Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
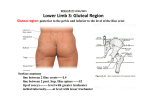
Anatomy Quiz: Week 38 4/22/2013 3:25:00 PM 1. Describe and demonstrate the bony landmarks of the pelvis on an articulated pelvis and on a plain film x-ray. Compare and contrast the shape of the female bony pelvis with that of the typical male bony pelvis. I’m imagining that the following bony landmarks are eligible (from his list): Iliac fossae Iliopubic eminence Arcuate line Pectineal line Superior pubic ramus Public symphysis Pubic arch Ischiopubic ramus Obturator foramen Ischial tuberosity Ischial spine Sacral promontory Anterior sacral foramina Coccyx I tried making a diagram and then I remembered that you all have books too. 2. Demonstrate the boundary structures and content of the urogenital and anal triangles on the bony pelvis. Urogenital Δ Boundaries: the vertices of the triangle are at the public symphysis and the two ischiopubic rami. It is the anterior triangle of the perineum. Contents: o Bulbospongiosus, ischiocavernosus, transversus perinei superficialis mm. o Crus of penis/ clitoral crura o Urethra o Bulbourethral gland (male)/ Bartolin’s gland (female) o Penis bulb, (yup) / vestibular bulb o Posterior scrotal or labial nerves Anal Δ Boundaries: the vertices are at the coccyx and the two ischiopubic rami. Posterior triangle of the perineum Contents: o Sacrospinous & sacrotuberous ligaments o Pudendal nerve o Internal pudendal a/v o Anal canal o Muscles Sphincter ani externus Gluteus maximus Obturator internus Levator ani Coccygeus o Ischioanal fossa 3. Describe the boundaries of the ischiorectal fossa from a posterior approach and describe the construction, attachments and functions of the components of levator ani in a female. The ischiorectal fossae are fat-filled, wedge-shaped, fascia-lined spaces between the pelvis diaphragm and the perianal skin. The boundaries are: Laterally; ischium, inferior obturator internus m., obturator fascia Medially; external anal sphincter, levator ani m. Posteriorly; sacrotuberous ligament, gluteus maximus Anteriorly; pubic bodies, inferior to the origin of puborectalis. The female levator ani muscle Puborectalis o Forms the sling for the rectum o Originates from inferior public symphysis and insert on the opposing puborectalis muscle o It lets you hold in a load when it might not be socially acceptable to dump it (wait, girls poop?) o N: S3, S4 Pubococcygeus o Hammock-shaped muscle from pubis to coccyx and forms the floor of the pelvic cavity o Joins iliococcygeus in forming the anococcygeal raphe o Controls urine flow, aids in childbirth, contracts during orgasm o N: S3, S4 Iliococcygeus o The most posterior of the group, from the ischial spine to the anococcygeus raphe, via the tendinous arch of the obturator fascia o Pulls the coccyx side to side and elevates the rectum o N: S3, S4 4. Describe the spermatic cord fascial layers including their embryological origin from the anterior abdominal wall structures. 3 Layers External Spermatic Fascia o derived from external oblique muscle o outermost covering of spermatic cord (& testes) Cremasteric Fascia o derived from internal oblique muscle Internal Spermatic Fascia o derived from transversalis fascia 5. Contrast and compare the arrangement of erectile tissue in the male and female genitalia. Male: 3 cylindrical cavernous bodies Paired corpora cavernosa dorsally Single corpus spongiosum ventrally The anatomical position for the penis is while erect. So dorsal is the side that’s easiest for his owner to view. Female: way more complicated than previously thought… Clitoris o At the anterior juncture of labia minora o Composed of two crura, two corpora cavernosa, and glans Glans is highly innervated Crura attach the clitoris to the inferior pubic rami Body of clitoris is covered by prepuce Bulbs of the Vestibule o Paired elongated masses of erectile tissue along the vaginal orifice, deep to the labia minora. o Homologous to the male’s bulb of the penis And, in conclusion, I present these schematics. Way more similar that I imagined. Gravy. 6. Compare and contrast the course of the urethra in the male and the female. Male (18-22cm) 1. Intramural / Preprostatic 1.5cm, vertically from the bladder, size depends on bladder status 2. Prostatic 3-4cm, descends through anterior prostate, very distensible 3. Intermediate (membranous) 1.0-1.5cm, through deep perineal pouch 4. Spongy Through the corpus spongiosum and out into the external environment Length doesn’t matter, right? Female (4cm long) From the internal urethral orifice of bladder, descends posterior to the pubic symphysis and then inferior to it, to the external urethral orifice. This is located in the vestibule of the vagina. 7. Trace the fascial layers of the abdomen as they descend into the pelvis. Anatomy Quiz: Week 39 4/22/2013 3:25:00 PM Compare and contrast the contours of the peritoneal lining of the pelvic cavity in the male and the female The pelvic peritoneum is thought to begin at the superior border of the pubic symphysis. In the male, in the black and green picture, the pelvic peritoneum continues posteriorly, covering the bladder and forming a broad retrovesical pouch between the bladder and the rectum. It will cover the rectum as it sweeps superiorly to meet the abdominal parietal peritoneum at S3. In the female, the peritoneum has to account for much more internal genitalia than the male. So, instead of going from bladder to rectum in the male, we go from bladder to uterus to rectum, (anterior to posterior). There will be two pouches: the uterovesical pouch (between 4 & 3 above) and the rectouterine pouch (pouch of Douglas). The uterovesical pouch is accessible by the anterior fornix of the vagina. The pouch of Douglas, or cul-de-sac, is accessible by the posterior fornix and from this location a procedure called a culdoscentesis may be performed to collect intraperitoneal fluids. Describe the arrangement of the internal female reproductive organs in the pelvic cavity, including the morphological changes that occur with pregnancy The vaginal canal, which is oriented superiorly and posteriorly, begins with the vestibule of the vagina and ends at the external os of the cervix. The uterus itself is most commonly flopped anteriorly onto the superior vesical surface. Other uterine orientations are possible. Most commonly, the angle of the vaginal canal is 45° to the angle of the uterus. Anteflexion: the long axis of uterus is bent anteriorly relative to that of the cervix Anteversion: the long axis of the cervix is bent anteriorly relative to that of the vagina (see pic) The cervix has length of a few and will terminate at the internal os. The uterus is next, which continues in whichever direction it decided to go (retro/anteflexed) to the fundus. At the fundus, the lumen of the uterus is continuous with the fallopian tubes, ending in the fimbriae. In pregnancy, the expanding 9 month intrauterine growth will push the fundus of the uterus superiorly with the head under the sacral promontory and the feet up past the belly button. In the case of retroflexed uterus, the baby’s orientation must be manipulated to avoid a feet first delivery. Describe the arrangement of the internal male reproductive organs in the pelvic cavity Internally, there are some extra things to your common knowledge of penises and balls. First, the ductus deferens. Beginning at the tail of the epididymis, the duct enters the abdomen by the inguinal canal and the pelvis by crossing over the external iliac vessels. It then travels along the lateral wall of the pelvis and ends by joining the seminal gland to form the ejaculatory duct. In the picture below, it’s the green tube coming from the scrotum. Superior to the prostate and posterior to the fundus of the bladder, we have the seminal glands. They are also closely related to the anterior wall of the rectum. The duct of these glands join the ductus deferens to form the proper ejaculatory duct. The ejaculatory ducts are closely related now, as they travel through the posterior prostate. The ducts terminate into one prostatic urethra. Next, the Cowper’s, or bulbourethral glands. Lying posteriolateral to the postprostatic urethra and mainly embedded in the external anal sphincter muscle. The content of the glands are emptied through tiny apertures in the spongy urethra. . Describe the blood supply to the pelvic cavity provided by the internal iliac artery and compare and contrast the differences seen in this blood supply between males and females Anterior The anterior division supplies the pelvic viscera, along with some to thigh and butt regions. Their arrangement is variable. Obturator o Gives off nutrient branch to ilium o Before leaving pelvis, gives off pubic branch Anastomosis with pubic branch of inferior epigastric artery Inferior gluteal o Larger, terminal branch of anterior division o Leaves pelvis via greater sciatic foramen, under piriformis Umbilical artery o Along lateral pelvic wall, ascends the anterior abdomen to the umbilicus Inferior vesical (male) or vaginal (females) o To prostate (not females) o to vagina, anterior and posterior branches often found as a branch of the uterine artery Uterine o Female only, additional branch that dudes don’t sport The male homolog is the branch to ductus deferens o Gives off a small vaginal branch and larger ascending branch at the side of cervix Middle rectal Internal pudendal o Larger in males > females o Goes for a ride out the greater sciatic foramen, under the piriformis, passes around the ischial spine and re-enters the pelvis via the lesser sciatic foramen to the ischioanal fossae o Within the fossae, the artery divides into the perineal artery and the dorsal artery of the penis/clitoris Posterior Iliolumbar o This shoots right back up to the iliac fossa and divides into an iliac branch (iliacus & ilium) and a lumbar branch (QL & psoas) Lateral sacral o Pass medially and descend, giving off spinal branches through the anterior sacral foramina to supply the sacral meninges o Some contribution to skin and erector spinae muscles Superior gluteal o Muscle to dem glutes Outline the course of lymphatic flow from the organs of the pelvic cavity; contrast the flow of lymph from the female and male pelvic cavities The word on the street is that the lymphatics for any region of the pelvis/perineum will follow the venous drainage…EXCEPT for the gonads. So, below you can see a number of regions highlighted that are named for the venous flow that the lymph nodes are associated with. The male pelvic viscera, (ejaculatory ducts, ductus deferens, inferior parts of seminal glands drain to the external iliac nodes. The prostate and superior seminal regions drain to the internal iliac. The ‘tip’ goes to the deep inguinal. The female, as always, is complicated. Ovaries drain to the lumbar lymph nodes, aka the caval/aortic nodes. Same with the fundus and upper uterine body. The uterine tubes and round ligament will drain to the superficial inguinal nodes. The uterine body and cervix will drain to the external iliac lymph nodes. Within the transverse cervical ligament, the uterine body will also drain to the internal iliac. Now the vagina has 3. Obv. Superior – internal and external iliac Middle – internal iliac Inferior – sacral, common iliac External – superficial inguinal nodes Describe the course of the somatic nerves (lumbosacral plexus) in the pelvic cavity Lumbar Iliohypogastric (L1) o Anterior to psoas major on lateral border to reach the anterior QL. There it pierces the transversus abdominis to run above the iliac crest, terminating near the inguinal ligament as an anterior cutaneous branch Ilioinguinal (L1) o Runs at the level of the iliac crest, after splitting from the iliohypogastric. Pierces lateral abdominal wall and runs above the inguinal ligament to the pubic symphysis Genitofemoral (L1, L2) o In the male, Lateral femoral cutaneous (posterior trunk) (L2, L3) Femoral (posterior trunk) (L2, L3, L4) Obturator (L2, L3, L4) Sacral Superior gluteal (L4-S1) o Above piriformis, leaves via greater sciatic foramen Inferior gluteal (L5-S2) o Below piriformis, leaves via greater sciatic forament Sciatic (L4-S3) o Large, forms and exits via greater sciatic foramen inferior to piriformis to the gluteal region Posterior femoral cutaneous (S2, S3) Nerve to QL (L4-S1) Nerve to Piriformis (S1, S2) Nerve to obturator internus (L5-S2) Perforating cutaneous (S2, S3) Pudendal S2-S4 o Via greater sciatic foramen, between piriformis and coccygeus muscles o Hooks around ischial spine, (like the artery) to enter the perineum via the lesser sciatic foramen o Branches to levator ani, external sphincter, coccygeus Coccygeal plexus S4-S5 anterior rami Arise on pelvic side of coccygeus muscle, supplying it, the levator ani and the sacrococcygeal joint Anococcygeal nerves arise from here and supply sensation from the skin between the tip of your coccyx and your anus