Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
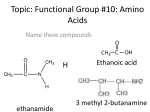
NME2.36: AMINO ACID AND PROTEIN METABOLISM 2 14/03/08 LEARNING OUTCOMES Explain the role of individual tissues in amino acid metabolism and changes in response to fasting, catabolic state and the fed state Amino acids can be categorised according to what their carbon skeletons can be converted to: o Glucogenic – from TCA cycle intermediates o Ketogenic – from acetyl-CoA o (Carbon dioxide is also produced) The majority of amino acids are glucogenic and most of the carbon yielded contributes to glucose o Leucine and lysine are ketogenic o Phenylalanine, tyrosine, threonine, tryptophan and isoleucine are both keto- and glucogenic Branched-chain amino acids (BCAAs) have non-linear aliphatic side-chains o These are leucine, isoleucine and valine o They can be used to generate energy by most tissues in the body – principally skeletal muscle B vitamins are generally essential cofactors in amino acid metabolism AMINO ACID METABOLISM IN DIFFERENT TISSUES The liver is the major site for amino acid metabolism o Only exceptions are BCAAs and alanine o High amino acid requirement for biosynthesis (plasma proteins, clotting factors etc.) o Primary site of non-essential amino acid synthesis Skeletal muscle is the major site for protein metabolism o Protein synthesis is increased following high protein meal o Muscle protein degradation provides amino acids during fasting o Oxidises BCAAs for energy releasing glutamine and alanine The gut utilises amino acids for fuel and protein synthesis o Intestinal mucosal cells use amino acids for energy in both fed and fasted states o Frequent turnover of mucosal cells requires a high rate of protein synthesis o Provided with amino acids for these vital functions at the expense of skeletal muscle The kidneys generate ammonia for excretion as urea o Glutamine reacts with water to yield ammonia catalysed by glutaminase Glutamine + H2O ↔ Glutamate + NH3 o Excretion of ammonia is used to dispose of protons in acidosis – glutamine usage increases o Glutamine is also used to generate energy CLINICAL ASPECTS Hypercatabolic states such as following surgery, trauma, burns etc. increase cortisol levels o Cortisol is the quintessential glucocorticoid that stimulates proteolysis and glycogen storage o Amino acids are released to provide energy and substrates for protein synthesis in healing o Since a lot of nitrogen is being produced there is often a negative nitrogen balance Discuss the benefits and potential problems associated with PKU treatment Phenylketonuria (PKU) is an autosomal recessive disorder affecting 1 in 10,000 o Single enzyme defect of phenylalanine hydroxylase o Inability to convert phenylalanine to tyrosine o Characterised by hyperphenylalaninaemia and presence of derivatives in the urine o Causes severe brain damage and mental retardation without treatment o Dietary restriction of phenylalanine only effective treatment Newborn screening for PKU was introduced in the UK in 1969 – the Guthrie test (heel prick) o ‘Heel prick’ during the first week of life o Samples applied to filter paper and sent to a laboratory o Blood analysed for phenylalanine levels Tyrosine becomes an essential amino acid in PKU so supplementation is necessary Life-long monitoring and restriction of phenylalanine intake is required QUESTIONS – PKU 1. What is the difference between congenital and inherited? Congenital describes a condition that is recognised at birth and could be due to genetic or environmental factors Inherited describes a condition that has been genetically determined 2. What might the nutritional consequence of phenylalanine hydroxylase deficiency be? Tyrosine deficiency, dietary restriction of phenylalanine and protein 3. Why is phenylpyruvate not normally excreted? Only unconverted phenylalanine goes on to form phenylpyruvate; normally it is all converted 4. What is the mechanism of the brain damage in untreated PKU babies? Amino acid transporters in the brain become saturated with phenylalanine inhibiting the uptake of other vital amino acids; excessively high amino acid levels also inhibit protein synthesis 5. What is the principle source of phenylalanine in the diet? Phenylalanine is found in meat, fish and dairy products as well as some carbonated drinks 6. Should the low phenylalanine diet be continued throughout life? Yes, though it is most crucial during the first 6 months of life 7. When and why might it be particularly important to maintain a strict diet in affected women? During pregnancy because the dangers posed to the developing foetus 8. What might be the effect of maternal PKU on the developing foetus? Congenital heart disease, growth and mental retardation