Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Scaling and root planing wikipedia , lookup
Dentistry throughout the world wikipedia , lookup
Forensic dentistry wikipedia , lookup
Endodontic therapy wikipedia , lookup
Dental hygienist wikipedia , lookup
Focal infection theory wikipedia , lookup
Impacted wisdom teeth wikipedia , lookup
Dental degree wikipedia , lookup
Periodontal disease wikipedia , lookup
Special needs dentistry wikipedia , lookup
Crown (dentistry) wikipedia , lookup
Tooth whitening wikipedia , lookup
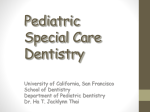
Case Report Amelogenesis Imperfecta: A Series of Case Report Nuzula Begum1, Gowri P Bhandarkar2, Raghavendra Kini3, Vathsala Naik4, K Rashmi1, Lizzy Carol D Souza1 Post Graduate Student, Department of Oral Medicine and Radiology, A.J. Institute of Dental Sciences, Kuntikana, Mangalore, Karnataka, India, Reader and Guide, Department of Oral Medicine and Radiology, A.J. Institute of Dental Sciences, Kuntikana, Mangalore, Karnataka, India, 3 Professor and Vice Principal, Department of Oral Medicine and Radiology, A.J. Institute of Dental Sciences, Kuntikana, Mangalore, Karnataka, India, 4Professor and Head, Department of Oral Medicine and Radiology, A.J. Institute of Dental Sciences, Kuntikana, Mangalore, Karnataka, India 1 2 ABSTRACT Amelogenesis imperfecta (AI) incorporates an assemblage of hereditary diseases that involve the defective formation or calcification of enamel. The occurrence of enamel defects without any sign of generalized or systemic defects is the pathognomonic feature of AI. It involves both primary and permanent dentitions. AI had been found to be associated with non-enamel anomalies such as delayed eruption, crown resorption, congenitally missing teeth, pulpal calcifications, dental follicular hamartomas, and gingival hyperplasia. We present here two case reports of AI (hypo maturative and hypoplastic) that we diagnosed on the basis of clinical and radiographic features along with the complete review. Keywords: Amelogenesis imperfecta, Discoloration, Hypoplastic, Hypomaturative, Prosthetic rehabilitation Corresponding Author: Dr. Nuzula Begum, Department of Oral Medicine and Radiology, A.J. Institute of Dental Sciences, Kuntikana, Mangalore, Karnataka, India. Phone: +91-9916517440. E-mail: [email protected] INTRODUCTION Amelogenesis imperfecta (AI) is a multifarious assemblage of inherited conditions that disturbs the developing enamel structure and presents independently of any related systemic disorder. 1 Improper differentiation of ameloblasts in AI causes poor development or complete absence of enamel of the teeth. Both the primary and permanent dentition may be affected by this enamel anomaly. AI encompasses a group of hereditary diseases that involve the defective formation or calcification of enamel. The occurrence of enamel defects without any sign of generalized or systemic defects is the pathognomic feature of AI. Non-enamel anomalies such as delayed eruption, crown resorption, congenitally missing teeth, pulpal calcifications, dental follicular hamartomas, and gingival hyperplasia had been found to be associated with AI. Exclusion of extrinsic environmental or other factors, the establishment of a likely inheritance pattern, and recognition of phenotype and correlation with the dates of tooth formation to exclude a chronological developmental disturbance involves diagnosis. 17 The enamel may be hypoplastic, hypo mineralized or both and teeth affected may be discolored, sensitive or prone to disintegration either post-eruption or preeruption.2 It may be associated with morphologic or biochemical changes elsewhere in the body.3 Hypoplastic AI represents 60-73% of all cases; hypomaturation AI represents 20-40%, and hypo-calcification AI represents 7%.4 The most widely accepted classification is that proposed by Witkop and Sank in 1976. Aldred and Crawford also proposed a new classification. Witkop and Rao, (1971) classified AI broadly based on phenotype and style of inheritance5 into three categories: Hypoplastic variety, hypocalcified variety, and hypo maturation variety. Aldred and Crawford in 19956 classified based on a molecular defect, biochemical result, mode of inheritance and phenotype. Dental enamel, a highly mineralized tissue has over 95% of its volume being occupied by unusually large, highly organized, hydroxyapatite crystals.2 The formation of enamel has been highly organized, and unusual structure is thought to be rigorously controlled in ameloblasts. This has been through the interaction of a number of organic matrix molecules.7 International Journal of Advanced Health Sciences • Vol 2 Issue 1 • May 2015 Begum, et al. Amelogenesis Imperfecta: A Series of Case Report AI affects both dentitions (deciduous and permanent). Teeth exhibit yellow to dark brown discoloration. The consistency varies from cheesy to hard. The teeth exhibit pits and grooves and in some cases enamel may be completely absent. In Type I/hypoplastic AI, enamel is well-mineralized but is reduced in quantity. There is a deficiency of enamel matrix. In type II/hypomaturation AI, enamel is of normal thickness but has a mottled appearance. In Type III/hypocalcified AI, enamel is of a normal thickness that often chips and abrades easily. AI may be allied with some other dental and skeletal developmental defects or abnormalities.8 We present here two case reports of AI (hypo maturative and hypoplastic) along with a complete review that we diagnosed on the basis of clinical and radiographic features. CASE REPORTS Case 1 (Figure 2). OPG and IOPA revealed a generalized loss of enamel thickness and reduced occlusal height with breakage of interproximal contact. Radio density of enamel was same as dentin with normal pulp chamber and root morphology. Based on radiographic examination AI (hypo maturative type) was given as the diagnosis. As the patient was 13-year-old; still canines were not erupted and distal expansion of first molar was remaining, so definitive treatment was not planned. Current treatment was done mainly to improve patient’s aesthetics’ and to prevent further deterioration of teeth. A conservative approach such as root canal treatment in relation to 16, 26 was advised followed by bite registration and full mouth prosthetic rehabilitation (Figure 3). Case 2 A 16-year-old female patient reported with a chief complaint of yellowish discoloration of teeth since 5 years, associated with sensitivity while having hot and cold food. The patient also gave a history of the discolored primary dentition. Family history was noncontributory. Past medical history revealed no associated A 13-year-old female patient reported to the department with a chief complaint of generalized discolored teeth since childhood. Patient gave a positive history of discolored deciduous teeth. Past medical, dental, and personal history was non-contributory. Family history revealed that the mother had a similar type of discoloration and attrition and underwent treatment for the same. On intraoral examination, generalized yellowish discoloration with attrition was present on the occlusal surface of the teeth with breakage of the interdental contact region. The thickness of enamel was reduced with localized chipping of enamel surface in anterior teeth region. The labial and buccal surface of the teeth was soft, cheesy, and generalized diffuse pitting was present. Flattening of incisal and occlusal table with deformed occlusal morphology was noted. Eruption pattern seemed to be within normal limits except for the canines in the upper quadrant that had not been erupted. Bilateral anterior and posterior cross bite was noted (Figure 1). Dental caries in relation to 16, 26 which had been pulpally involved. Figure 1: Generalized yellowish brown discoloration with chipped out enamel surface Hence, considering the history and after clinical examination AI (hypo maturative type) was conferred as the provisional diagnosis. Dental fluorosis, dentinogenesis imperfecta, dentin dysplasia were considered under differential diagnosis. Patient had been advised for full mouth intraoral periapical (IOPA) and orthopantomogram (OPG) Figure 2: Intraoral periapical and orthopantomogram reveals normal pulp chamber and root morphology. Radio density of enamel is same as dentin International Journal of Advanced Health Sciences • Vol 2 Issue 1 • May 2015 18 Amelogenesis Imperfecta: A Series of Case Report systemic abnormalities. Intraoral examination revealed, yellowish brown discoloration of permanent teeth with generalized attrition leading to a reduced occlusal height of teeth. Loss of interproximal contacts with posterior open bite was present (Figure 4). Radiographic investigations such as IOPA and OPG revealed a relatively thin layer of enamel with normal pulp chamber and root morphology. Radio-density of enamel was same as dentin. Radiolucency had been seen on the coronal aspect of 17, 27, 36, and 46 involving dentin suggestive of dentinal caries. Flattening of the occlusal table with the loss of interproximal contacts was present in the anterior regions (Figures 5 and 6). As per the patient’s history and clinical findings, a provisional diagnosis was given as Type I AI (hypoplastic variety). Differential diagnosis of severe dentinal fluorosis was considered. Patient had been referred for restoration followed by complete rehabilitation with fixation of the full ceramic prosthesis (Figure 7). Begum, et al. autosomal recessive, sex-linked, and sporadic inheritance patterns, as well as sporadic cases.2 Epidemiology AI had been first reported in 1890. It was considered a clinical entity distinct from dentinogenesis imperfecta only in 1938. Its prevalence varies widely between studies, from 1 in 718 to 1 in 14,000. Classification There are numerous classification systems and the most widely accepted is that proposed by Witkop and Sank in 1976, which considers the inheritance pattern of the disorder, as well as its specific clinical characteristics. Aldred and Crawford proposed a new classification that not only evaluates the phenotype but also the molecular disorder, the biochemical composition of the enamel, and the mode of inheritance of the defect. Witkop and Rao, (1971) classified based on phenotype and style of inheritance.5 DISCUSSION AI represents a group of conditions and is genomic in origin. AI affects the structure and clinical appearance of the enamel of all or nearly all the teeth in a more or less equal manner. AI is a developmental condition of the dental enamel that is characterized by hypoplasia or hypomineralization. AI shows autosomal dominant, Figure 5: Full mouth intraoral periapical ??? Figure 3: Prosthetic rehabilitation Figure 6: Orthopantomogram Figure 4: Yellowish brown discoloration with generalized attrition 19 Figure 7: Full mouth rehabilitation (postoperative treatment photograph) International Journal of Advanced Health Sciences • Vol 2 Issue 1 • May 2015 Begum, et al. Amelogenesis Imperfecta: A Series of Case Report Three broad categories: Hypoplastic, hypocalcified, hypomaturation. a. Hypoplastic • Autosomal dominant hypoplastichypomaturation with taurodontism (subdivided into a and b according to author) • Autosomal dominant smooth hypoplastic with eruption defect and resorption of teeth • Autosomal dominant rough hypoplastic • Autosomal dominant pitted hypoplastic • Autosomal dominant local hypoplastic • X-linked dominant rough hypoplastic b. Hypocalcified • Autosomal dominant hypocalcified c. Hypomaturation • X-linked recessive hypo maturation • Autosomal recessive pigmented hypo maturation • Autosomal dominant snow-capped teeth • White hypomature spots? Aldred and Crawford, 1995.6 Classification based on: (a) Molecular defect (when known) (b) Biochemical result (when known) (c) Mode of inheritance (d) Phenotype Etiology Dental enamel, a highly mineralized tissue has over 95% of its volume being occupied by unusually large, highly organized, hydroxyapatite crystals.2 The formation of enamel has been highly organized, and unusual structure is thought to be rigorously controlled in ameloblasts. This has been through the interaction of a number of organic matrix molecules. They include enamelin (ENAM; 4q21), amelogenin (AMELX; Xp22.3-p22.1), ameloblastin (AMBN; 4q21), tuftelin (TUFT1; 1q21), amelotin (AMELOTIN; 4q13), dentine sialophosphoprotein (DSPP; 4q21.3), kallikrein 4 (KLK4; 19q13.3–q13.4), matrix metalloproteinase 20 (MMP20; 11q22.3–q23).7 Clinical Features Affects both dentitions (deciduous and permanent). Teeth exhibit yellow to dark brown discoloration, the consistency varying from cheesy to hard. The teeth exhibit pits and grooves and in some cases enamel may be completely absent. Type I/hypoplastic AI Enamel is well-mineralized but is reduced in quantity. Clinically grooves and pits will be realized on the surface of the fine enamel. The rough pattern of hypoplastic type exhibits thin, hard, and rough surfaced enamel. The tooth is tapered toward the incisal/occlusal face and has open contact points. There is a deficiency of enamel matrix. In about 50% of cases, the anterior open bite is noticed as a result of a decreased crown height. Type II/hypomaturation AI Enamel is of normal thickness but has a mottled appearance. It is slightly softer than normal enamel, is easily penetrated by the point of a probe and chips away from the crown. Enamel appears clear to cloudy, mottled yellow to brown. Enamel has random alternating vertical bands of either opaque white or opaque yellow enamel with bands of translucent normal enamel.8 AI may be allied with some other dental and skeletal developmental defects or abnormalities. They are crown and root resorption, attrition, taurodontism, delayed eruption, and tooth impaction, dens in dente, pulp stones, anterior open bite, and agenesis of teeth.8 AI is sometimes associated with syndromes such as AI with taurodontism, tricho-dento osseous syndrome, AI with nephrocalcinosis, and cone-rod dystrophy with AI.9 Type III/hypocalcified AI This variety of AI appears as opaque white to yellow-brown discoloration with soft and rough enamel surface. Dentin sensitivity and the open bite are common, as well as heavy calculus formation. This type of AI has normal thickness with enamel that often chips and abrades easily. Enamel has a contrast similar to or less than that of dentin. Unerupted crowns have normal morphology. Differential Diagnosis Extrinsic disorders of tooth formation, chronological disorders of tooth formation, and localized disorders of tooth formation should be considered in the differential diagnosis. The differential diagnosis considered most probable is dental fluorosis. The variability of this condition, from mild white “flecking” of the enamel to profoundly dense white coloration with random, disfiguring areas of staining and hypoplasia, entails careful interrogation to distinguish from AI. Fluorosis may present with areas of horizontal white banding corresponding to periods of more intense fluoride intake. The premolars or second molars are normally spared (chronological distribution). The history often reveals excessive fluoride intake in terms of a habit, such as eating toothpaste in childhood or related to a local water supply.2 Treatment The treatment of these patients has been usually done in two phases, temporary phase followed by transitory phase.10 The complexity of the condition requires an interdisciplinary approach for optimal International Journal of Advanced Health Sciences • Vol 2 Issue 1 • May 2015 20 Amelogenesis Imperfecta: A Series of Case Report treatment outcomes.11 Adhesive restorative techniques, over-dentures, fixed partial dentures, full porcelain crowns, porcelain-fused-to-metal crowns, and inlay/onlay restorations constitute the contemporary treatment modalities. The treatment approach should ideally be developed keeping in mind the specific AI type and underlying defect.12 CONCLUSION AI is a serious problem resulting in reduced oral health-related quality of life. People with AI need extensive treatment. While planning the treatment, the age and the socioeconomic status of the patient, type, and the severity of the disorder should be taken into consideration. Radiology plays a very important role in an assessment of enamel density and to develop a more appropriate treatment plan in patients with enamel defect. The dentist has to balance the decision for early intervention and longtime survival of the restorations to prevent later problems. REFERENCES 1. 2. 3. 21 Neville BW, Damm DD, Allen CM, Bouquot JE. Abnormalities of teeth. In: Oral and Maxillofacial Pathology. 2nd ed., Ch. 2. Philadelphia: Saunders, an Imprint of Elseiver; 2005. p. 89. Crawford PJ, Aldred M, Bloch-Zupan A. Amelogenesis imperfecta. Orphanet J Rare Dis 2007;2:17. Aldred MJ, Savarirayan R, Crawford PJ. Amelogenesis imperfecta: Begum, et al. A classification and catalogue for the 21st century. Oral Dis 2003;9:19-23. 4. Rajendran R. Developmental disturbances of oral and para oral structures. In: Rajendran R, Sivaparthasundaram B, editors. Shafer’s Text book of Oral Pathology. 5th ed., Ch. 1. Amsterdam: Elsevier; 2007. p. 67. 5. Witkop CJ Jr, Rao S. Inherited defects in tooth structure. The clinical delineation of birth defects. Part XI orofacial structures. In: Bergsma E, editor. Birth Defects Original Article Series. Vol. 7. Baltimore: Williams & Wilkins; 1971. p. 153-84. 6. Aldred MJ, Crawford PJ. Amelogenesis imperfecta – Towards a new classification. Oral Dis 1995;1:2-5. 7. Iwasaki K, Bajenova E, Somogyi-Ganss E, Miller M, Nguyen V, Nourkeyhani H, et al. Amelotin – A novel secreted, ameloblastspecific protein. J Dent Res 2005;84:1127-32. 8. Canger EM, Celenk P, Yenísey M, Odyakmaz SZ. Amelogenesis imperfecta, hypoplastic type associated with some dental abnormalities: A case report. Braz Dent J 2010;21:170-4. 9. Chanmougananda SC, Ashokan KA, Ashokan SC, Bojan AB, Ganesh RM. Literature review of amelogenesis imperfecta with case report. J Indian Acad Oral Med Radiol 2012;24:83-7. 10. Bouvier D, Duprez JP, Bois D. Rehabilitation of young patients with amelogenesis imperfecta: A report of two cases. ASDC J Dent Child 1996;63:443-7. 11. Turkistanin JM, Almushayt A, Farsi S. Multidisciplinary treatment approach of a patient with amelogenesis imperfecta: A case report. Open J Stomatol 2013;3:397-01. 12. Kharkwal R. Dental rehabilitation of amelogenesis imperfecta in the mixed dentition. Int J Sci Stud 2014;1:56-9. How to cite this article: Begum N, Bhandarkar GP, Kini R, Naik V, Rashmi K, D Souza LC. Amelogenesis Imperfecta: A Series of Case Report. Int J Adv Health Sci 2015;2(1):17-21. Source of Support: Nil, Conflict of Interest: None declared. International Journal of Advanced Health Sciences • Vol 2 Issue 1 • May 2015