et al. High-fat diet: A trigger of nonalcoholic steatohepatitis? Preliminary findings in obese subjects. Nutrition. 2008;24(11-12):1097-1102. 44. Panagiotakos DB, Polychronopoulos E. The role of Mediterranean diet in the epidemiology of metabolic syndrome; converting epidemiology to clinical practice. Lipids Health Dis. 2005;4:7. 45. Kastorini CM, Milionis HJ, Esposito K, Giugliano D, Goudevenos JA, Panagiotakos DB. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol. 2011;57(11):1299-1313. 46. Gillingham LG, Harris-Janz S, Jones PJ. Dietary monounsaturated Fatty acids are protective against metabolic syndrome and cardiovascular disease risk factors. Lipids. 2011;46(3):209-228. 21. Stern L, Iqbal N, Seshadri P, et al. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: Oneyear follow-up of a randomized trial. Ann Intern Med. 2004;140(10): 778-785. 22. York LW, Puthalapattu S, Wu GY. Nonalcoholic fatty liver disease and low-carbohydrate diets. Annu Rev Nutr. 2009;29:365-379. 23. Garg A, Bantle JP, Henry RR, et al. Effects of varying carbohydrate content of diet in patients with non-insulin-dependent diabetes mellitus. JAMA. 1994;271(18):1421-1428. 24. McLaughlin T, Abbasi F, Lamendola C, Yeni-Komshian H, Reaven G. Carbohydrate-induced hypertriglyceridemia: an insight into the link between plasma insulin and triglyceride concentrations. J Clin Endocrinol Metab. 2000;85(9):3085-3088. 25. Hudgins LC, Hellerstein M, Seidman C, Neese R, Diakun J, Hirsch J. Human fatty acid synthesis is stimulated by a eucaloric low fat, high carbohydrate diet. J Clin Invest. 1996;97(9):2081-2091. 26. Kang H, Greenson JK, Omo JT, et al. Metabolic syndrome is associated with greater histologic severity, higher carbohydrate, and lower fat March 2012 Volume 112 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 407 RESEARCH 68. Ahmed FE. Effect of diet on progression of chronic renal disease. J Am Diet Assoc. 1991;91(10):1266-1270. 69. Meyer TW, Anderson S, Brenner BM. Dietary protein intake and progressive glomerular sclerosis: The role of capillary hypertension and hyperperfusion in the progression of renal disease. Ann Intern Med. 1983;98(5 pt 2):832-838. Lefevre M, Champagne CM, Tulley RT, Rood JC, Most MM. Individual variability in cardiovascular disease risk factor responses to low-fat and low-saturated-fat diets in men: Body mass index, adiposity, and insulin resistance predict changes in LDL cholesterol. Am J Clin Nutr. 2005;82(5):957-963. 70. Hill JO, Thompson H, Wyatt H. Weight maintenance: What’s missing? J Am Diet Assoc. 2005;105(5 suppl 1):S63-66. 71. Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare’s search for effective obesity treatments: Diets are not the answer. Am Psychol. 2007;62(3):220-233. 50. Wang D, Wei Y, Pagliassotti MJ. Saturated fatty acids promote endoplasmic reticulum stress and liver injury in rats with hepatic steatosis. Endocrinology. 2006;147(2):943-951. 72. 51. van den Berg SA, Guigas B, Bijland S, et al. High levels of dietary stearate promote adiposity and deteriorate hepatic insulin sensitivity. Nutr Metab (Lond). 2010;7:24. Phelan S, Wing RR, Loria CM, Kim Y, Lewis CE. Prevalence and predictors of weight-loss maintenance in a biracial cohort: Results from the coronary artery risk development in young adults study. Am J Prev Med. 2010;39(6):546-554. 73. Tetri LH, Basaranoglu M, Brunt EM, Yerian LM, Neuschwander-Tetri BA. Severe NAFLD with hepatic necroinflammatory changes in mice fed trans fats and a high-fructose corn syrup equivalent. Am J Physiol Gastrointest Liver Physiol. 2008;295(5):G987-G995. Hindle L, Carpenter C. An exploration of the experiences and perceptions of people who have maintained weight loss. J Hum Nutr Diet. 2011; 24(4):342-350. 74. Pillai AA, Rinella ME. Non-alcoholic fatty liver disease: Is bariatric surgery the answer? Clin Liver Dis. 2009;13(4):689-710. 75. Mummadi RR, Kasturi KS, Chennareddygari S, Sood GK. Effect of bariatric surgery on nonalcoholic fatty liver disease: Systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2008;6(12): 1396-1402. 76. Hamdy O, Zwiefelhofer D. Weight management using a meal replacement strategy in type 2 diabetes. Curr Diab Rep. 2010;10(2): 159-164. 77. Centis E, Marzocchi R, Di Domizio S, Ciaravella MF, Marchesini G. The effect of lifestyle changes in non-alcoholic fatty liver disease. Dig Dis. 2010;28(1):267-273. 78. Moscatiello S, Di Luzio R, Bugianesi E, et al. Cognitive-behavioral treatment of nonalcoholic fatty liver disease: A propensity scoreadjusted observational study. Obesity (Silver Spring). 2011;19(4): 763-770. 79. Greaves CJ, Sheppard KE, Abraham C, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health. 2011;11(1):119. 80. Boule NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA. 2001;286(10): 1218-1227. 81. Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, et al. Role of leisuretime physical activity in nonalcoholic fatty liver disease: A population-based study. Hepatology. 2008;48(6):1791-1798. 82. St George A, Bauman A, Johnston A, Farrell G, Chey T, George J. Independent effects of physical activity in patients with nonalcoholic fatty liver disease. Hepatology. 2009;50(1):68-76. 83. Kistler KD, Brunt EM, Clark JM, Diehl AM, Sallis JF, Schwimmer JB. Physical activity recommendations, exercise intensity, and histological severity of nonalcoholic Fatty liver disease. Am J Gastroenterol. 2011;106(3):460-468. 84. Devries MC, Samjoo IA, Hamadeh MJ, Tarnopolsky MA. Effect of endurance exercise on hepatic lipid content, enzymes, and adiposity in men and women. Obesity (Silver Spring). 2008;16(10):2281-2288. 85. Bassuk SS, Manson JE. Epidemiological evidence for the role of physical activity in reducing risk of type 2 diabetes and cardiovascular disease. J Appl Physiol. 2005;99(3):1193-1204. 86. Lavine JE. Vitamin E treatment of nonalcoholic steatohepatitis in children: A pilot study. J Pediatr. 2000;136(6):734-738. 87. Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med. 2010; 362(18):1675-1685. 88. Arendt BM, Allard JP. Effect of atorvastatin, vitamin E and C on nonalcoholic fatty liver disease: Is the combination required? Am J Gastroenterol. 2011;106(1):78-80. 89. Sanyal AJ, Mofrad PS, Contos MJ, et al. A pilot study of vitamin E versus vitamin E and pioglitazone for the treatment of nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol. 2004;2(12):1107-1115. 90. Kugelmas M, Hill DB, Vivian B, Marsano L, McClain CJ. Cytokines and NASH: A pilot study of the effects of lifestyle modification and vitamin E. Hepatology. 2003;38(2):413-419. 47. Vallim T, Salter AM. Regulation of hepatic gene expression by saturated fatty acids. Prostaglandins Leukot Essent Fatty Acids. 2010;82(46):211-218. 48. Musso G, Gambino R, De Michieli F, et al. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology. 2003;37(4):909-916. 49. 52. 53. Martinez-Gonzalez MA, Sanchez-Villegas A. The emerging role of Mediterranean diets in cardiovascular epidemiology: monounsaturated fats, olive oil, red wine or the whole pattern? Eur J Epidemiol. 2004;19(1):9-13. 54. Alonso A, Ruiz-Gutierrez V, Martinez-Gonzalez MA. Monounsaturated fatty acids, olive oil and blood pressure: Epidemiological, clinical and experimental evidence. Public Health Nutr. 2006;9(2):251-257. 55. Assy N, Nassar F, Nasser G, Grosovski M. Olive oil consumption and non-alcoholic fatty liver disease. World J Gastroenterol. 2009;15(15): 1809-1815. 56. Clarke SD, Jump DB. Polyunsaturated fatty acid regulation of hepatic gene transcription. Lipids. 1996;31(suppl):S7-S11. 57. Kim HJ, Takahashi M, Ezaki O. Fish oil feeding decreases mature sterol regulatory element-binding protein 1 (SREBP-1) by downregulation of SREBP-1c mRNA in mouse liver. A possible mechanism for down-regulation of lipogenic enzyme mRNAs. J Biol Chem. 1999; 274(36):25892-25898. 58. Benatti P, Peluso G, Nicolai R, Calvani M. Polyunsaturated fatty acids: Biochemical, nutritional and epigenetic properties. J Am Coll Nutr. Aug 2004;23(4):281-302. 59. Capanni M, Calella F, Biagini MR, et al. Prolonged n-3 polyunsaturated fatty acid supplementation ameliorates hepatic steatosis in patients with non-alcoholic fatty liver disease: A pilot study. Aliment Pharmacol Ther. 2006;23(8):1143-1151. 60. Spadaro L, Magliocco O, Spampinato D, et al. Effects of n-3 polyunsaturated fatty acids in subjects with nonalcoholic fatty liver disease. Dig Liver Dis. 2008;40(3):194-199. 61. Tanaka N, Sano K, Horiuchi A, Tanaka E, Kiyosawa K, Aoyama T. Highly purified eicosapentaenoic acid treatment improves nonalcoholic steatohepatitis. J Clin Gastroenterol. 2008;42(4):413-418. 62. Zuliani G, Galvani M, Leitersdorf E, Volpato S, Cavalieri M, Fellin R. The role of polyunsaturated fatty acids (PUFA) in the treatment of dyslipidemias. Curr Pharm Des. 2009;15(36):4087-4093. 63. Ebrahimi M, Ghayour-Mobarhan M, Rezaiean S, et al. Omega-3 fatty acid supplements improve the cardiovascular risk profile of subjects with metabolic syndrome, including markers of inflammation and auto-immunity. Acta Cardiol. 2009;64(3):321-327. 64. Tapsell LC, Gillen LJ, Patch CS, et al. Including walnuts in a low-fat/ modified-fat diet improves HDL cholesterol-to-total cholesterol ratios in patients with type 2 diabetes. Diabetes Care. 2004;27(12): 2777-2783. 65. Araya J, Rodrigo R, Videla LA, et al. Increase in long-chain polyunsaturated fatty acid n-6/n-3 ratio in relation to hepatic steatosis in patients with non-alcoholic fatty liver disease. Clin Sci (Lond). 2004; 106(6):635-643. 66. 67. 408 Tovar AR, Torre-Villalvazo I, Ochoa M, et al. Soy protein reduces hepatic lipotoxicity in hyperinsulinemic obese Zucker fa/fa rats. J Lipid Res. 2005;46(9):1823-1832. Mikkelsen PB, Toubro S, Astrup A. Effect of fat-reduced diets on 24-h energy expenditure: Comparisons between animal protein, vegetable protein, and carbohydrate. Am J Clin Nutr. 2000;72(5): 1135-1141. JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS March 2012 Volume 112 Number 3 RESEARCH 91. Foster T, Budoff MJ, Saab S, Ahmadi N, Gordon C, Guerci AD. Atorvastatin and antioxidants for the treatment of nonalcoholic fatty liver disease: The St Francis Heart Study randomized clinical trial. Am J Gastroenterol. 2011;106(1):71-77. 92. Harrison SA, Torgerson S, Hayashi P, Ward J, Schenker S. Vitamin E and vitamin C treatment improves fibrosis in patients with nonalcoholic steatohepatitis. Am J Gastroenterol. 2003;98(11):2485-2490. 93. Miller ER, 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):3746. 94. Abdelmalek MF, Angulo P, Jorgensen RA, Sylvestre PB, Lindor KD. Betaine, a promising new agent for patients with nonalcoholic steatohepatitis: Results of a pilot study. Am J Gastroenterol. 2001;96(9): 2711-2717. 95. Kathirvel E, Morgan K, Nandgiri G, et al. Betaine improves nonalcoholic fatty liver and associated hepatic insulin resistance: A potential mechanism for hepatoprotection by betaine. Am J Physiol Gastrointest Liver Physiol. 2010;299(5):G1068-G1077. 96. Wang Z, Yao T, Pini M, Zhou Z, Fantuzzi G, Song Z. Betaine improved adipose tissue function in mice fed a high-fat diet: A mechanism for hepatoprotective effect of betaine in nonalcoholic fatty liver disease. Am J Physiol Gastrointest Liver Physiol. 2010;298(5):G634G642. 100. Loguercio C, Federico A, Tuccillo C, et al. Beneficial effects of a probiotic VSL#3 on parameters of liver dysfunction in chronic liver diseases. J Clin Gastroenterol. 2005;39(6):540-543. 101. Sahebkar A. Potential efficacy of ginger as a natural supplement for nonalcoholic fatty liver disease. World J Gastroenterol. 2011;17(2): 271-272. 102. Mohamed Salih S, Nallasamy P, Muniyandi P, Periyasami V, Carani Venkatraman A. Genistein improves liver function and attenuates non-alcoholic fatty liver disease in a rat model of insulin resistance. J Diabetes. 2009;1(4):278-287. 103. Yalniz M, Bahcecioglu IH, Kuzu N, et al. Preventive role of genistein in an experimental non-alcoholic steatohepatitis model. J Gastroenterol Hepatol. 2007;22(11):2009-2014. 104. Kim MH, Kang KS, Lee YS. The inhibitory effect of genistein on hepatic steatosis is linked to visceral adipocyte metabolism in mice with diet-induced non-alcoholic fatty liver disease. Br J Nutr. 2010; 104(9):1333-1342. 105. Casiglia E, Spolaore P, Ginocchio G, Ambrosio GB. Unexpected effects of coffee consumption on liver enzymes. Eur J Epidemiol. 1993;9(3): 293-297. 106. Sharp DS, Benowitz NL. Re: “Alcohol, smoking, coffee, and cirrhosis” and “coffee and serum gamma-glutamyltransferase: A study of selfdefense officials in Japan.” Am J Epidemiol. 1995;141(5):480-482. 97. Abdelmalek MF, Sanderson SO, Angulo P, et al. Betaine for nonalcoholic fatty liver disease: Results of a randomized placebo-controlled trial. Hepatology. 2009;50(6):1818-1826. 107. Modi AA, Feld JJ, Park Y, et al. Increased caffeine consumption is associated with reduced hepatic fibrosis. Hepatology. 2010;51(1): 201-209. 98. Abu-Shanab A, Quigley EM. The role of the gut microbiota in nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2010; 7(12):691-701. 108. Costentin CE, Roudot-Thoraval F, Zafrani ES, et al. Association of caffeine intake and histological features of chronic hepatitis C. J Hepatol. 2011;54(6):1123-1129. 99. Loguercio C, De Simone T, Federico A, et al. Gut-liver axis: A new point of attack to treat chronic liver damage? Am J Gastroenterol. 2002;97(8):2144-2146. 109. Ruhl CE, Everhart JE. Coffee and tea consumption are associated with a lower incidence of chronic liver disease in the United States. Gastroenterology. 2005;129(6):1928-1936. AUTHOR INFORMATION E. M. McCarthy is a registered dietitian, Northwestern Faculty Foundation, Chicago, IL. M. E. Rinella is an associate professor of medicine, Department of Gastroenterology and Hepatology, Northwestern University Feinberg School of Medicine, Northwestern Memorial Hospital, Chicago, IL. Address correspondence to: Mary E. Rinella, MD, Department of Gastroenterology and Hepatology, Northwestern University Feinberg School of Medicine, Northwestern Memorial Hospital, 303 E Chicago Ave, Searle 10-563, Chicago, IL 60611. E-mail: [email protected] STATEMENT OF POTENTIAL CONFLICT OF INTEREST: No potential conflict of interest was reported by the authors. March 2012 Volume 112 Number 3 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 409