Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
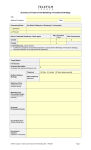
CREDIT ACCOUNT APPLICATION FORM PRIVATE & CONFIDENTIAL We …………………………………………… (hereafter called the Distributor) apply for Credit Facilities with High Chem Essentials Ltd (hereinafter called the Supplier) and agree to the following conditions: 1. That the Supplier may apply to our Bankers or the Traders for reference and this application is therefore signed by our Authorized Bank Signatories. 2. That all accounts are due for payment 30 days after issue of invoice unless otherwise agreed in writing. 3. That should the Distributor fail to observe the terms granted by the Supplier, our credit facilities will immediately be withdrawn and only reinstated at the Supplier’s sole discretion. 4. That the Distributor agrees to pay charges on overdue balances at the rate of 2% per month. 5. That the Distributor agrees to pay all and any legal charges that may result form the Supplier having to take legal action to recover any debt due to the Supplier. 6. In the event of any account being handed over to Solicitors, after settlement, all subsequent transaction shall be for cash or guaranteed Bankers Cheque only. 7. The Distributor agrees to supply all information on the attached form as follows: Name: ………………………………. Name: ………………………………. Signature: ……………………………. Signature: …………………………….. Designation: …………………………. Designation: …………………………. Date of Application: ……………………………………………….. Please note that the granting of credit is purely at the Supplier’s discretion. All details must be completed or the application may not be considered. 8) Bankers: Name _________________ _________________ _________________ _________________ Account No. __________________ __________________ __________________ __________________ Address ______________ ______________ ______________ ______________ Tel. No. Physical Address _________________ ______________ _________________ ______________ __________________ __________________ ______________ ______________ b) Name Tel. No. Physical Address __________________ __________________ ______________ ______________ 9) Branch ______________ ______________ ______________ ______________ Trade Reference: a) Name Postal Address Postal Address _________________ ______________ _________________ ______________ 10) What value of credit do you anticipate requiring on monthly basis? Kshs. ____________________________________________________________________ Yours sincerely, ________________________ AUTHORISED SIGNATURE DISTRIBUTOR’S COMPANY NAME: ____________________________________________ ADDRESS: __________________________________________________________________ RUBBER STAMP: ____________________________________________________________ 11. DISTRIBUTOR INFORMATION: a. Name of Company: __________________________________________________________ b. Type of Company (Private/Public/Unlimited) _____________________________________ c. Date of incorporation: ____________________ d. Incorporation No. ___________________ e. Postal Address: _____________________________________________________________ f. Email Address: _____________________________________________________________ g. Physical Address of Company: ________________________________________________ h. Name of Managing Person: ___________________________________________________ i. Designation: _______________________________________________________________ j. Telephone Numbers: _________________________________________________________ k. Associated / Subsidiary Companies: NAME: ADDRESS: ________________________________ ___________________________________ ________________________________ ___________________________________ l. DIRECTORS’ NAMES NATIONALITY ADDRESS ______________________ ___________________ ______________________ ______________________ ___________________ ______________________ m. Issued and paid up capital as per current Balance Sheet, ____________________________ n. What Business Activity are you engaged in? _____________________________________ o. Number of Employees _______________________________________________________ p. Number of years in Business __________________________________________________ q. Details of Insurance Cover over stock i.e. Cover issued by __________________________ __________________________________________________________________________ Insurance Cover value _______________________________________________________ Insurance Cover valid up to ___________________________________________________ 12. PERSONAL GUARANTEE: By signing the agreement constituted herein, the Director’s guarantee that if the distributor defaults in payment of the monies due to HighChem Veterinary Ltd, they shall be personally and severally liable to pay HighChem Veterinary Ltd as if they were the principal debtor. Dated this _____________________________ day of _______________________ , 2003 Signature ______________________________ Signature __________________________ Name _________________________________ Name _____________________________ Designation ____________________________ Designation ________________________ Company Rubber Stamp: ________________________________________________________ 13. SUPPLIER COMMITMENTS: 1. To supply all products in schedule 1 and to update this schedule to the Distributor regularly as the portfolios changes from time to time. 2. To supply a price structure for all our products in schedule 1. 3. Protect the Distributor against unfair competition in his region of operation. 4. To promote all marketing activities that relate to increased business in the area of Distributor operations. 14. DISTRIBUTOR COMMITMENTS: 1. To provide all information that may impede on the business here entered into. 2. To put under confidential cover any matters relating to business that is not of public consumption. 3. To use all within the Distributor’s control to promote the products in the area of operation. 4. To maintain professionalism in all matters of sales, distribution and marketing within the laws that govern the Kenyan Agricultural business. 15. FOR OFFICIAL USE ONLY: Recommendation Remarks: _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ Application approved for a limit of Kshs. ____________________________________________ Application Recommended by: ____________________________________________________ Approving Authority: ________________________________ Signature: __________________ Date: ________________________________________________________________________