Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
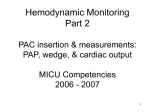
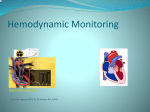
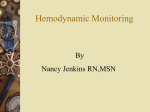
Cardiovasc Eng DOI 10.1007/s10558-010-9113-0 ORIGINAL PAPER Afterload Assessment With or Without Central Venous Pressure: A Preliminary Clinical Comparison Glen Atlas • Jay Berger • Sunil Dhar Ó Springer Science+Business Media, LLC 2010 Abstract A clinical comparison, of two methods of afterload assessment, has been made. The first method, systemic vascular resistance index (SVRi), is based upon the traditional formula for afterload which utilizes central venous pressure (CVP), as well as cardiac index (Ci), and mean arterial blood pressure (MAP). The second method, total systemic vascular resistance index (TSVRi), also uses MAP and Ci. However, TSVRi ignores the contribution of CVP. This preliminary examination, of 10 randomlyselected ICU patients, has shown a high degree of correlation (ranging from 90 to 100%) between SVRi and TSVRi (P \ 0.0001). Furthermore, there was also a high degree of correlation (ranging from 94 to 100%) noted between the hour-to-hour change in SVRi with the hour-tohour change in TSVRi (P \ 0.0001). The results, of this pilot study, support the premise that the use of CVP may not always be necessary for afterload evaluation in the clinical setting. Minimally-invasive means of measuring both Ci and MAP, without CVP, may be adequate for use in assessing afterload. Keywords Systemic vascular resistance index Total systemic vascular resistance index Central venous pressure Pulmonary artery occlusion catheter Introduction Examining SVRi Clinicians have typically used systemic vascular resistance index (SVRi) as a measure of afterload in the management of critically ill patients (Melo and Peters 1999) as well as those undergoing extensive cardiac, vascular, and thoracic surgical procedures (Barash et al. 2009). SVRi is defined as (Li 2000, 2004): SVRi ¼ G. Atlas (&) J. Berger Department of Anesthesiology, University of Medicine and Dentistry of NJ, Newark, NJ, USA e-mail: [email protected] G. Atlas Department of Chemistry, Chemical Biology, and Biomedical Engineering, Stevens Institute of Technology, Hoboken, NJ, USA S. Dhar Department of Mathematical Sciences, New Jersey Institute of Technology, Newark, NJ, USA S. Dhar Center for Applied Mathematics and Statistics, New Jersey Institute of Technology, Newark, NJ, USA ðMAP CVPÞ 80 Ci ð1Þ where MAP is mean arterial pressure, CVP is central venous pressure, and Ci is cardiac index. Note that the constant 80 allows for SVRi to be expressed with the dimensions of: dyne s cm-5 m-2 or ‘‘resistance units’’. A list of abbreviations, dimensions, and associated terminology is shown in Table 1. Traditionally, the determination of SVRi has required invasive hemodynamic monitoring with a pulmonary artery occlusion catheter (PAOC) to provide measurements of both Ci and CVP. Note that MAP can be obtained noninvasively, with a blood pressure cuff, or in a minimallyinvasive manner with a peripherally-placed arterial catheter.1 1 Typically, the radial artery is used for this purpose. 123 Cardiovasc Eng Table 1 List of abbreviations, dimensions, and terminology a Based upon patient height b Based upon patient body surface area Abbreviation Meaning Dimensions BMi Body mass indexa kg m-2 CAD Coronary artery disease Ci Cardiac indexb CVP Central venous pressure mmHg DBP Diastolic blood pressure mmHg DM Diabetes mellitus l min-1 m-2 EDM Esophageal Doppler monitor EF Ejection fraction HTN Hypertension MAP Mean arterial pressure OSA Obstructive sleep apnea % mmHg PAOC Pulmonary artery occlusion catheter SBP Systolic blood pressure SVRi Systemic vascular resistance indexb TSVRi mmHg Total systemic vascular resistance index The clinical utility of PAOCs has been questioned as outcome studies have generally not supported their use (ASA 2003; Sandham et al. 2003; NHLBI 2006; Warzawski et al. 2003). Furthermore, minimally-invasive and noninvasive means of measuring Ci have emerged. These technologies include the esophageal Doppler monitor (EDM) or CardioQÒ (Deltex Medical, UK) and the FloTracÒ (Edwards Lifesciences, USA).2 Note that the EDM determines Ci using the velocity of blood flow in the distal aorta (Dark and Singer 2004). Whereas the FlowTracÒ requires a peripheral arterial catheter to measure pulse pressure and uses a ‘‘pulse contour analysis’’ method to estimate cardiac output (Manecke 2005). The assumptions made with pulse contour analysis may be erroneous as clinical comparisons, of this device with the EDM, have demonstrated significant inconsistencies in stroke volume determination (Chatti et al. 2009). Measurement of the change in electrical impedance or ‘‘bioimpedance’’ of the thorax, or whole-body, as a function of a time, has also been developed to non-invasively assess Ci (Barin et al. 2000; Ouzounian et al. 1996). Unfortunately, this method has also demonstrated inconsistent correlation with traditional methods of measuring cardiac output (Imhoff et al. 2000; Simon et al. 2009). None of these minimally-invasive techniques, of Ci evaluation, allow for CVP measurement. An ideal method of afterload assessment would therefore also be minimally invasive and allow for continuous measurements. It should be noted that PAOCs only allow for determination of SVRi on an intermittent basis. dyne s cm-5 m-2 (resistance units) b dyne s cm-5 m-2 (resistance units) Examining TSVRi Another method of afterload assessment can be defined as total systemic vascular resistance (TSVRi) in which the contribution of CVP is ignored (Wang et al. 2008; Atlas 2008): TSVRi ¼ MAP 80 Ci Thus, the purpose of this study was to assess the correlation of SVRi to TSVRi using the data acquired from PAOCs. Therefore, the contribution of CVP, to afterload assessment, could be made. In addition, the hour-to-hour changes in both SVRi and TSVRi were also examined. This was done to determine how changes in CVP effect changes in afterload. Ultimately, the use of minimally-invasive and noninvasive devices could possibly be utilized, for the assessment of afterload, without the potential complications associated with pulmonary artery cannulation. These complications are summarized in Table 2 (ASA 2003). Differential Analysis A differential examination of both SVRi and TSVRi was also made to assess the hour-to-hour changes in these values. It should be noted that clinicians frequently examine the ‘‘trend’’ in afterload over time. Thus, the hourto-hour changes in SVRi and TSVRi are defined as: DSVRi ðkÞ ¼ SVRi ðk þ 1Þ SVRi ðkÞ; k ¼ 1; 2. . .ðN 1Þ 2 Atys Medical (France) also manufactures an EDM. However, it is not currently available in the USA. 123 ð2Þ and ð3Þ Cardiovasc Eng Table 2 List of complications associated with PAOCs (ASA 2003) Complication Incidence in most studies (%) Arterial puncture B3.6 0.3–1.9 Minor dysrthymias [20 Severe dysrthymias (ventricular tachycardia or fibrillation) 0.3–3.8 Pulmonary artery rupture 0.03–0.7 Positive catheter-tip cultures C19 Catheter-related sepsis 0.7–3.0 Venous thrombosis 0.5–3.0 Pulmonary infarction 0.1–2.6 Valvular/endocardial vegetations or endocarditis 2.2–7.1 DTSVRi ðkÞ ¼ TSVRi ðk þ 1Þ TSVRi ðkÞ; k ¼ 1; 2. . .ðN 1Þ MAP = ð4Þ Note that k ranges from the first hour to the hour preceding the final hour (N - 1). Where N represents the final hour. The mathematical relationship, between DSVRi and DTSVRi, using both an algebraic method as well as the definition of the total differential, is documented in the Appendix. 2 1 DBP + SBP 3 3 ð5Þ As this was a preliminary or ‘‘pilot’’ study, no attempt to stratify data, based upon patient acuity, severity, or survival, was made. Furthermore, the hemodynamic influence, of any of each patient’s medications, such as sedatives or vasoactive medications, was also not included. SVRi and TSVRi were calculated, for each hour, using Eqs. 1 and 2 respectively. Similarly, DSVRi and DTSVRi were also calculated, on an hourly basis, using Eqs. 3 and 4. 3000.0 Resistance Units (dyne·s·cm-5·m-2) Pneumothorax Care Unit (CTICU) at University Hospital/Newark. Note that this study was strictly a retrospective chart review of preexisting data. Each patient’s demographic information is shown in Table 3. Hemodynamic data, from all 10 patients, were initially obtained each hour for at least 24 h. These data included: Ci, CVP, and MAP. Note that MAP was determined from either an indwelling arterial catheter or a non-invasive blood pressure cuff. For the purposes of this study, MAP was calculated using (Li 2000, 2004): Methods Data Acquisition and Analysis SVRi and TSVR i Patient #1 2500.0 2000.0 1500.0 1000.0 SVRi TSVRi 500.0 1 After institutional review board approval, the medical records of 10 randomly-selected patients, whose treatment had included indwelling PAOCs, were examined. All patients had been admitted to the Cardiothoracic Intensive 3 5 7 9 11 13 15 17 19 21 23 25 Time (hours) Fig. 1 SVRi and TSVRi calculated, on an hourly basis, using the data from patient #1 Table 3 Demographic data of the ten randomly-selected cardiothoracic ICU patients HTN CAD DM Tobacco OSA EF Patient Age Gender Weight Height BMi (kg m-2) use (years) (kg) (m) Procedure 1 46 Male 116 1.85 33.64 ? Ascending aortic aneurysm 2 65 Male 124 1.80 38.07 ? 3 64 Male 79 1.72 26.30 ? ? 4 76 Male 73 1.70 25.06 ? ? 5 72 Female 57 1.57 22.86 ? 6 47 Female 94 1.65 34.61 ? 7 53 Male 104 1.52 44.91 ? 8 70 Male 106 1.72 35.58 ? 9 62 Male 70 1.72 23.41 10 57 Female 80 1.75 25.99 ? ? ? 50% ? ? 55–60% Esophagectomy ? 55% Coronary artery bypass graft(s)/mitral valve replacement ? ? 75% Coronary artery bypass graft(s) ? ? 70% Aortic valve replacement ? ? ? ? 25–30% Coronary artery bypass graft(s)/mitral valve replacement ? ? 56–60% Mitral valve repair ? 50% ? ? 40–45% Coronary artery bypass graft(s) Coronary artery bypass graft(s) ? ? 50% Mitral valve replacement 123 Cardiovasc Eng Results Fig. 2 A linear correlation, between SVRi and TSVRi, is illustrated using the data from patient #1 Resistance Units (dyne·s·cm-5·m-2) ΔSVRi and ΔTSVRi Patient #1 Based upon this preliminary study, SVRi and TSVRi are closely correlated. This is exemplified in both Figs. 1 and 2 which graphically demonstrate the data from patient #1. The correlation coefficients, from all ten patients’ data, ranged from 90 to 100%. Furthermore, all correlation coefficients were statistically significant (P \ 0.0001). Similarly, DSVRi and DTSVRi, which represent the hour-to-hour changes in SVRi and TSVRi, were also highly correlated. These correlation coefficients ranged from 94 to 100% (P \ 0.0001). Figures 3 and 4, which are also based upon the data from patient #1, illustrate this relationship. All correlation coefficients and their associated 95% confidence intervals are documented in Table 4. Discussion Time (hours) Fig. 3 Hour-to-hour changes in SVRi and TSVRi using the data from patient #1. These changes are referred to as DSVRi and DTSVRi respectively Statistical analysis was accomplished, on a patient-bypatient basis, using a Pearson product-moment correlation coefficient (Kutner et al. 2004; Kreyszig 1999). In addition, a Fisher’s z-transformation was also used to determine statistical significance, and associated confidence intervals, from the correlation coefficients derived from each patient’s data (Hawkins 1989). Furthermore, it was assumed that all data points were from a bivariate normal distribution. The assessment of afterload remains an important aspect of hemodynamic monitoring during anesthesia and critical care situations. Specifically, clinical conditions such as: septicemia, adrenal insufficiency, and pancreatitis frequently require afterload measurement (Melo and Peters 1999). In addition, cardiac, thoracic, and vascular surgical procedures also may necessitate intraoperative and postoperative afterload assessment (Barash et al. 2009). Furthermore, severely injured patients, particularly those with neurogenic shock (Bilello et al. 2003) or with systemic inflammatory response syndrome (SIRS) (Cremer et al. 1996; Carrel et al. 2000; Kohsaka et al. 2005), may require afterload measurements. Other conditions requiring possible afterload assessment include: hypertensive crisis, congestive heart failure, aortic dissection, hepatic transplantation, burn injury, and the management of pheochromocytoma (Barash et al. 2009). Δ Fig. 4 A linear correlation, between DTSVRi and DSVRi, is documented using the data from patient #1 Δ 123 * P \ 0.0001 0.94* (0.88, 0.97) 0.99* (0.98, 1.00) 1.00* (0.99, 1.00) 0.99* (0.98, 1.00) 0.93* (0.87, 0.97) 0.97* (0.93, 0.98) 0.97* (0.93, 0.99) 0.96* (0.91, 0.98) 1.00* (0.99, 1.00) 1.00* (0.99, 1.00) 0.97* (0.94, 0.99) 0.97* (0.93, 0.99) 0.99* (0.97, 0.99) 0.99* (0.99, 1.00) 0.94* (0.85, 0.97) 0.95* (0.87, 0.98) 0.92* (0.83, 0.97) 0.90* (0.77, 0.95) 0.91* (0.79, 0.96) TSVRi versus SVRi DTSVRi versus DSVRi 0.96* (0.91, 0.98) 8 7 6 5 4 3 2 1 Patient Table 4 The correlation coefficient, R (in bold), and the corresponding 95% confidence intervals for both TSVRi versus SVRi and DTSVRi versus DSVRi 9 10 Cardiovasc Eng However, the use of PAOCs has been associated with questionable benefit as well as significant morbidity, mortality, and economic cost (ASA 2003; Domino et al. 2004; Stewart et al. 1998). In particular, the rising incidence of antibiotic-resistant nosocomial infections may further question, and limit, the use of these highly invasive hemodynamic monitors (Blot et al. 2005; Richards et al. 2000). Minimally-invasive hemodynamic monitors, specifically the EDM, have become well established as reliable, safe, and accurate (Madan et al. 1999; DiCorte et al. 2000; Dark and Singer 2004). Furthermore, the EDM can be placed either orally, in intubated patients, or nasally, in awake patients (Atlas and Mort 2001; Dodd 2002). Whereas the FlowTracÒ requires a peripheral arterial cannula. It should be noted that both of these instruments provide approximations of cardiac output. However, in clinical trials, the EDM has been shown to provide reproducible and reliable measurements of cardiac output (Singer et al. 1989; Valtier et al. 1998). In addition, the EDM is extremely accurate in measuring changes in cardiac output (DiCorte et al. 2000; Dark and Singer 2004). Therefore, the ability to assess afterload, with minimally-invasive devices, without CVP measurement, could offer significant benefit in patient safety. This preliminary study has shown that CVP appears to play a minor role in afterload assessment. Furthermore, the hour-to-hour changes in afterload appear to be minimally affected by the exclusion of CVP. However, specific clinical conditions may nonetheless require CVP measurement for management purposes. These would include such pathological states as: superior vena cava syndrome, congenital cardiac anomalies, intracardiac tumors, and cardiac tamponade. These conditions can create significant increases in CVP by restricting venous blood flow (Magder 2005). Furthermore, jugular venous distention (JVD), which is a diagnostic ‘‘hallmark’’ of CHF, is also associated with an increase in central venous pressure (Drazner et al. 2001). However, invasive monitoring of CVP is rarely necessary for the clinical diagnosis and management of this common condition (Senni et al. 1998). Certain clinical situations may artificially alter CVP. The use of positive end-expiratory pressure (PEEP), for patients with severe pulmonary disease, is one example (Magder 2005). In addition, the simultaneous use of the central venous cannula, for intravenous fluid administration during CVP measurements, may produce erroneous data (Ho et al. 2005). Furthermore, CVP may not be meaningful for patients who are in the prone or lateral decubitus positions (Soliman et al. 1998). A malpostioned pressure transducer can also significantly change CVP measurements (Magder 2005). Therefore, in these clinical situations, TSVRi may be advantageous over SVRi due to the possible inaccuracy of CVP. 123 Cardiovasc Eng Continuous afterload assessment would also be useful in ‘‘highly critical’’ situations. These would possible include patients on potent vasoactive medications for treatment during shock or sepsis. Patients undergoing removal of a pheochromocytoma may also benefit from this. Lastly, other hemodynamic parameters and terminology, associated with afterload assessment, exist. These include: pulse wave velocity, impedance, and characteristic impedance (Segers et al. 2007; Nichols and O’Rourke 2005; Milnor 1989). However, SVR and SVRi remain the ‘‘mainstays’’ of clinical afterload measurement within the hospital-based clinical community. CVP1 CVP2 Ci1 Ci2 CVP1 CVP2 thus: 0 Ci1 Ci2 ð4AÞ Finally: DSVRi DTSVRi ð5AÞ This concept can also be illustrated using the definition of the total differential: DSVRi ¼ oSVRi oSVRi oSVRi DMAP þ DCVP DCi þ oMAP oCi oCVP ð6AÞ and DTSVRi ¼ oTSVRi oTSVRi DMAP þ DCi oMAP oCi ð7AÞ Conclusions This preliminary study has favorably compared, and correlated, afterload assessment with CVP measurement (SVRi) to afterload assessment without CVP measurement (TSVRi). Further research, which would include prospective trials to assess the benefits, risks, and limitations of TSVRi measurement, appear indicated. In addition, these studies could be carried out with minimally-invasive hemodynamic monitors. A clinical comparison, of various means of afterload assessment, could then be implemented. Thus, a comparison of SVRi to TSVRi, with respect to patient outcome, complications, and cost, could be made. Appendix The Interrelationship Between DSVRi and DTSVRi DSVRi is calculated using the definition of SVRi from Eq. 1: ðMAP2 CVP2 Þ ðMAP1 CVP1 Þ DSVRi ¼ 80 80 Ci2 Ci1 ð1AÞ Rearrangement yields: MAP2 MAP1 CVP1 CVP2 DSVRi ¼ 80 þ 80 Ci2 Ci1 Ci1 Ci2 ð2AÞ Substituting the definition of TSVRi from Eq. 2 results in: CVP1 CVP2 DSVRi ¼ DTSVRi þ 80 ð3AÞ Ci1 Ci2 Realizing that: 123 oSVRi oCVP DCVP oTSVRi oSVRi oMAP and oCi Since oSVRi oMAP 0 then DSVRi DTSVRi . Also: i oTSVR oCi . References American Society of Anesthesiologists (ASA). Task force on guidelines for pulmonary artery catheterization. Practice guidelines for pulmonary artery catheterization. Anesthesiology. 2003; 99(4):988–1014. Atlas GM. Development and application of a logistic-based systolic model for hemodynamic measurements using the esophageal Doppler monitor. Cardiovasc Eng. 2008;8(3):159–73. Atlas G, Mort T. Placement of the esophageal Doppler ultrasound monitor probe in awake patients. Chest. 2001;119:319. Milnor WR. Vascular impedance. In: Hemodynamics. 2nd ed. Baltimore: Williams & Wilkins;(1989). pp. 167–203. Barash PG, Cullen BF, Stoelting RK. Clinical anesthesia. 6th ed. Phila: Lippincott Williams and Wilkins; 2009. Barin E, Haryadi DG, Schookin SI, Westenskow DR, Zubenko VG, Beliaev KR, Morozov AA. Evaluation of a thoracic bioimpedance cardiac output monitor during cardiac catheterization. Crit Care Med. 2000;28(3):698–702. Bilello JF, Davis JW, Cunningham MA, Groom TF, Lemaster D, Sue LP. Cervical spinal cord injury and the need for cardiovascular intervention. Arch Surg. 2003;138:1127–9. Blot SI, Depuydt P, Annemans L, Benoit D, Hoste E, De Waele JJ, Decruyenaere J, Vogelaers D, Colardyn F, Vandewoude KH. Clinical and economic outcomes in critically ill patients with nosocomial catheter-related bloodstream infections. Clin Infect Dis. 2005;41:1591–8. Carrel T, Englberger L, Mohacsi P, Neidhart P, Schmidli J. Low systemic vascular resistance after cardiopulmonary bypass: incidence, etiology, and clinical importance. J Card Surg. 2000;15: 347–53. Chatti R, de Rudniki S, Marqué S, Dumenil AS, Descorps-Declère A, Cariou A, Duranteau J, Aout M, Vicaut E, Cholley BP. Comparison of two versions of the Vigileo-Ò system (1.03 and 1.07) for stroke volume estimation: a multicentre, blinded comparison with oesophageal Doppler measurements. Br J Anaesth. 2009;102: 463–9. Cardiovasc Eng Cremer J, Martin M, Redl H, Bahrami S, Abraham C, Graeter T, Haverich A, Schlag G, Hans-Beorg B. Systemic inflammatory response syndrome after cardiac operations. Ann Thorac Surg. 1996;61:1714–20. Dark PM, Singer M. The validity of trans-esophageal Doppler ultrasonography as a measure of cardiac output in critically ill adults. Intensive Care Med. 2004;30:2060–6. DiCorte CJ, Latham P, Greilich PE, Cooley MV, Grayburn PA, Jessen ME. Esophageal Doppler monitor determinations of cardiac output and preload during cardiac operations. Ann Thorac Surg. 2000;69(6):1782–6. Dodd TEL. Nasal insertion of the oesophageal Doppler probe. Anaesthesia. 2002;57(4):412. Domino KB, Bowdle TA, Posner KL, Spitellie PH, Lee LA, Cheney FW. Injuries and liability related to central vascular catheters: a closed claims analysis. Anesthesiology. 2004;100(6):1411–8. Drazner MH, Rame JE, Stevenson LW, Dries DL. Prognostic importance of elevated jugular venous pressure and a third heart sound in patients with heart failure. NEJM. 2001;345(8):574–81. Hawkins DL. Using U-statistics to derive the asymptotic distribution of Fisher’s Z statistic. Am Stat. 1989;43:235–7. Ho AMH, Dion PW, Karmaker MK, Jenkins CR. Accuracy of central venous pressure monitoring during simultaneous continuous infusion through the same catheter. Anaesthesia. 2005;60(10): 1027–30. Imhoff M, Lehner JH, Dietrich Löhlein D. Noninvasive whole-body electrical bioimpedance cardiac output and invasive thermodilution cardiac output in high-risk surgical patients. Crit Care Med. 2000;28:2812–8. Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA, Hochman JS. Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. Arch Intern Med. 2005;165:1643–50. Kreyszig E. Advanced engineering mathematics. 8th ed. New York: Wiley; 1999. Kutner MH, Nachtsheim CJ, Neter J. Applied linear regression models. 4th ed. Chicago: McGraw-Hill; 2004. Li JK-J. The arterial circulation. Physical principles and clinical applications. Totowa: Humana Press; 2000. Li JK-J. Dynamics of the vascular system. Singapore: World Scientific; 2004. Madan AK, UyBarreta VV, Aliabadi-Wahle S, Jesperson R, Hartz RS, Flint LM, Steinberg SM. Esophageal Doppler ultrasound monitor versus pulmonary artery catheter in the hemodynamic management of critically ill surgical patients. J Trauma Injury Infect Critic Care. 1999;46(4):607–11. Magder S. How to use central venous pressure measurements. Curr Opin Crit Care. 2005;11(3):264–70. Manecke GR. EdwardsÒ sensor and VigileoÒ monitor: easy, accurate, reliable cardiac output assessment using the arterial pulse wave. Expert Rev Med Devices. 2005;2(5):523–7. Melo J, Peters JI. Low systemic vascular resistance: differential diagnosis and outcome. Crit Care. 1999;3:71–7. National Heart, Lung, and Blood Institute (NHLBI). Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Pulmonary artery versus central venous catheter to guide treatment of acute lung injury. NEJM. 2006;354(21):2213–23. Nichols W, O’Rourke M. Vascular impedance. In: McDonald’s blood flow in arteries. Theoretical, experimental and clinical principles. 5th ed. London: Hodder Arnold, Oxford University Press; 2005. pp. 233–67. Ouzounian JG, Masaki DI, Abboud TK, Greenspoon JS. Systemic vascular resistance index determined by thoracic electrical bioimpedance predicts the risk for maternal hypotension during regional anesthesia for cesarean delivery. Am J Obstet Gynecol. 1996;174(3):1019–25. Richards MJ, Edwards JR, Culver DH, Gaynes RP. The National Nosocomial Infections Surveillance System. Nosocomial infections in combined medical and surgical intensive care units in the United States. Infect Control Hosp Epidemiol. 2000;21:510–5. Sandham JD, Hull RD, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. NEJM. 2003;348(1):5–14. Segers P, Rietzschel ER, De Buyzere ML, Vermeersch SJ, De Bacquer D, Van Bortel LM, De Backer G, Gillebert TC, Verdonck PR. Noninvasive (Input) impedance, pulse wave velocity, and wave reflection in healthy middle-aged men and women. Hypertension. 2007;49(6):1248–55. Senni M, Tribouilloy CM, Rodeheffer RJ, Jacobsen SJ, Evans JM, Bailey KR, Redfield MM. Congestive heart failure in the community: a study of all incident cases in Olmsted county, Minnesota, in 1991. Circulation. 1998;98:2282–9. Simon R, Desebbe O, Henaine R, Bastien O, Lehot JJ, Cannesson M. Comparison of ICG thoracic bioimpedance cardiac output monitoring system in patients undergoing cardiac surgery with pulmonary artery cardiac output measurements. [French (English abstract)] Annales Françaises d’Anesthésie et de Réanimation. 2009;28(6):537–41. Singer M, Clarke J, Bennett ED. Continuous hemodynamic monitoring by esophageal Doppler. Crit Care Med. 1989;17:447–52. Soliman DE, Maslow AD, Bokesch PM, Strafford M, Karlin L, Marx GR. Transoesophageal echocardiography during scoliosis repair: comparison with CVP monitoring. Can J Anaesth. 1998;45(10): 925–32. Stewart RD, Psyhojos T, Lahey SJ, Levitsky S, Campos CT. Central venous catheter use in low-risk coronary artery bypass grafting. Ann Thorac Surg. 1998;66(4):1306–11. Valtier B, Cholley BP, Belot JP, de la Coussaye JE, Mateo J, Payen D. Noninvasive monitoring of cardiac output in critically ill patients using transesophageal Doppler. Am J Respir Crit Care Med. 1998;158:77–83. Wang GY, Ma B, Tang HT, Zhu SH, Lu J, Wei W, Ge SD, Xia ZF. Esophageal echo-Doppler monitoring in burn shock resuscitation: are hemodynamic variables the critical standard guiding fluid therapy? J Trauma. 2008;65:1396–401. Warzawski RC, Deye AN, et al. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trail. JAMA. 2003;290(20):2713–20. 123