Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
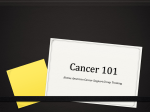
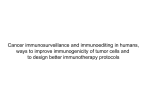
TREIMM 1288 No. of Pages 15 Review Targeted Therapy and Checkpoint Immunotherapy Combinations for the Treatment of Cancer Paul E. Hughes,1 Sean Caenepeel,1 and Lawren C. Wu2,* Many advances in the treatment of cancer have been driven by the development of targeted therapies that inhibit oncogenic signaling pathways and tumorassociated angiogenesis, as well as by the recent development of therapies that activate a patient's immune system to unleash antitumor immunity. Some targeted therapies can have effects on host immune responses, in addition to their effects on tumor biology. These immune-modulating effects, such as increasing tumor antigenicity or promoting intratumoral T cell infiltration, provide a rationale for combining these targeted therapies with immunotherapies. Here, we discuss the immune-modulating effects of targeted therapies against the MAPK and VEGF signaling pathways, and how they may synergize with immunomodulatory antibodies that target PD1/PDL1 and CTLA4. We critically examine the rationale in support of these combinations in light of the current understanding of the underlying mechanisms of action of these therapies. We also discuss the available preclinical and clinical data for these combination approaches and their implications regarding mechanisms of action. Insights from these studies provide a framework for considering additional combinations of targeted therapies and immunotherapies for the treatment of cancer. Introduction The treatment of cancer has advanced significantly over the past 15 years, driven by many scientific insights including those that have led to the approval of targeted therapies that inhibit tumor angiogenesis and intrinsic drivers of cancer cell growth, as well as immunomodulatory therapies that enhance host antitumor immunity (Table 1). Targeted therapies can elicit dramatic clinical responses in several tumor types, but these responses are transient, with tumor escape and clinical relapse usually occurring within months after an initial response. By contrast, cancer immunotherapies can elicit durable responses in subsets of treated patients across multiple tumor types, and this striking clinical activity has led to a surge of research and clinical development in the field of cancer immunotherapy. The key steps involved in a productive antitumor immune response have been outlined by Chen and Mellman and termed the ‘cancer-immunity cycle’ (Figure 1) [1]. Briefly, cancer-specific antigens created during the process of oncogenesis are captured and processed by dendritic cells in the tumor microenvironment. Upon additional proinflammatory signals, these dendritic cells are activated and travel to tumor-draining lymph nodes, where they prime the activation and differentiation of naïve T cells to become effector T cells that are capable of killing cancer cells. Activated effector T cells traffic from the lymph nodes through blood vessels to the Trends in Immunology, Month Year, Vol. xx, No. yy Trends Targeted therapies inhibit tumor-intrinsic drivers of growth and can elicit significant but transient clinical responses. Immunotherapies enhance host antitumor immunity and can elicit durable responses in subsets of patients across multiple tumor types. Checkpoint inhibitors are immunotherapies that relieve suppressive signals acting on host T cells to unleash antitumor T cell activity. In some cases, targeted therapies can enhance aspects of cancer immunity, such as tumor antigenicity, T cell trafficking, or T cell infiltration into tumors, which provides a rationale for combining them with checkpoint inhibitors or other cancer immunotherapies that may lead to synergistic efficacy. Considerations for the clinical development of combinations of targeted therapies and immunotherapies include optimizing dosing regimens, minimizing treatment related toxicities, and selecting appropriate biomarkers and endpoints to assess efficacy. 1 Department of Oncology, Amgen, Inc, Thousand Oaks, CA, USA 2 Department of Oncology, Amgen, Inc, South San Francisco, CA, USA *Correspondence: [email protected] (L.C. Wu). http://dx.doi.org/10.1016/j.it.2016.04.010 © 2016 Elsevier Ltd. All rights reserved. 1 TREIMM 1288 No. of Pages 15 Table 1. Approved Targeted Therapies and Immunotherapy Checkpoint Inhibitors for the Treatment of Solid Tumors[1_TD$IF]. Drug Target Targeted Therapy/ Immunotherapy Modality Indication(s) Vemurafenib BRAF Targeted therapy Small molecule Melanoma Dabrafenib BRAF Targeted therapy Small molecule Melanoma Trametinib MEK Targeted therapy Small molecule Melanoma Cobimetinib MEK Targeted therapy Small molecule Melanoma Ipilimumab CTLA-4 Immunotherapy Antibody Melanoma Nivolumab PD-1 Immunotherapy Antibody Melanoma, renal cell carcinoma, lung cancer Pembrolizumab PD-1 Immunotherapy Antibody Melanoma, lung cancer Bevacizumab VEGF-A Targeted therapy Antibody Renal cell carcinoma, brain cancer, cervical cancer, colorectal cancer, lung cancer, ovarian epithelial, fallopian tube, peritoneal cancers Axitinib Multikinase inhibitor (VEGFR, PDGFR, KIT, ABL) Targeted therapy Small molecule Renal cell carcinoma Pazopanib Multikinase inhibitor (VEGFR, PDGFR, FGFR, KIT, LTK, LCK) Targeted therapy Small molecule Renal cell carcinoma, soft tissue sarcoma Sorafenib Multikinase inhibitor (VEGFR, PDGFR, KIT, RET, RAF) Targeted therapy Small molecule Renal cell carcinoma, thyroid cancer, liver cancer Sunitinib Multikinase inhibitor (VEGFR, PDGFR, KIT, RET) Targeted therapy Small molecule Renal cell carcinoma, gastrointestinal stromal tumor, pancreatic cancer Temsirolimus mTOR Targeted therapy Small molecule Renal cell carcinoma Everolimus mTOR Targeted therapy Small molecule Renal cell carcinoma, breast cancer, brain cancer, pancreatic cancer, gastrointestinal cancer, lung cancer Ceritinib ALK Targeted therapy Small molecule Lung cancer Alectinib ALK Targeted therapy Small molecule Lung cancer Gefitinib EGFR Targeted therapy Small molecule Lung cancer Afatinib EGFR Targeted therapy Small molecule Lung cancer Osimertinib EGFR Targeted therapy Small molecule Lung cancer Nectumumab EGFR Targeted therapy Antibody Lung cancer Crizotinib Multikinase inhibitor (MET, ALK, ROS) Targeted therapy Small molecule Lung cancer Erlotinib EGFR Targeted therapy Small molecule Lung cancer, pancreatic cancer Ramucirumab VEGFR2 Targeted therapy Antibody Lung cancer, adenocarcinoma of stomach or gastroesophageal junction, colorectal cancer 2 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 Table 1. (continued) Drug Target Targeted Therapy/ Immunotherapy Modality Indication(s) Vismodegib SMO Targeted therapy Small molecule Basal cell carcinoma Sonidegib SMO Targeted therapy Small molecule Basal cell carcinoma Anastrozole Aromatase Targeted therapy Small molecule Breast cancer Exemestane Aromatase Targeted therapy Small molecule Breast cancer Letrozole Aromatase Targeted therapy Small molecule Breast cancer Palbociclib CDK4 CDK6 Targeted therapy Small molecule Breast cancer Lapatinib EGFR HER2 Targeted therapy Small molecule Breast cancer Tamoxifen ER Targeted therapy Small molecule Breast cancer Toremifene ER Targeted therapy Small molecule Breast cancer Fulvestrant ER Targeted therapy Small molecule Breast cancer Pertuzumab HER2 Targeted therapy Antibody Breast cancer Trastuzumab emtasine HER2 Targeted therapy Antibody drug conjugate Breast cancer Trastuzumab HER2 Targeted therapy Antibody Breast cancer and adenocarcinoma of stomach or gastroesophageal junction Panitumumab EGFR Targeted therapy Antibody Colorectal cancer Aflibercept VEGF-A, VEGF-B Targeted therapy Recombinant fusion protein Colorectal cancer Regorafenib Multikinase inhibitor (VEGFR, PDGFR, KIT, RET, RAF) Targeted therapy Small molecule Colorectal cancer, gastrointestinal stromal tumor Cetuximab EGFR Targeted therapy Antibody Colorectal cancer, head and neck cancer Imatinib mesylate Multikinase inhibitor (ABL, KIT, PDGFR,) Targeted therapy Small molecule Dermatofibrosarcoma protuberans, gastrointestinal stromal tumor, systemic mastocytosis Denosumab RAK ligand Targeted therapy Antibody Giant cell tumor of bone Dinutuximab GD2 Targeted therapy Antibody Neuroblastoma Olaparib PARP Targeted therapy Small molecule Ovarian epithelial, fallopian tube, peritoneal cancers Abiraterone acetate Androgen synthase Targeted therapy Small molecule Prostate cancer Enzalutamide AR Targeted therapy Small molecule Prostate cancer Cabozantinib Multikinase inhibitor (MET, VEGFR2, RET, KIT) Targeted therapy Small molecule Thyroid cancer Lenvatinib Multikinase inhibitor (VEGFR, FGFR, PDGFR, KIT, RET) Targeted therapy Small molecule Thyroid cancer Vandetanib Multikinase inhibitor (VEGFR, RET, EGFR) Targeted therapy Small molecule Thyroid cancer Trends in Immunology, Month Year, Vol. xx, No. yy 3 TREIMM 1288 No. of Pages 15 An-PD1 and An-PDL1 MAPK inhibitors T cell acvaon and tumor cell killing MAPK inhibitors Tumor cell death T cell infiltraon Angen acquision by dendric cells MAPK inhibitors VEGF inhibitors VEGF inhibitors T cell trafficking T cell priming An-CTLA4 Figure 1. The Cancer-Immunity Cycle. The generation of anticancer T cell responses is initiated when tumor antigens are captured and processed by dendritic cells in the tumor microenvironment. These dendritic cells are activated and travel to tumor-draining lymph nodes, where they prime naïve T cells to become effector T cells that are capable of killing cancer cells. Activated effector T cells traffic from the lymph nodes to the tumor and infiltrate the tumor bed, where they kill cancer cells and trigger additional antigen release that can induce subsequent rounds of anticancer immunity. T cell checkpoint therapies (green text) enhance either T cell priming (anti-CTLA4) or T cell activation and killing in the tumor (anti-PD1 and antiPDL1). MAPK inhibitors (red text) complement T cell checkpoint therapies by enhancing tumor antigen expression, immunogenic tumor cell death, and T cell infiltration into tumors. VEGF inhibitors (blue text) complement T cell checkpoint therapies by enhancing dendritic cell maturation and activity, as well as T cell infiltration into tumors. Adapted from [1]. tumor and infiltrate into the tumor bed through a multistep process that involves initial adhesive interactions between the T cells and vascular endothelial cells, followed by transendothelial migration into the tumor [2,3]. Once T cells have infiltrated the tumor bed, recognition of specific tumor antigens leads to T cell killing of cancer cells, which can trigger additional antigen release and subsequent induction of additional rounds of the cancer-immunity cycle. A significant number of clinical studies have been planned or are ongoing to combine targeted therapies with immunomodulatory therapies (Table 2). While these studies are supported by a rationale of combining therapies that target nonoverlapping immune and tumor biology mechanisms to enhance antitumor activity, in some cases evidence exists that the targeted therapies can also enhance aspects of the cancer-immunity cycle, which provides an additional rationale for combining them with cancer immunotherapies. In this review, we discuss two examples in which targeted therapies against the MAPK pathway and the VEGF pathway can elicit effects on tumor antigenicity and intratumoral T cell infiltration, in addition to their direct effects on cancer cell growth and tumor angiogenesis. The effects of these targeted therapies on host immune responses, beyond their effects on tumor biology, provide a strong rationale for combining them with immune-modulating T cell checkpoint therapies. T Cell Checkpoint Therapies T cell activation is a multistep process that is triggered by the initial recognition of antigenic peptide-MHC complexes by the T cell receptor, followed by the delivery of secondary costimulatory signals to fully activate the T cell [4,5]. T cell activation can also be inhibited by negative regulatory molecules, also referred to as checkpoint molecules, which can override primary and secondary T cell activation signals [4]. Multiple T cell checkpoint molecules have been described, and the blockade of either of two of these inhibitory proteins, CTLA4 and PD1, has resulted in clinical benefit in several tumor types [6–9]. 4 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 Table 2. Key Targeted Therapy and Checkpoint Immunotherapy Combination Trials in Melanoma, Non-Small Cell Lung Carcinoma (NSCLC), and Renal Cell Carcinoma (RCC)[2_TD$IF]. Clinical Trial ID Indication Targeted Therapy Immunotherapy Phase Status Scheduling NCT01673854 Melanoma (BRAFMUT)a Vemurafenib Ipilimumab II Completed Sequential NCT01400451 Melanoma (BRAFMUT)a Vemurafenib Ipilimumab I Terminated Concurrent NCT01656642 Melanoma (BRAFMUT)a Vemurafenib or vemurafenib + cobimetinib Atezolizumab I Recruiting Concurrent NCT01767454 Melanoma (BRAFMUT)b Dabrafenib or dabrafenib + trametinib Ipilimumab I Completed Concurrent NCT01940809 Melanoma (BRAFMUT)b Dabrafenib or trametinib or dabrafenib + trametinib Ipilimumab + nivolumab I Recruiting Sequential NCT02224781 Melanoma (BRAFMUT)b Dabrafenib + trametinib Ipilimumab + nivolumab III Suspended Sequential NCT02200562 Melanoma (BRAFMUT)b Dabrafenib Ipilimumab I/II Recruiting Concurrent NCT02027961 Melanoma (BRAFMUT)b Trametinib or dabrafenib + trametinib Durvalumab I/II Ongoing Concurrent NCT02625337 Melanoma (BRAFMUT)b Dabrafenib + trametinib Pembrolizumab II Not open yet Concurrent NCT02130466 Melanoma (BRAFMUT)b Dabrafenib + trametinib Pembrolizumab I/II Recruiting Concurrent NCT02039674 NSCLC (EGFRMUT) Erlotinib or gefitinib Pembrolizumab I/II Recruiting Concurrent NCT01454102 NSCLC (EGFRMUT)c Erlotinib Nivolumab I Active, not recruiting Concurrent NCT02088112 NSCLC (EGFRMUT)c Erlotinib Durvalumab I Recruiting Concurrent NCT02630186 NSCLC (EGFRMUT)d Rociletinib Atezolizumab I/II Active, not recruiting Concurrent NCT02143466 NSCLC (EGFRMUT)e Osimertinib Durvalumab or durvalumab + tremelimumab I Recruiting Concurrent NCT02364609 NSCLC (EGFRMUT)f Afatinib Pembrolizumab I Recruiting Concurrent NCT02013219 NSCLC (ALK+)g or (EGFRMUT)c Alectinib or erlotinib Atezolizumab I Recruiting Concurrent NCT02393625 NSCLC (ALK+)h Ceritinib Nivolumab I Recruiting Concurrent NCT02511184 +g NSCLC (ALK ) Crizotinib Pembrolizumab I Recruiting Concurrent NCT02584634 NSCLC (ALK+)g or (ALK–)i Lorlatinib or crizotinib Avelumab I Recruiting Concurrent NCT02323126 NSCLC (MET+)j Capmatinib Nivolumab II Recruiting Concurrent NCT01988896 NSCLC Cobimetinib Atezolizumab I Recruiting Concurrent NCT02574078 NSCLC Erlotinib or crizotinib Nivolumab I/II Recruiting Concurrent NCT02210117 RCC Bevacizumab Nivolumab II Recruiting Concurrent NCT02420821 RCC Bevacizumab Atezolizumab III Recruiting Concurrent Trends in Immunology, Month Year, Vol. xx, No. yy 5 TREIMM 1288 No. of Pages 15 Table 2. (continued) Clinical Trial ID Indication Targeted Therapy Immunotherapy Phase Status Scheduling NCT02724878 RCC Bevacizumab Atezolizumab II Not open yet Concurrent NCT01984242 RCC Bevacizumab Atezolizumab II Active, not recruiting Concurrent NCT02348008 RCC Bevacizumab Pembrolizumab I/II Recruiting Concurrent NCT02684006 RCC Axitinib Avelumab III Not yet open Concurrent NCT02493751 RCC Axitinib Avelumab I Recruiting Concurrent NCT02133742 RCC Axitnib Pembrolizumab I Recruiting Concurrent NCT02496208 RCC Cabozantinib Nivolumab or nivolumab and ipilimumab I Recruiting Concurrent NCT02501096 RCC Levantinib Pembrolizumab I/II Recruiting Concurrent NCT02014636 RCC Pazopanib Pembrolizumab I Recruiting Concurrent NCT01472081 RCC Sunitinib or pazopanib Nivolumab I Active, not recruiting Concurrent NCT02298959 RCC Ziv-aflibercept Pembrolizumab I Recruiting Concurrent a BRAF V600 mutation. BRAF V600E or V600K mutation. EGFR mutation positive. d EGFR mutation (e.g., G719X, exon 19 deletion, L858R, L861Q) and absence of exon 20 insertion. e EGFR mutation positive and for T790M-directed EGFR TKI patients: documented T790M-positive status when patient started on the previous T790M-directed EGFR TKI. f EGFR activating mutations (exon 19 del, exon 21 L858R, L861Q, G718X) in patients who have radiologic and/or clinically progressive disease on erlotinib. g ALK positive. h ALK rearrangement. i ALK negative. j MET positive. b c CTLA4 is a receptor that inhibits early T cell activation and has an important role in the priming phase of the immune response [10,11]. Ipilimumab, an antibody that inhibits CTLA4 interactions with its ligands CD80 and CD86, is approved for the treatment of patients with advanced melanoma, based on clinical studies that demonstrated improvements in overall survival in a subset of patients [12–14]. While the exact determinants of clinical response to ipilimumab therapy are not well understood, studies have demonstrated that clinical benefit is associated with high tumor mutational load [15,16], high levels of tumor antigen-specific CD8 T cells [17], and high pretreatment levels of tumor-infiltrating lymphocytes [18]. PD1 is another inhibitory receptor that blocks T cell activation and is associated with chronically activated and exhausted T cells, such as those found in the tumor microenvironment [19–21]. It has two receptors, PDL1 and PDL2, which are expressed on antigen-presenting and other immune cells, as well as on tumor cells. Multiple antibodies that inhibit PD1 or PDL1 are in clinical development [22,23]. Nivolumab and pembrolizumab, two antibodies that target PD1 and block its interactions with PDL1 and PDL2, are approved for the treatment of advanced melanoma, non-small cell lung cancer (NSCLC), and renal cell carcinoma (RCC), based on clinical studies that demonstrated improvements in overall survival [24,25]. Similar to anti-CTLA4 therapy, the exact determinants of response to anti-PD1 and anti-PDL1 therapies are not well understood. However, clinical benefit is associated with high tumor mutational load [26], high pretreatment levels of PDL1 on tumor cells and tumor-infiltrating immune cells [27–29], and high pretreatment levels of tumor-infiltrating lymphocytes [30]. 6 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 The association of checkpoint inhibitor efficacy with tumor antigenicity and high pretreatment levels of intratumoral T cells suggests that agents that increase these factors may combine effectively with checkpoint therapies. Below, we highlight two examples of targeted therapies that promote these effects on host immunity and discuss their combinations with checkpoint therapies. Combinations of MAPK Pathway Inhibitors with Checkpoint Therapies The serine threonine kinase BRAF is mutated in approximately half of all malignant melanomas [31]. Among the reported mutations, substitutions involving the V600 amino acid residue are the most common. These mutations drive constitutive MAPK pathway signaling, promoting tumor cell proliferation and survival [31,32]. Multiple agents targeting the MAPK pathway have been approved for the treatment of BRAFV600[3_TD$IF] mutant melanoma, including two BRAF inhibitors, vemurafenib and dabrafenib (Table 1 and Figure 2A). Phase II and III clinical trials have reported response rates of approximately 50% for both inhibitors in patients with BRAF mutant melanoma, with significant improvements in progression-free survival (PFS) and overall survival (OS) compared with standard-of-care chemotherapy [33–35]. Although rapid and deep regressions are frequently observed with these therapies, resistance invariably develops. Clinically validated resistance mechanisms often involve reactivation of the MAPK pathway [36–38], suggesting that resistant tumors remain addicted to the MAPK pathway for survival. Combined BRAF + MEK inhibitor therapies, designed to address the aforementioned resistance mechanisms by targeting vertical nodes within the MAPK pathway, are now approved and exhibit incremental improvements in PFS and OS over single-agent BRAF inhibitors [39,40]. However, resistance remains a vexing problem [41]. In addition to serving as an oncogenic driver in melanoma, a growing body of data suggests that activating mutations in BRAF can promote an immune-compromised tumor microenvironment, such that inhibition of MAPK pathway signaling with BRAF and MEK inhibitors can counteract mechanisms of immune escape. One mechanism of MAPK pathway-driven immune evasion by melanoma cells is the downregulation of melanoma antigens. This was initially demonstrated by transient overexpression of mutant BRAF in melanoma cell lines, where elevated MAPK pathway signaling caused a marked reduction in the expression of the melanocyte differentiation antigen MART-1 [42]. Subsequently, inhibition of MAPK pathway signaling in BRAFV600E mutant melanoma cell lines and tumor digests was shown to drive increased expression of melanocyte differentiation antigens [42,43]. In addition, elevated melanoma antigen expression has been reported in biopsies from patients with BRAF mutant melanoma treated with MAPK pathway inhibitors; however, this induction was transient, with antigen expression returning to pretreatment levels at the time of progression on therapy [44]. Coupled with the potential of BRAF and MEK inhibitors to drive immunogenic tumor cell death [45], these therapy-induced increases in tumor antigen levels may result in enhanced priming of antitumor T cell responses. An additional mechanism by which BRAF and MEK inhibitors enhance host antitumor immunity is through increased intratumoral T cell infiltration. Multiple studies have reported significant increases in T cells in BRAF mutant melanoma tumors following treatment with MAPK pathway inhibitors [44,46,47]. These increases in intratumoral T cells could be due to direct modulation of T cell trafficking or could be secondary to increases in tumor cell antigenicity. Similar to the aforementioned transient induction of melanoma tumor antigens by MAPK pathway inhibitors, inhibitor-mediated increases in intratumoral T cells were also lost at the time of progression on therapy [44]. MAPK pathway inhibitors can also directly impact T cell function. Recent studies performed in immune-competent mice support a role for MEK inhibitors in potentiating the antitumor T cell response by protecting effector CD8 T cells from death by chronic T cell receptor stimulation [48]. However, MEK inhibitors can also have negative effects on naïve T cell proliferation, viability, and interferon gamma secretion [43,48,49]. Selective BRAFV600E[3_TD$IF] inhibitors Trends in Immunology, Month Year, Vol. xx, No. yy 7 TREIMM 1288 No. of Pages 15 (A) (B) ALK Ramucirumab EGFR Bevacizumab Aflibercept Gefinib Erlonib Afanib Osimernib Crizonib Cerinib Alecnib VEGF-A VEGF-C VEGF-D VEGF-B VEGFR1 VEGFR2 VEGFR3 RAS BRAF Vemurafenib dabrafenib MEK Tramenib cobimenib Other signaling pathways ERK Reduced tumor angen expression Reduced intratumoral T cells VEGFR kinase inhibitors (e.g., suninib, sorafenib, others) Dysfunconal tumor vasculature Reduced dendric cell differenaon and acvaon Figure 2. MAPK and VEGF Signaling Pathways and Inhibitors. (A) Approved therapeutic agents targeting the MAPK signaling pathway and select upstream receptor tyrosine kinases. Genes harboring frequent oncogenic alterations are highlighted in red. Oncogenic alterations can promote an immune-compromised tumor microenvironment through reduced tumor antigen expression and reduced intratumoral T cell infiltration, such that targeted inhibition of these nodes can counteract mechanisms of immune escape. (B) Approved therapeutic agents targeting VEGF/VEGFR signaling. VEGF/ VEGFR signaling can lead to dysfunctional vasculature that inhibits infiltration of T cells into the tumor, as well as reduced dendritic cell differentiation and activation, which may impair T cell priming. Inhibition of VEGF/VEGFR signaling can improve intratumoral immune cell infiltration and antitumor immune responses. do not exhibit negative effects on T cell function [43,47,50,51] and have been reported to induce T cell activation and function via paradoxical activation of the MAPK pathway upon T cell receptor signaling [52]. The effect of MAPK pathway inhibition on PD1 and PDL1 levels has also received substantial attention, with some variability in reported results. Transcript levels of both receptor and ligand were reported to be elevated in melanoma samples from patients receiving BRAF or BRAF + MEK inhibitor therapy [44], suggesting that combining PD1/PDL1 + MAPK pathway inhibition may improve antitumor immune responses. However, immunohistochemistry studies on larger sets of BRAFV600E mutant melanoma samples revealed no significant increase in overall tumor PDL1 staining when comparing baseline pretreatment samples to samples on-treatment or at time of progression, although subgroup analysis demonstrated that pretreatment PDL1-negative tumors exhibited a significant increase in PDL1 expression at the time of progression [46]. Elevated PDL1 expression has been reported in BRAF inhibitor-resistant melanoma cell lines [53,54], suggesting that evasion of the host immune system has an important role in mediating resistance to MAPK pathway inhibitors. However, this does not appear to be a common theme across all resistant cell lines, because additional studies reported PDL1 induction to be limited to cell lines whose resistance was not dependent on reactivation of the MAPK pathway [55]. Taken together, these findings suggest that inhibition of the MAPK pathway serves to enhance host antitumor immunity through multiple mechanisms, including elevation of melanoma antigen expression and improved T cell infiltration and function. These changes may serve to prime the 8 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 tumor microenvironment for response to immunotherapy. Given the significant clinical activity observed with both targeted and checkpoint therapies in BRAFV600E mutant melanoma, there has been great interest in combining these two modalities. The immune-stimulatory effects of MAPK pathway inhibitors, in addition to the direct effects on tumor cell proliferation and survival, provide a strong rationale for combining MAPK pathway inhibitors with T cell checkpoint inhibitors. A clinical study investigating the safety and efficacy of concurrent targeted therapy and checkpoint immunotherapy was recently completed in BRAFV600E/K mutant metastatic melanoma. In this study, ipilimumab was combined with dabrafenib in a doublet arm or with dabrafenib and trametinib in a triplet arm. Early reports from this Phase I/II study suggested that preliminary activity was observed in all patients in the doublet arm, as measured by a reduction in the sum of lesion diameters for index lesions [56]. Longer follow-up will be required to meaningfully assess any benefit of the dabrafenib + ipilimumab combination. While no doselimiting observations were reported in the doublet arm, the triplet combination of dabrafenib + trametinib + ipilimumab was poorly tolerated and was closed due to safety findings. Many additional clinical trials testing MAPK pathway inhibitors in combination with immunecheckpoint inhibitors are ongoing or planned (Table 2). These trials involve various BRAF and MEK inhibitors as well as checkpoint inhibitors targeting CTLA4, PD1, and PDL1. As data from these trials mature, they will provide greater insight into optimal dosing schedules, treatment related toxicities, and, most importantly, the targeted therapy and immunotherapy combinations that provide the greatest efficacy in the BRAF mutant melanoma setting. Combinations of VEGF Pathway Inhibitors with Checkpoint Therapies VEGF-A is a protein that is critical for the early development and differentiation of vascular and hematopoietic cells through binding to its receptors VEGFR1 and VEGFR2 [57]. VEGF-A is a clinically validated driver of tumor angiogenesis, and several therapeutic agents that target VEGF-A (bevacizumab, an anti-VEGF-A antibody; and aflibercept, a recombinant fusion protein containing the VEGF-A/B-binding domains of VEGFR1/2) or VEGF receptors (sunitinib and sorafenib, multikinase inhibitors that inhibit VEGFRs and other receptor tyrosine kinases; and ramucirumab, an anti-VEGFR2 antibody) are approved for the treatment of advanced colorectal cancer, non-squamous NSCLC, RCC, ovarian cancer, and glioblastoma (Table 1 and Figure 2B) [58,59]. VEGF-A reduces adhesion molecule expression on endothelial cells [60,61], which results in a dysfunctional tumor vasculature and inhibits the infiltration of T cells and other immune cells into the tumor [62–65]. Several studies have shown an association of tumor angiogenesis, tumor vascular dysfunction, or elevated VEGF-A levels with reductions in tumor T cell infiltration in human tumors [64,66,67], and one study documented that high serum VEGF-A levels are associated with lower overall survival under anti-CTLA4 therapy [68]. Studies in mice demonstrated that modulation or normalization of tumor vasculature can result in increased T cell recruitment and infiltration into tumors [69,70]. Treatment of mouse cancer models with inhibitors of VEGF-A or VEGFRs increases T cell recruitment and infiltration into tumors [71–73] and can be synergistic with anti-PD1 therapy [74]. Aside from its activity on the tumor vasculature to modulate host immunity, VEGF-A can also act directly on immune cells in an inhibitory manner. In vitro and mouse in vivo studies demonstrated that VEGF-A suppresses dendritic cell differentiation and activity [75–77], increases the expression of checkpoint molecules on CD8[3_TD$IF] T cells [78], and modulates the proliferation of regulatory T cells that inhibit effector T cell responses [79]. Studies of VEGF-A or VEGFR inhibition in patients with cancer are consistent with the immune biology of VEGF-A delineated by in vitro and mouse in vivo studies. Patients with RCC treated Trends in Immunology, Month Year, Vol. xx, No. yy 9 TREIMM 1288 No. of Pages 15 with bevacizumab or sunitinib exhibited increased intratumoral T cells, increased PDL1 expression in the tumor, and increased PD1 expression on tumor-infiltrating lymphocytes compared with untreated patients [80,81]. In addition, treatment of patients with colorectal, lung, or breast cancer with bevacizumab was associated with reductions in immature dendritic cells and improved dendritic cell antigen presentation [82]. Patients with RCC who were treated with sorafenib exhibited reductions in myeloid-derived suppressor cells and intratumoral regulatory T cells [83]. Several clinical studies combining VEGF-A or VEGFR inhibitors with checkpoint therapies have reported enhancements in tumor immune responses with associated clinical benefit. In a study of bevacizumab and ipilimumab combination therapy versus ipilimumab monotherapy in advanced metastatic melanoma, combination therapy resulted in increased adhesion molecule expression on tumor endothelial cells and increased intratumoral immune cell infiltration that was associated with clinical responses [84]. In RCC, combination studies of bevacizumab with the anti-PDL1 therapeutic MPDL3280A, as well as sunitinib with nivolumab, have been reported [85,86]. In a combination study of bevacizumab with MPDL3280A, intratumoral T cells were increased by treatment with bevacizumab alone, and were further increased upon combination with MPDL3280A [87]. Multiple clinical studies combining VEGF-A or VEGFR inhibitors with checkpoint therapies are either planned or ongoing (Table 2). It may also be interesting to assess combinations of checkpoint therapies with other modulators of the tumor vasculature aside from VEGF, such as the angiopoietin/Tie2 signaling pathway, which not only promotes tumor angiogenesis, but may also modulate inhibitory macrophages in the tumor microenvironment [88,89]. Considerations for the Clinical Development of Targeted and Checkpoint Therapy Combinations Some key considerations for the clinical development of targeted therapy and immunotherapy combinations include optimizing dosing regimens, minimizing treatment-related toxicities, and selecting appropriate endpoints to assess efficacy. Both concurrent and sequential dosing regimens of targeted therapies and immunotherapies are currently being assessed in clinical trials. There are obvious advantages to concurrent therapy administration, including a potential to maximize synergistic interactions between targeted therapy and immunotherapy, particularly with respect to creating a positive cycle where treatment with a targeted therapy may drive tumor antigen presentation, T cell infiltration, and PD1/PDL1 expression that could prime a tumor for a response to checkpoint inhibition. One consideration for concurrent administration of targeted therapies and immunotherapies is whether the targeted therapy inhibits patient immune responses, especially T cell function. This has been a particular focus in the case of combinations of MAPK pathway inhibitors with immunotherapies, with recent data suggesting that MEK inhibitors are compatible with checkpoint inhibitors, despite a dependence on the MAPK pathway for certain T cell functions [48]. In addition, while concurrent administration of targeted therapies and immunotherapies may offer the greatest potential for a synergistic response, it may also present greater risks of toxicity compared with sequential treatment regimens. A significant number of clinical trials in melanoma are testing the sequential administration of MAPK pathway inhibitors followed by checkpoint inhibitors. An important consideration favoring an initial treatment with targeted therapy is the relatively high rate of rapid clinical response that is often observed with agents directed towards oncogenic drivers. For patients presenting with advanced disease, an initial course of targeted therapy is likely to be a favored option for clinicians, whose initial priority is relief of disease burden [90]. However, some of the immunomodulatory benefits of targeted therapy may be short lived. For instance, increases in tumor infiltration of T cells, elevated expression of melanocyte differentiation antigens, and upregulation of PDL1 in patients with melanoma treated with vemurafenib were transient and had 10 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 disappeared by 4 weeks after the initiation of therapy [44]. Ultimately, sequential treatment of targeted therapy followed by immunotherapy will require a better understanding of the optimal timing for adding an immunotherapy to the treatment regime. The limited clinical experience in melanoma to date suggests that the immunotherapy should be added before relapse and disease progression on targeted therapy [91]. A major challenge for combinations of targeted therapies and immunotherapies is the potential for combined toxicity. This issue was highlighted by findings in an early clinical study testing concurrent treatment of vemurafenib and ipilimumab, which was terminated due to a high and unexpected incidence of hepatotoxicity [92]. These findings reinforced the potential for unpredicted toxicities with targeted therapy and immunotherapy combinations and emphasized the need to evaluate these combinations with carefully conducted clinical trials. To date, the toxicities observed with combinations of MAPK inhibitors and immunotherapies have been reversible and largely successfully addressed via clinical monitoring, drug holidays, changes in dose levels, and the administration of steroids [93,94]. Moving forward, a thorough preclinical assessment of the mechanism of action and risks associated with each potential combination of targeted therapy and immunotherapy may help limit the severity and incidence of toxicities in the clinic, as well as inform dose-sequencing and clinical-monitoring paradigms. One additional consideration in the design and execution of clinical studies is the choice of endpoints to define efficacy. Most clinical trials evaluating targeted cancer therapies use Response Evaluation Criteria in Solid Tumors (RECIST) to define a response to therapy. A significant reduction in tumor size using a radiographic assessment is considered a response by RECIST, whereas an increase in tumor size or the development of new lesions is considered to be evidence of disease progression, which often triggers a switch in therapy. However, a small subset of patients treated with immunotherapies have had a delayed or mixed clinical response, with some patients exhibiting an initial increase in the size of their lesions that was subsequently followed by a reduction in tumor volume, whereas, in other patients, new lesions can emerge before a response following treatment with immunotherapy [95–97]. The lag in response and the initial increase in lesion size, which has been termed ‘pseudoprogression’, is thought to reflect the mechanism of action of immunotherapies and may result from significant immune cell infiltration into the tumor. The phenomenon of pseudoprogression has stimulated a discussion on modifying the response criteria that specifically pertains to immunotherapy. Thus, clinical trials evaluating combinations of targeted therapies and immunotherapies may need to take into account the complexities of an immune-related response and modify their criteria for evaluating clinical benefit accordingly. Outstanding Questions What strategies should be taken to develop targeted therapies in combination with immunotherapies beyond CTLA4 and PD1/PDL1 checkpoint inhibitors, such as cancer vaccines, additional checkpoint molecules, T cell co-stimulatory molecules, or modulators of tumor-associated myeloid cells? Can biomarkers be identified that enable better patient selection and stratification for combination therapies, as well as more detailed assessments of therapeutic mechanisms in patients? As therapeutic response rates and response durability increase, will novel endpoints or more prolonged and complex clinical studies be needed to achieve registrational status for future therapeutic combinations? Will synergistic toxicities curtail the development of combinations of targeted therapy and immunotherapy? Can we better understand resistance mechanisms for immunotherapies and address them through combinations with targeted therapies? Concluding Remarks In this review, we have proposed a framework for considering combinations of targeted therapies and immunotherapies, in which targeted therapies may synergize with immunotherapies by enhancing complementary aspects of the cancer-immunity cycle, such as tumor antigenicity, T cell priming, and T cell trafficking and infiltration into tumors. We have utilized this framework in discussing combinations of targeted agents against the MAPK and VEGF pathways with checkpoint immunotherapies (Figure 1). We propose that the effects of targeted therapies on such aspects of host immunity may be used to guide and prioritize the testing of additional combinations of targeted therapies and immunotherapies to yield synergies in promoting antitumor immune responses. Anti-CTLA4 and anti-PD1/anti-PDL1 act primarily at distinct steps in the cancer immunity cycle, and this may affect their synergy with targeted therapies. Indeed, anti-CTLA4 and anti-PD1 therapies are synergistic when combined together, likely due to their complementary effects on T cell priming in the lymph nodes and T cell activation and killing in the tumor (Figure 1) [98,99]. It will be important to determine whether each checkpoint therapy synergizes better with targeted therapies that induce mechanisms that Trends in Immunology, Month Year, Vol. xx, No. yy 11 TREIMM 1288 No. of Pages 15 are more proximal or more distal to its point of activity within the cancer immunity cycle. For example, therapies that enhance tumor cell antigenicity or dendritic cell activity may synergize better with anti-CTLA4 than anti-PD1/anti-PDL1, given the potential of these mechanisms to more directly impact T cell priming as opposed to intratumoral T cell activation and killing. Similarly, therapies that enhance T cell trafficking and infiltration into tumors may synergize better with anti-PD1/anti-PDL1 than anti-CTLA4, given the potential of these mechanisms to more directly impact T cell killing of tumor cells compared with T cell priming in the lymph nodes. Beyond the MAPK and VEGF pathway examples that we have discussed in this review, other combinations of targeted therapies and immunotherapies are being assessed in the clinic; and the results of these trials will further inform our understanding of how to best combine these different therapeutic modalities. Of particular note are clinical studies of combinations of EGFR and ALK inhibitors with checkpoint inhibitors in NSCLC. In preclinical models, oncogenic alterations in EGFR and ALK have been shown to induce PDL1 expression, and activation of the PD1 pathway has been linked to immune escape in an EGFR-driven murine lung cancer model [100,101], thereby providing a rationale for combining EGFR and ALK inhibitors with checkpoint inhibitors. By contrast, it was recently observed that many EGFRmutant and ALK-translocated tumors have low levels of PDL1 expression and infiltrating CD8[3_TD$IF] T cells [102]. Furthermore, many patients presenting with EGFR mutant or ALK translocated NSCLC tend to be never- or light-smokers who harbor tumors with a relatively low nonsynonymous mutational burden [103], which may lead to a lower probability of response to PD1 blockade [26]. The outcomes of the clinical trials evaluating combinations of EGFR and ALK inhibitors with checkpoint inhibitors (Table 2) should provide further insights into the ability of these targeted therapies to prime the immune environment of the tumor for response to immunotherapy. Several emerging issues regarding combinations of targeted therapies and immunotherapies will need to be addressed in the coming years, as highlighted in the Outstanding Questions. In addition, ongoing work is identifying new opportunities for combination treatments with immunotherapies, based on mechanisms that elicit distinct and complementary aspects of the cancer-immunity cycle. Roles for radiation therapy [104,105] and chemotherapy [106] in complementing checkpoint inhibitors by enhancing aspects of cancer immunity, such as tumor antigen load, T cell priming, T cell trafficking, and T cell infiltration into tumors, are currently being examined. Moreover, several new pathways have recently been identified that may synergize with immunotherapy. A systematic analysis of specific pathways that are associated with low levels of intratumoral T cell infiltrate has revealed that the WNT/b-catenin [107], PTEN/PI3K [108], and PPARg and FGFR3 pathways [109] are associated with exclusion of T cells from solid tumors and, in the case of the WNT/b-catenin and PTEN/PI3K pathways, has further demonstrated that inhibition of these pathways can enhance intratumoral T cell infiltration and, therefore, are potential candidates for combination treatment with checkpoint inhibitors. Other work has demonstrated that molecules involved in epigenetic modifications can modulate tumor antigen expression [110] or suppress T cell infiltration in tumors [111,112] and, therefore, comprise additional candidates for combinations with checkpoint inhibitors. These and other pathways yet to be discovered may contribute to not only intrinsic resistance to immunotherapies, but also acquired resistance to immunotherapies through de novo mutations that lead to disease relapse. Understanding the immune-modulating activities of these pathways may lead to novel combinations of targeted therapies and immunotherapies with the potential to significantly improve the future treatment of [5_TD$IF]4cancer. Disclaimer Statement All authors are employed by Amgen, Inc. 12 Trends in Immunology, Month Year, Vol. xx, No. yy TREIMM 1288 No. of Pages 15 [6_TD$IF]Acknowledgments We thank Jackson Egen for assistance with figure illustrations. References 1. Chen, D.S. and Mellman, I. (2013) Oncology meets immunology: the cancer-immunity cycle. Immunity 39, 1–10 2. Muller, W.A. (2016) Localized signals that regulate transendothelial migration. Curr. Opin. Immunol. 38, 24–29 3. Slaney, C.Y. et al. (2014) Trafficking of T cells into tumors. Cancer Res. 74, 7168–7174 4. Chen, L. and Flies, D.B. (2013) Molecular mechanisms of T cell costimulation and co-inhibition. Nat. Rev. Immunol. 13, 227–242 5. Kim, H.J. and Cantor, H. (2014) The path to reactivation of antitumor immunity and checkpoint immunotherapy. Cancer Immunol. Res. 2, 926–936 6. Lesokhin, A.M. et al. (2015) On being less tolerant: enhanced cancer immunosurveillance enabled by targeting checkpoints and agonists of T cell activation. Sci. Trans. Med. 7, 280sr281 26. Rizvi, N.A. et al. (2015) Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 348, 124–128 27. Herbst, R.S. et al. (2014) Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 515, 563–567 28. Patel, S.P. and Kurzrock, R. (2015) PD-L1 expression as a predictive biomarker in cancer immunotherapy. Mol. Cancer Therapeutics 14, 847–856 29. Taube, J.M. et al. (2014) Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin. Cancer Res. 20, 5064–5074 30. Tumeh, P.C. et al. (2014) PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 515, 568–571 7. Sharma, P. and Allison, J.P. (2015) The future of immune checkpoint therapy. Science 348, 56–61 31. Davies, H. et al. (2002) Mutations of the BRAF gene in human cancer. Nature 417, 949–954 8. Shin, D.S. and Ribas, A. (2015) The evolution of checkpoint blockade as a cancer therapy: what's here, what's next? Curr. Opin. Immunol. 33, 23–35 32. Wan, P.T. et al. (2004) Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF. Cell 116, 855–867 9. Topalian, S.L. et al. (2015) Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell 27, 450–461 33. Ascierto, P.A. et al. (2013) Phase II trial (BREAK-2) of the BRAF inhibitor dabrafenib (GSK2118436) in patients with metastatic melanoma. J. Clin. Oncol. 31, 3205–3211 10. Chambers, C.A. et al. (2001) CTLA-4-mediated inhibition in regulation of T cell responses: mechanisms and manipulation in tumor immunotherapy. Annu. Rev. Immunol. 19, 565–594 34. Chapman, P.B. et al. (2011) Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 364, 2507–2516 11. Teft, W.A. et al. (2006) A molecular perspective of CTLA-4 function. Annu. Rev. Immunol. 24, 65–97 35. Hauschild, A. et al. (2012) Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet 380, 358–365 12. Hodi, F.S. et al. (2010) Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363, 711–723 13. Robert, C. et al. (2011) Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 364, 2517–2526 14. Schadendorf, D. et al. (2015) Pooled analysis of long-term survival data from Phase II and Phase III trials of ipilimumab in unresectable or metastatic melanoma. J. Clin. Oncol. 33, 1889–1894 15. Snyder, A. et al. (2014) Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 371, 2189–2199 16. Van Allen, E.M. et al. (2015) Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science 350, 207–211 17. Yuan, J. et al. (2011) Integrated NY-ESO-1 antibody and CD8+ T-cell responses correlate with clinical benefit in advanced melanoma patients treated with ipilimumab. Proc. Natl. Acad. Sci. U. S.A. 108, 16723–16728 18. Ji, R.R. et al. (2012) An immune-active tumor microenvironment favors clinical response to ipilimumab. Cancer Immunol. Immunother. 61, 1019–1031 19. Chen, L. and Han, X. (2015) Anti-PD-1/PD-L1 therapy of human cancer: past, present, and future. J. Clin. Invest. 125, 3384–3391 20. Keir, M.E. et al. (2008) PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 26, 677–704 21. Pauken, K.E. and Wherry, E.J. (2015) Overcoming T cell exhaustion in infection and cancer. Trends Immunol. 36, 265–276 22. Henick, B.S. et al. (2014) The PD-1 pathway as a therapeutic target to overcome immune escape mechanisms in cancer. Expert Opin. Ther. Targets 18, 1407–1420 23. Ohaegbulam, K.C. et al. (2015) Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol. Med. 21, 24–33 24. Gunturi, A. and McDermott, D.F. (2015) Nivolumab for the treatment of cancer. Expert Opin. Invest. Drugs 24, 253–260 25. Khoja, L. et al. (2015) Pembrolizumab. J. Immunother. Cancer 3, 36 36. Poulikakos, P.I. et al. (2011) RAF inhibitor resistance is mediated by dimerization of aberrantly spliced BRAF(V600E). Nature 480, 387–390 37. Shi, H. et al. (2014) Acquired resistance and clonal evolution in melanoma during BRAF inhibitor therapy. Cancer Discov. 4, 80–93 38. Van Allen, E.M. et al. (2014) The genetic landscape of clinical resistance to RAF inhibition in metastatic melanoma. Cancer Discov. 4, 94–109 39. Larkin, J. et al. (2014) Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N. Engl. J. Med. 371, 1867–1876 40. Robert, C. et al. (2015) Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med. 372, 30–39 41. Long, G.V. et al. (2014) Increased MAPK reactivation in early resistance to dabrafenib/trametinib combination therapy of BRAF-mutant metastatic melanoma. Nat. Commun. 5, 5694 42. Kono, M. et al. (2006) Role of the mitogen-activated protein kinase signaling pathway in the regulation of human melanocytic antigen expression. Mol. Cancer Res. 4, 779–792 43. Boni, A. et al. (2010) Selective BRAFV600E inhibition enhances T-cell recognition of melanoma without affecting lymphocyte function. Cancer Res. 70, 5213–5219 44. Frederick, D.T. et al. (2013) BRAF inhibition is associated with enhanced melanoma antigen expression and a more favorable tumor microenvironment in patients with metastatic melanoma. Clin. Cancer Res. 19, 1225–1231 45. Kroemer, G. et al. (2013) Immunogenic cell death in cancer therapy. Annu. Rev. Immunol. 31, 51–72 46. Kakavand, H. et al. (2015) PD-L1 expression and tumor-infiltrating lymphocytes define different subsets of MAPK inhibitortreated melanoma patients. Clin. Cancer Res. 21, 3140–3148 47. Liu, C. et al. (2013) BRAF inhibition increases tumor infiltration by T cells and enhances the antitumor activity of adoptive immunotherapy in mice. Clin. Cancer Res. 19, 393–403 48. Ebert, P.J. et al. (2016) MAP kinase inhibition promotes T cell and anti-tumor activity in combination with PD-L1 checkpoint blockade. Immunity 44, 609–621 Trends in Immunology, Month Year, Vol. xx, No. yy 13 TREIMM 1288 No. of Pages 15 49. DeSilva, D.R. et al. (1998) Inhibition of mitogen-activated protein kinase kinase blocks T cell proliferation but does not induce or prevent anergy. J. Immunol. 160, 4175–4181 72. Manning, E.A. et al. (2007) A vascular endothelial growth factor receptor-2 inhibitor enhances antitumor immunity through an immune-based mechanism. Clin. Cancer Res. 13, 3951–3959 50. Comin-Anduix, B. et al. (2010) The oncogenic BRAF kinase inhibitor PLX4032/RG7204 does not affect the viability or function of human lymphocytes across a wide range of concentrations. Clin. Cancer Res. 16, 6040–6048 73. Shrimali, R.K. et al. (2010) Antiangiogenic agents can increase lymphocyte infiltration into tumor and enhance the effectiveness of adoptive immunotherapy of cancer. Cancer Res. 70, 6171–6180 51. Hong, D.S. et al. (2012) BRAF(V600) inhibitor GSK2118436 targeted inhibition of mutant BRAF in cancer patients does not impair overall immune competency. Clin. Cancer Res. 18, 2326–2335 52. Callahan, M.K. et al. (2014) Paradoxical activation of T cells via augmented ERK signaling mediated by a RAF inhibitor. Cancer Immunol. Res. 2, 70–79 53. Jiang, X. et al. (2013) The activation of MAPK in melanoma cells resistant to BRAF inhibition promotes PD-L1 expression that is reversible by MEK and PI3K inhibition. Clin. Cancer Res. 19, 598–609 54. Liu, L. et al. (2015) The BRAF and MEK inhibitors dabrafenib and trametinib: effects on immune function and in combination with immunomodulatory antibodies targeting PD-1, PD-L1, and CTLA-4. Clin. Cancer Res. 21, 1639–1651 55. Atefi, M. et al. (2014) Effects of MAPK and PI3K pathways on PDL1 expression in melanoma. Clin. Cancer Res. 20, 3446–3457 56. Puzanov, I. et al. (2014) Phase 1 study of the BRAF inhibitor dabrafenib (D) with or without the MEK inhibitor trametinib (T) in combination of ipilimumab (Ipi) for V600E/K mutation-positive unresectable or metastatic melanoma (MM). J. Clin. Oncol. 32, Abstr 2511 57. Ferrara, N. and Davis-Smyth, T. (1997) The biology of vascular endothelial growth factor. Endocr. Rev. 18, 4–25 58. Ellis, L.M. and Hicklin, D.J. (2008) VEGF-targeted therapy: mechanisms of anti-tumour activity. Nat. Rev. Cancer 8, 579–591 59. Meadows, K.L. and Hurwitz, H.I. (2012) Anti-VEGF therapies in the clinic. Cold Spring Harb. Perspect. Med. 2, a006577 60. Dirkx, A.E. et al. (2003) Tumor angiogenesis modulates leukocyte-vessel wall interactions in vivo by reducing endothelial adhesion molecule expression. Cancer Res. 63, 2322–2329 61. Griffioen, A.W. et al. (1996) Tumor angiogenesis is accompanied by a decreased inflammatory response of tumor-associated endothelium. Blood 88, 667–673 62. Castermans, K. and Griffioen, A.W. (2007) Tumor blood vessels, a difficult hurdle for infiltrating leukocytes. Biochim. et Biophys. Acta 1776, 160–174 63. Huang, Y. et al. (2013) Vascular normalization as an emerging strategy to enhance cancer immunotherapy. Cancer Res. 73, 2943–2948 64. Lanitis, E. et al. (2015) Targeting the tumor vasculature to enhance T cell activity. Curr. Opin. Immunol. 33, 55–63 65. Peske, J.D. et al. (2015) Control of CD8 T-cell infiltration into tumors by vasculature and microenvironment. Adv. Cancer Res. 128, 263–307 66. Bouma-ter Steege, J.C. et al. (2004) Angiogenic profile of breast carcinoma determines leukocyte infiltration. Clin. Cancer Res. 10, 7171–7178 67. Zhang, L. et al. (2003) Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N. Engl. J. Med. 348, 203–213 68. Yuan, J. et al. (2014) Pretreatment serum VEGF is associated with clinical response and overall survival in advanced melanoma patients treated with ipilimumab. Cancer Immunol. Res. 2, 127–132 69. Dirkx, A.E. et al. (2006) Anti-angiogenesis therapy can overcome endothelial cell anergy and promote leukocyte-endothelium interactions and infiltration in tumors. FASEB J 20, 621–630 70. Hamzah, J. et al. (2008) Vascular normalization in Rgs5deficient tumours promotes immune destruction. Nature 453, 410–414 71. Huang, Y. et al. (2012) Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. Proc. Natl. Acad. Sci. U.S.A. 109, 17561–17566 14 Trends in Immunology, Month Year, Vol. xx, No. yy 74. Yasuda, S. et al. (2013) Simultaneous blockade of programmed death 1 and vascular endothelial growth factor receptor 2 (VEGFR2) induces synergistic anti-tumour effect in vivo. Clin. Exp. Immunol. 172, 500–506 75. Alfaro, C. et al. (2009) Influence of bevacizumab, sunitinib and sorafenib as single agents or in combination on the inhibitory effects of VEGF on human dendritic cell differentiation from monocytes. Br. J. Cancer 100, 1111–1119 76. Gabrilovich, D.I. et al. (1996) Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nat. Med. 2, 1096–1103 77. Gabrilovich, D.I. et al. (1999) Antibodies to vascular endothelial growth factor enhance the efficacy of cancer immunotherapy by improving endogenous dendritic cell function. Clin. Cancer Res. 5, 2963–2970 78. Voron, T. et al. (2015) VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J. Exp. Med. 212, 139–148 79. Terme, M. et al. (2013) VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res. 73, 539–549 80. Guislain, A. et al. (2015) Sunitinib pretreatment improves tumorinfiltrating lymphocyte expansion by reduction in intratumoral content of myeloid-derived suppressor cells in human renal cell carcinoma. Cancer Immunol. Immunother. 64, 1241–1250 81. Liu, X.D. et al. (2015) Resistance to antiangiogenic therapy is associated with an immunosuppressive tumor microenvironment in metastatic renal cell carcinoma. Cancer Immunol. Res. 3, 1017–1029 82. Osada, T. et al. (2008) The effect of anti-VEGF therapy on immature myeloid cell and dendritic cells in cancer patients. Cancer Immunol. Immunother. 57, 1115–1124 83. Desar, I.M. et al. (2011) Sorafenib reduces the percentage of tumour infiltrating regulatory T cells in renal cell carcinoma patients. Int. J. Cancer 129, 507–512 84. Hodi, F.S. et al. (2014) Bevacizumab plus ipilimumab in patients with metastatic melanoma. Cancer Immunol. Res. 2, 632–642 85. Amin, A. et al. (2014) Nivolumab (anti-PD1; BMS-936558, ONO4538) in combination with sunitinib or pazopanib in patients (pts) with metastatic renal cell carcinoma (mRCC). J. Clin. Oncol. 32, Abstr 5010 86. Lieu, C. et al. (2014) Safety and efficacy of MPDL3280A (anti– PDL1) in combination with bevacizumab (BEV) and/or chemotherapy (chemo) in patients (PTS) with locally advanced or metastatic solid tumors. Ann. Oncol. 25, iv361 87. Sznol, M. et al. (2015) Phase Ib evaluation of MPDL3280A (anti– PDL1) in combination with bevacizumab (bev) in patients (pts) with metastatic renal cell carcinoma (mRCC). J. Clin. Oncol. 33, Abstr 410 88. Augustin, H.G. et al. (2009) Control of vascular morphogenesis and homeostasis through the angiopoietin-Tie system. Nat. Rev. Mol. Cell Biol. 10, 165–177 89. Fiedler, U. and Augustin, H.G. (2006) Angiopoietins: a link between angiogenesis and inflammation. Trends Immunol. 27, 552–558 90. Gibney, G.T. and Atkins, M.B. (2015) Immunotherapy or molecularly targeted therapy: what is the best initial treatment for stage IV BRAF-mutant melanoma? Clin. Adv. Hematol. Oncol. 13, 451–458 91. Ackerman, A. et al. (2014) Outcomes of patients with metastatic melanoma treated with immunotherapy prior to or after BRAF inhibitors. Cancer 120, 1695–1701 92. Ribas, A. et al. (2013) Hepatotoxicity with combination of vemurafenib and ipilimumab. N. Engl. J. Med. 368, 1365–1366 93. Kim, T. et al. (2014) Combining targeted therapy and immune checkpoint inhibitors in the treatment of metastatic melanoma. Cancer Biol. Med. 11, 237–246 TREIMM 1288 No. of Pages 15 94. Wargo, J.A. et al. (2014) Universes collide: combining immunotherapy with targeted therapy for cancer. Cancer Discov. 4, 1377–1386 95. Chiou, V.L. and Burotto, M. (2015) Pseudoprogression and immune-related response in solid tumors. J. Clin. Oncol. 33, 3541–3543 96. Di Giacomo, A.M. et al. (2009) Therapeutic efficacy of ipilimumab, an anti-CTLA-4 monoclonal antibody, in patients with metastatic melanoma unresponsive to prior systemic treatments: clinical and immunological evidence from three patient cases. Cancer Immunol. Immunother. 58, 1297–1306 97. Wolchok, J.D. et al. (2009) Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin. Cancer Res. 15, 7412–7420 98. Das, R. et al. (2015) Combination therapy with anti-CTLA-4 and anti-PD-1 leads to distinct immunologic changes in vivo. J. Immunol. 194, 950–959 99. Larkin, J. et al. (2015) Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 373, 23–34 100. Akbay, E.A. et al. (2013) Activation of the PD-1 pathway contributes to immune escape in EGFR-driven lung tumors. Cancer Discov. 3, 1355–1363 101. Ota, K. et al. (2015) Induction of PD-l1 Expression by the EML4-ALK oncoprotein and downstream signaling pathways in non-small cell lung cancer. Clin. Cancer Res. 21, 4014– 4021 102. Gainor, J.F. et al. (2015) Clinical correlation and frequency of programmed death ligand-1 (PD-L1) expression in EGFR-mutant and ALK-rearranged non-small cell lung cancer. J. Clinical Oncol. 33, Abstr 8012 103. Cancer Genome Atlas Research (2014) Comprehensive molecular profiling of lung adenocarcinoma. Nature 511, 543–550 104. Bernstein, M.B. et al. (2016) Immunotherapy and stereotactic ablative radiotherapy (ISABR): a curative approach? Nat. Rev. Clin. Oncol. Published online March 8, 2016. http://dx.doi.org/ 10.1038/nrclinonc.2016.30 105. Kalbasi, A. et al. (2013) Radiation and immunotherapy: a synergistic combination. J. Clin. Invest. 123, 2756–2763 106. Galluzzi, L. et al. (2015) Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell 28, 690–714 107. Spranger, S. et al. (2015) Melanoma-intrinsic beta-catenin signalling prevents anti-tumour immunity. Nature 523, 231–235 108. Peng, W. et al. (2016) Loss of PTEN Promotes Resistance to T Cell-Mediated Immunotherapy. Cancer Discov. 6, 202–216 109. Sweis, R.F. et al. (2015) Molecular driver of the non-T cellinflamed tumor microenvironment in urothelial bladder cancer. J. Clin. Oncol. 33, Abstr 4511 110. Chiappinelli, K.B. et al. (2016) Combining epigenetic and immunotherapy to combat cancer. Cancer Res. 76, 1683 111. Nagarsheth, N. et al. (2016) PRC2 epigenetically silences Th1type chemokines to suppress effector T-cell trafficking in colon cancer. Cancer Res. 76, 275–282 112. Peng, D. et al. (2015) Epigenetic silencing of TH1-type chemokines shapes tumour immunity and immunotherapy. Nature 527, 249–253 Trends in Immunology, Month Year, Vol. xx, No. yy 15