Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
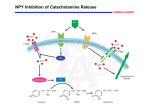
Clinical Science (2002) 103, 535–542 (Printed in Great Britain) Cardiovascular effects and cardiopulmonary plasma gradients following intravenous infusion of neuropeptide Y in humans: negative dromotropic effect on atrioventricular node conduction Bengt ULLMAN*, John PERNOW†, Jan M. LUNDBERG‡, Hans AH STRO= M§ and Lennart BERGFELDT† *Department of Cardiology, So$ der Hospital, SE-118 83 Stockholm, Sweden, †Department of Cardiology, Thoracic Clinics, Karolinska Hospital, Stockholm, Sweden, ‡Division of Pharmacology, Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden, and §Department of Clinical Physiology, Thoracic Clinics, Karolinska Hospital, Stockholm, Sweden A B S T R A C T Neuropeptide Y (NPY) is co-released with noradrenaline from sympathetic nerves, has a strong vasoconstrictive action, and causes an attenuation of parasympathetic action in animal experiments. The plasma level of NPY is greatly elevated in patients with congestive heart failure, but the clinical relevance of this finding is unclear. Central haemodynamic effects, cardiac conduction system electrophysiology and coronary sinus blood flow were therefore studied in two sets of experiments, each carried out on seven healthy men. In the first series, NPY was given intravenously at doses of 3, 10 and 30 pmol : min−1 : kg−1, and in the second it was given as a bolus injection of 90, 200 or 900 pmol/kg, which resulted in plasma concentrations similar to those seen in heart failure patients. During continuous infusion of NPY, systemic blood pressure increased slightly, but myocardial perfusion, cardiac output, pulmonary arterial pressure, cardiac conduction intervals and atrioventricular (AV) node functional measures remained unchanged. In contrast, the bolus injection of NPY evoked prolongation and block (in four out of seven subjects) of AV node conduction, but did not affect haemodynamic variables, apart from a minor increase in systemic blood pressure. Impaired AV node conduction is a novel observation, which might reflect a baroreceptor-mediated vagal reflex, or – more likely – an NPY-induced direct negative dromotropic effect, caused by a reduction of the L-type calcium current as observed in vitro, or a combination of the two. INTRODUCTION Neuropeptide Y (NPY) is co-released with the classical transmittor substance noradrenaline from sympathetic nerve terminals. Immunohistochemical studies have shown that NPY-immunoreactive fibres are present in high density in the mammalian heart and around blood vessels (especially arteries) [1]. The highest density is found around the coronary arteries, followed by the conduction system and the myocardium [1–3]. Systemic NPY infusions in the pig have revealed that certain regions, such as skeletal muscle, kidney and spleen, are very sensitive to NPY [4]. Furthermore, threshold vasoconstrictor effects in the human renal circulation are Key words : atrioventricular node, electrophysiology, haemodynamics, humans, neuropeptide Y. Abbreviations : AV, atrioventricular ; CHF, congestive heart failure ; CSBF, coronary sinus blood flow ; NPY, neuropeptide Y ; NPY-LI, NPY-like immunoreactivity ; PCV, pulmonary capillary venous. Correspondence : Dr Bengt Ullman (e-mail bengt.ullman!sos.sll.se). # 2002 The Biochemical Society and the Medical Research Society 535 536 B. Ullman and others obtained upon NPY infusion at plasma concentrations of approx. 260 pmol\l [5]. The vasoconstrictor effect of NPY potentiates α-adrenoceptor-mediated vasoconstriction in vitro [6], but is unaltered after α- and βadrenoceptor blockade [7,8]. NPY infusion into coronary arteries in the rabbit, guinea pig, dog and pig causes a sustained decrease in coronary perfusion [2,9–12]. Intracoronary NPY infusion in patients with angina pectoris without coronary stenosis produces transient myocardial ischaemia with typical ECG changes, decreased arterial blood pressure and bradycardia [13]. In addition to coronary vasoconstriction, NPY also inhibits vagal parasympathetic neurotransmission in the dog heart, as reflected by a decreased vagal-induced bradycardia [14]. More recent experimental studies show that relatively low concentrations of NPY have electrophysiological effects on the myocardium both in vitro [15] and in vivo [16], but the potential synergistic effects of noradrenaline and its co-transmittor NPY on electrophysiological function under pathological conditions have been little studied [17]. Plasma NPY-like immunoreactivity (NPY-LI) is elevated in humans during sympathetic activation, such as heavy physical exercise [18,19], and in patients with acute myocardial infarction [20]. Severe congestive heart failure (CHF) is associated with markedly elevated (up to 2000 pmol\l) plasma levels of NPY-LI [21,22]. It is not clear, however, whether this is of clinical relevance, or just an epiphenomen. The aim of the present study was therefore to evaluate whether doses of exogenous NPY that result in plasma levels found in patients with CHF have any pharmacological effects on central haemodynamics, myocardial blood flow or cardiac electrophysiology (the conduction system) in healthy men. In addition, we wanted to determine the possible clearance of NPY over the pulmonary and coronary vascular beds. METHODS Subjects This study was performed as two separate sets of experiments on a total of 14 healthy male volunteers. Their mean age was 28 years (range 23–35 years), height 180 cm (range 170–187 cm), and weight 79 kg (range 65–92 kg). They were all non-smokers and were not on any medication. They were fully informed about the procedures. The study protocol was approved by the Ethics Committee of the Karolinska Hospital. Catheterization and cardiovascular measurements All catheterizations were performed in the morning with the subject non-sedated and fasting. No tea or coffee was ingested during a period of 12 h prior to the study. # 2002 The Biochemical Society and the Medical Research Society A thermodilution catheter was inserted percutaneously via a medial cubital vein and advanced into the coronary sinus. The position of the tip of the catheter was verified by injection of contrast medium. Teflon catheters were inserted percutaneously into the brachial artery and the femoral vein. A 7F Swan-Ganz catheter was inserted through the femoral vein and advanced to the pulmonary artery. The pulmonary and brachial arterial catheters were connected to electromechanical transducers (Siemens-Elema, EMT 34). The pressures were recorded on a Mingograph (Sicor) and processed in a computer. The mid-thoracic level was used as the zero reference for pressures. Cardiac output was measured according to the Fick principle. Stroke volume was calculated from cardiac output and heart rate. Pulmonary capillary venous (PCV) pressure could not be obtained in two patients, for whom PCV pressure was substituted by diastolic pulmonary artery pressure. Blood samples for measurements of oxygen saturation were drawn from the pulmonary artery, the brachial artery and the coronary sinus. Coronary sinus blood flow (CSBF) was measured by the continuous thermodilution technique [23] using isotonic saline at room temperature. The flow was calculated using computerized on-line integration of the temperature curve. The mean value of three measurements was used. Myocardial oxygen consumption was calculated according to the Fick principle from CSBF and the oxygen difference between arterial and coronary sinus blood. Two 6F quadripolar electrode catheters (USCI) were introduced through the right femoral vein using 10-cm, 7F introductory sets. One catheter was positioned high on the lateral wall in the right atrium for pacing and recording, and one was positioned over the tricuspid valve in the His bundle position for recording of the low right atrial activity and His bundle potential. Right atrial pacing was performed with a current that was 2–4 times the diastolic threshold. The following electrophysiological variables were assessed, with estimated detection levels of interventions within parentheses [24] : intra-atrial conduction time (PA interval ; 15 %) ; atrioventricular (AV) node conduction time (AH interval ; 10 %) ; His-Purkinje conduction time (HV interval ; 15 %) ; Wenckebach cycle length ( 10 %) ; effective refractory period of the AV node ( 20 %), intraventricular depolarization and conduction time (QRS interval; 10 %) ; and intraventricular depolarization, conduction and repolarization time [QT interval, which was heart rate corrected according to Bazett (QTc l QT\NRR), in s (5 %)]. Surface ECG leads I, II, V1, V2 and V6 were recorded together with intracardiac signals on a multi-channel ink jet recorder (SiemensElema, Solna, Sweden) at a paper speed of 100 mm\s. All conduction intervals were measured by an experienced technician on a digitizer table working in point mode with a resolution of 10 lines\mm and an accuracy Cardiovascular effects of neuropeptide Y in humans During the infusion of the low dose of NPY (3 pmol : min−" : kg−"), only blood samples for determination of clearance were collected, whereas haemodynamic and electrophysiological variables were determined during infusion of the two higher doses. Pacing was stopped for 10 min during each NPY infusion for the assessment of the conduction intervals at a spontaneous rate, and the evaluation of AV node function. At the end of the last infusion, atropine was given intravenously (0.04 mg\kg) in order to evaluate the influence of NPY on vagal tone. The study protocol is shown in Figure 1 (upper panel). In the second part of the study, NPY was given as bolus injections into the femoral vein at doses of 90, 200 and 900 pmol\kg. Blood samples for analysis of NPY-LI in the femoral vein were drawn at 0, 1, 2, 5 and 10 min after each injection. The study protocol is shown in Figure 1 (lower panel). In this part of the study, neither cardiac output nor pulmonary arterial pressure were determined. Figure 1 Study protocols for the continuous infusion (upper panel) and bolus injection (lower panel) of NPY ‘ Time ’ is the time (min) in relation to the start of the first infusion/injection ; NPY inf 3, 10 and 30 represent NPY infusion at 3, 10, and 30 pmol : min−1 : kg−1 ; NPY bolus 1, 2 and 3 represent bolus injections of 90, 200, and 900 pmol/kg. A, intravenous injection of atropine (0.04 mg/kg) ; RAP, right atrial pacing ; H, haemodynamic measurement ; E (EPS), electrophysiological study. The time points at which blood samples were taken are indicated by arrows. of p0.635 mm (Calcomp 2000 ; Digitizer Products Division). The average of at least three intervals was calculated. The Wenckebach cycle length was determined by incremental atrial pacing from just above the basic rate. The effective refractory period of the AV node was determined by the extrastimulus (S1S2) technique after 8beat trains of regular atrial pacing at 100 beats\min with an accuracy of 10 ms. Synthetic human NPY was dissolved in saline containing 0.5 % human albumin and sterile filtered through a Millipore filter prior to infusion. NPY was administered as a continuous infusion at three different concentrations in seven men, and as bolus injections at three different doses in a separate group of seven men. Experimental protocols Following catheterization, the subjects were allowed to rest in the supine position for 30 min. Pressures in the brachial artery, pulmonary artery and PCV were measured, and cardiac output and CSBF were determined. Blood samples from the brachial artery, pulmonary artery and coronary sinus were drawn simultaneously. Right atrial pacing was started at 100 beats\min to assure a constant heart rate. In the first part of the study, NPY was infused into the femoral vein at a constant rate of 1 ml\min for 20 min at three different doses (3, 10 and 30 pmol : min−" : kg−"). Analysis of plasma NPY-LI Blood samples were collected in parallel from the brachial artery, pulmonary artery and coronary sinus during protocol 1, and from the femoral vein during protocol 2. The blood samples were put into pre-chilled heparinized tubes. The samples were placed in an ice bath and centrifuged at 3000 rev.\min for 10 min at 4 mC. Plasma was frozen at k70 mC until assayed for NPY-LI (within 2 months). Plasma NPY-LI was determined by RIA after extraction with acid ethanol. "#&I-labelled human NPY was used as a tracer and synthetic human NPY as the standard [25]. HPLC characterization of human plasma in connection with stress (physical exercise) [19] or NPY infusion [26] has revealed that one main peak corresponding to NPY-(1–36) is recognized by the antiserum. This has also been substantiated by recent characterization of the N-1 antiserum, showing that it does not cross-react with NPY fragments comprising residues 1–21, 16–36 or 26–36 to any significant extent ( 0.1 %). An even higher cross-reactivity (136 %) is observed for NPY-(2–36) than for NPY-(1–36), however. The stability of NPY in samples handled according to this protocol is well documented [25]. The limit of detection for plasma NPY-LI was 10 pmol\l using 0.5 ml of plasma. The coefficient of variation between duplicate samples in the same assay is 7 % for concentrations below 200 pmol\l. Statistical methods Variables are presented as meanspS.E.M. Statistical analyses were performed by ANOVA for repeated measurements. A probability level of P 0.05 was regarded as statistically significant. # 2002 The Biochemical Society and the Medical Research Society 537 538 B. Ullman and others RESULTS Continuous infusion – protocol 1 Baseline cardiac index and CSBF increased, while stroke volume decreased slightly, during right atrial pacing (Table 1). Arterial and pulmonary artery pressures remained unchanged. During NPY infusion, mean arterial blood pressure increased slightly, but this was not statistically significant. Oxygen consumption, cardiac index, pulmonary artery pressure, PCV pressure and total systemic resistance did not change. Mean CSBF and myocardial oxygen consumption were higher during NPY infusion, but these changes were not significant (Table 1). The spontaneous heart rate remained unchanged. The conduction interval, the Wenckebach cycle length and the effective refractory period of the AV node did not change during NPY infusion (Table 2). After the atropine injection, mean heart rate increased from 67 to 126 beats\min (Figure 2). The plasma levels of NPY-LI in the brachial artery, pulmonary artery and coronary sinus are shown in Figure 3. At baseline, the plasma NPY-LI level was 35p7 pmol\l in the pulmonary artery, 48p10 pmol\l in the brachial artery and 38p6 pmol\l in the coronary sinus. During the first, second and third infusions (3, 10 and 30 pmol : min−" : kg−"), plasma NPY was elevated 6fold, 20-fold and 60-fold respectively. At baseline before atrial pacing the mean plasma NPY-LI level was somewhat higher in the coronary sinus (55p15 pmol\l) than in arterial blood (32p4 pmol\l), but the difference was not significant (P l 0.06). During the first and second NPY infusions, mean plasma NPY-LI was higher (27 %) in arterial blood than in blood from the coronary sinus, while at the highest NPY dose no significant difference was found. Mean plasma NPY-LI was higher in systemic Table 1 Table 2 Results from electrophysiological studies in seven healthy men before and during intravenous infusion of NPY at 10 pmol : min−1 : kg−1 (NPY10) and 30 pmol : min−1 : kg−1 (NPY30) The conduction intervals were obtained during sinus rhythm. RR, ventricular cycle length ; PA, intra-atrial conduction time ; AH, AV node conduction time ; HV, HisPurkinje conduction time ; QRS, ventricular depolarization time ; QTc, ventricular depolarization and repolarization time corrected for heart rate (QTc l QT/NRR) ; Wb, stimulation interval at Wenckebach block in the AV node ; ERPAVN, effective refractory period of the AV node. No statistically significant differences compared with baseline were seen. Interval (ms) Variable Baseline NPY10 NPY30 RR PA AH HV QRS QTc Wb ERP-AVN 919p70 39p4 76p6 46p2 99p4 392p7 366p19 387p36 964p51 40p3 74p5 47p1 97p4 386p8 365p24 410p37 903p49 40p4 75p7 47p1 96p4 389p8 380p24 397p34 than in pulmonary arterial blood during infusion of all three doses, but a significant difference (25 %) was only found between the two lowest NPY doses (Figure 3). Bolus injection – protocol 2 After each injection of NPY (90, 200 and 900 pmol\kg), the greatest difference compared with baseline was noted 1 min after injection. The bolus injections of NPY resulted in a dose-dependent, statistically significant, increase in mean arterial blood pressure compared with Haemodynamics and CSBF in seven healthy men during continuous infusion of NPY HR, heart rate ; MAP, mean arterial blood pressure ; CI, cardiac index ; SV, stroke volume ; PPA, pulmonary artery pressure ; PCW, pulmonary capillary wedge pressure ; Rs,tot, total systemic resistance ; Rcor, coronary resistance ; RAP, right atrial pacing. NPY was infused over 10 min at 10 (NPY10) and 30 (NPY30) pmol : min−1 : kg−1. None of the differences between RAP and RAPjNPY10 or RAPjNPY30 are statistically significant. Parameter Baseline RAP RAPjNPY10 RAPjNPY30 HR (beats/min) MAP (mmHg) O2 consumption (ml/min) CI (litres : min−1 : kg−1) SV (ml) PPA (mmHg) PCW (mmHg) Rs,tot (mmHg : l−1 : min−1) CSBF (ml/min) Myocardial O2 consumption (ml/min) Rcor (mmHg : l−1 : min−1) 69p4 100p5 313p18 3.59p0.16 106p5 14p1 8p1 14p1 91.4p4 12.3p0.6 1.09p0.06 100p0 103p4 307p23 4.22p0.37 88p7 13p2 7p1 13p1 111p5 14.9p0.9 0.94p0.06 100p0 107p4 313p19 4.27p0.23 89p5 12p2 7p2 13p1 124p8 16.1p1.3 0.92p0.07 100p0 111p3 314p16 4.16p0.29 87p7 13p2 6p1 14p1 137p14 18.4p2.1 0.87p0.1 # 2002 The Biochemical Society and the Medical Research Society Cardiovascular effects of neuropeptide Y in humans Figure 2 Heart rate during intravenous infusion of NPY at 3 (NPY 3), 10 (NPY 10) and 30 (NPY 30) pmol : min−1 : kg−1 At the end of the last infusion, atropine (0.04 mg/kg) was given intravenously. Values are meanspS.E.M. Figure 3 Plasma NPY-LI levels in pulmonary arterial (PA), arterial (A) and coronary sinus (SC) blood during intravenous NPY infusion at 3, 10 and 30 pmol : min−1 : kg−1 Blood samples were drawn simultaneously during spontaneous sinus rhythm without pacing. Values are meanspS.E.M. Differences were calculated as PAkA and AkSC ; *P 0.05. Figure 4 ECG and arterial blood pressure recordings after intravenous bolus injection of NPY in one subject who developed a second-degree AV block other three only at the highest dose of NPY. Along the same lines, the mean AV node conduction time (the AH interval) was increased compared with baseline (Table 3). The His-ventricular conduction time (the HV interval), QRS and QT intervals were not altered after the NPY injections. The plasma NPY-LI level measured in femoral venous blood was dose-dependently elevated by the NPY injections (Table 3). There was a weak but significant correlation between the change in mean arterial blood pressure compared with baseline and the change in the mean AV node conduction time (Spearman non-parametric correlation test ; P 0.05 and R l 0.22). DISCUSSION baseline (Table 3). Four out of seven subjects developed second-degree AV block after the injections. All blocks occurred in the AV node and resulted in single blocked atrial impulses (Figure 4). One subject developed a second-degree AV block after each injection, and the During continuous infusion of NPY, mean arterial pressure increased, while other haemodynamic and electrophysiological variables remained unchanged. In contrast, bolus injections of NPY increased the mean AV Table 3 Arterial pressure, coronary resistance and electrophysiological variables after intravenous injection of NPY at three doses : 90 pmol/kg (1), 200 pmol/kg (2) and 900 pmol/kg (3) All values were obtained at right atrial pacing at 100 beats/min. MAP, mean arterial blood pressure ; Rcor, coronary resistance ; AH, AV node conduction time ; HV, His-Purkinje conduction time ; QT, intraventricular depolarization, conduction and repolarization time ; QS, intra-ventricular depolarization and conduction time. Time intervals (AH, HV, QT and QS) are given as a percentage of the baseline value. Significance of differences : *P 0.05, **P 0.01 compared with baseline. Parameter Baseline Dose 1 Dose 2 Dose 3 MAP (mmHg) Rcor (mmHg : l−1 : min−1) AH ( %) HV ( %) QT ( %) QS ( %) NPY-LI (pmol/l) 94p2 0.68p0.08 100p0 100p0 100p0 100p0 18p4 97p3 0.60p0.08 116p9* 100p2 101p1 102p1 291p72** 102p4 0.63p0.06 106p6 100p2 101p1 102p2 837p212** 104p6* 0.58p0.05 126p12* 102p3 101p1 101p2 3920p1950** # 2002 The Biochemical Society and the Medical Research Society 539 540 B. Ullman and others node conduction time and resulted in AV node block in four out of seven subjects, in addition to mildly increased mean arterial pressure. At plasma levels similar to those seen in patients with CHF, NPY thus had very modest haemodynamic effects, but significant electrophysiological effects, on the healthy human heart. Cardiovascular effects of NPY We have shown previously that patients with severe CHF have plasma NPY-LI values of up to 2000 pmol\l [21]. Similar levels have also been found in patients with hypertension [27]. This level (2000 pmol\l) was therefore chosen as a maximal target for the infusion studies, since the overall hypothesis was to test the haemodynamic and electrophysiological effects of NPY at observed clinical plasma levels. The only significant cardiovascular effect of the continuous NPY infusion was elevation of systemic blood pressure. This effect is probably due to peripheral vasoconstriction, since cardiac output was unchanged. In the second protocol, the same total amounts of NPY were administered as bolus injections in order to achieve even higher plasma concentrations of the peptide. The bolus injections evoked increases in arterial blood pressure, but did not significantly affect coronary blood flow or vascular resistance. The present human data are in accordance with findings in the pig, in which intravenous NPY infusion caused peripheral but no coronary vasoconstriction, at similar plasma levels of NPY-LI [12]. This observation suggests that circulating NPY at this plasma level does not regulate coronary blood flow in healthy men. However, the concentration of endogenous NPY that is close to its receptors after release from nerve terminals may be even higher. It may thus be difficult to relate circulating levels to interstitial concentrations of endogenous substances. However, the effect on AV node conduction, which was impaired, is a novel and unexpected observation, and has not been described previously after intravenous or intracoronary bolus injections in humans. The positive correlation between mean arterial blood pressure and AV node conduction time suggests that this might be a baroreceptor-mediated vagal reaction. However, the increase in blood pressure was minor, and apparently not sufficient to elicit a vagal reflex, which also would seem to contrast with the results of animal experiments, in which NPY had an inhibitory effect on cardiac vagal action. Another explanation, based on results from in vitro experiments in guinea pig cardiac myocytes and phaeochromocytoma cells, is offered [16,28,29]. According to these experiments, NPY inhibits L-type calcium channel activity through a mechanism that involves a G-proteinmediated pathway in guinea pig ventricular cardiomyocytes [16,28], and an intracellular Ca#+- and protein kinase C-dependent pathway in phaeochromocytoma cells [29]. As stated in the latter reference, both catecholamine synthesis and release is inhibited by NPY, # 2002 The Biochemical Society and the Medical Research Society probably via the activation of different NPY receptor subtypes and different calcium-ion channels. Thus, whereas the direct vascular effects of NPY generally are mediated via the Y receptor subtype, other receptors " such as the Y receptor may be involved in prejunctional # regulation of transmitter release. Taken together, in vitro data support the hypothesis that NPY actually regulates sympathetic neuronal function, according to these authors [29]. Since it is well known – and has been exploited therapeutically in clinical cardiology for many years – that inhibition of L-type calcium channel activity impairs AV node conduction, the experimental data above thus offer an alternative explanation for our results. The physiologically beneficial effect of such NPY modulation on catecholamine synthesis and release at the AV node level would apparently be to counteract any exaggerated sympathetic activity that would threaten the ventricles by resulting in too rapid conduction of atrial impulses and hence too frequent activation of the ventricles. Our observations are in contrast to those of some previous in vivo experiments, in which exogenous NPY in doses of 5–7 nmol\kg had no effect on cardiac conduction intervals in dogs, but the vagal effects on the sinus and AV nodes were attenuated [14,30]. Intravenous bolus injection of NPY at even higher doses (approximately 15 nmol\kg) into the femoral vein increased mean arterial pressure, reduced coronary blood flow and also inhibited the response to vagal stimulation in dogs [31]. When atropine was given after 20 min infusion of NPY at 30 pmol : min−" : kg−" in our study the average heart rate increased from 67 to 126 beats\min, which is not less than the expected response of approximately j46 to 60 % [32,33]. This finding together with the unaltered resting heart rate and AV node function, Table 2, Figure 3, suggests that NPY in doses according to our protocol 1 does not have any major effect on the cardiac cholinergic tone. This may not be surprising, however, since considerably higher doses of NPY were given in the above mentioned animal experiments, which demonstrated an inhibitory effect on vagal action. The absence of any detectable effect on cardiac electrophysiology in the healthy heart during continuous infusion does not exclude the possibility that the high circulating levels of NPY observed in patients with heart disease are of biological importance. First, the circulating plasma levels of endogenous NPY may not properly reflect the local concentration close to the receptor site at the neuro-effector junction. Secondly, the sensitivity to an agonist may differ between healthy and diseased tissue. Thus, when comparing the effects of the sodiumchannel blocking substances carbamazepine and disopyramide in healthy subjects and patients with cardiac disease, we found no or only mild effects in the healthy heart, but moderate to severe effects in the sick heart [34–36]. Cardiovascular effects of neuropeptide Y in humans Gradients of NPY between different compartments The concentration of NPY near the site of release is probably much higher than in venous plasma because of local degradation by peptidases [37], and the local concentration of NPY in the myocardium during severe heart failure is unknown. During intravenous administration of NPY, there is probably a lower interstitial concentration in the myocardium than in arterial plasma, as NPY is a relatively large peptide (Mr approx. 4200), resulting in a possible diffusion gradient into the myocardium during intravenous infusion. Earlier studies have shown net cardiac release of NPY in humans, especially upon exercise and hypoxia [38]. In accordance with previous observations, we found slightly higher plasma NPY-LI levels in coronary sinus than in arterial plasma before right atrial pacing and NPY infusion, but the difference was not significant (P l 0.06). The NPY-LI overflow from the heart is enhanced during sympathetic nerve stimulation in pigs [12] and dogs [39], suggesting release of NPY from the myocardium during sympathetic activation. Furthermore, one study has demonstrated that a portion of coronary constriction evoked by sympathetic nerve stimulation was resistant to adrenergic receptor blockade and correlated with the release of NPY [40]. Approx. 50 % of NPY is cleared over the splanchnic vascular bed during NPY infusion in humans [5], but possible clearance over the coronary circulation is unknown. During NPY infusion in the present study, the mean plasma NPY-LI level was lower in coronary sinus blood than in arterial blood at an infusion dose of 10 pmol : min−" : kg−", which indicates clearance of the peptide over the coronary vascular bed. At the highest dose no difference was found, possibly due to saturation of NPY degradation. Surprisingly, higher plasma levels were found in the brachial artery than in the pulmonary artery. This suggests production of NPY-LI in the lung. One possible explanation for this may be production of long NPY-like fragments [e.g. NPY-(3–36)], which can occur, at least in vitro [37]. Although this particular fragment was not available for testing, NPY-(2–36) has a higher cross-reactivity with the N-1 antiserum than NPY-(1–36). Therefore the higher levels of NPY-LI in systemic than in pulmonary arterial plasma may indicate production of NPY fragments in the pulmonary circulation, with high cross-reactivity to the antiserum used. Further analysis, e.g. by reverse-phase HPLC or gel-permeation chromatography, is necessary to test this hypothesis. Conclusions Continuous intravenous infusion of NPY into healthy men at doses resulting in plasma concentrations observed in patients with severe CHF increased systemic blood pressure, but did not significantly influence coronary blood flow or other haemodynamic variables. Neither was there evidence of any significant electrophysiological effect, nor of inhibition of cholinergic effects on the heart. In contrast, bolus injections impaired AV node conduction, possibly due to a NPY-induced reduction of the L-type calcium current. This novel finding suggests that NPY can have a modulating (counteractive) role in the sympathetic nervous system, at least in some tissues. Evidence for NPY-LI production in the lung was obtained during NPY infusion. The electrophysiological effect of NPY observed in the present study is intriguing, but it remains to be established, preferably by the use of a specific NPY antagonist, whether the high levels of NPY in heart failure patients have any pathophysiological effects. ACKNOWLEDGMENTS This study was supported by the Swedish Medical Research Council (10857, 14X-6554), the Swedish Heart Lung Foundation, the Swedish Society of Medicine, and the Karolinska Institutet. REFERENCES 1 2 3 4 5 6 7 8 9 Lundberg, J. M., Terenius, L., Ho$ kfelt, T. and Goldstein, M. (1983) High levels of neuropeptide Y in peripheral noradrenergic neurons in various mammals including man. Neurosci. Lett. 42, 167–172 Allen, J. M., Gjo$ rstrup, P., Bjo$ rkman, J.-A., Ek, L., Abrahamsson, T. and Bloom, S. R. (1986) Studies on cardiac distribution and function of neuropeptide Y. Acta Physiol. Scand. 126, 405–411 Gu, J., Polak, J. M., Adrian, T. E., Allen, J. M., Tatemoto, K. and Bloom, S. R. (1983) Neuropeptide tyrosine (NPY) – a major cardiac neuropeptide. Lancet ii, 1008–1010 Rudehill, A., Olce! n, M., Sollevi, A., Hamberger, B. and Lundberg, J. M. (1987) Release of neuropeptide Y upon haemorrhagic hypovolemia in relation to vasoconstrictor effects in the pig. Acta Physiol. Scand. 131, 517–523 Ahlborg, G., Weitzberg, E., Sollevi, A. and Lundberg, J. M. (1992) Splanchnic and renal vasoconstrictor and metabolic responses to neuropeptide Y infusion in resting and exercising man. Acta Physiol. Scand. 145, 139–149 Ekblad, E., Edvinsson, L., Wahlestedt, C., Uddman, R., Ha/ kanson, R. and Sundler, F. (1984) Neuropeptide Y coexists and co-operates with noradrenaline in perivascular nerve fibers. Regul. Pept. 8, 225–235 Lundberg, J. M. and Tatemoto, K. (1982) Pancreatic polypeptide family (APP, BPP, NPY and PPY) in relation to sympathetic vasoconstriction resistant to alpha-adrenoceptor blockade. Acta Physiol. Scand. 116, 393–402 Lundberg, J. M., Franco-Cereceda, A., Hemse! n, A., Lacroix, J. S. and Pernow, J. (1990) Pharmacology of noradrenaline and neuropeptide tyrosine (NPY)-mediated sympathetic co-transmission. Fund. Clin. Pharmacol. 4, 373–391 Allen, J. M., Bircham, P. M. M., Edwards, A. V., Tatemoto, K. and Bloom, S. R. (1983) Neuropeptide Y (NPY) reduces myocardial perfusion and inhibits the force of contraction of the isolated perfused rabbit heart. Regul. Pept. 6, 247–253 # 2002 The Biochemical Society and the Medical Research Society 541 542 B. Ullman and others 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 Franco-Cereceda, A., Lundberg, J. M. and Dahlo$ f, C. (1985) Neuropeptide Y and sympathetic control of heart contractility and coronary vascular tone. Acta Physiol. Scand. 124, 361–369 Komaru, T., Ashikawa, K., Kanatsuka, H., Sekiguchi, N., Suzuki, T. and Takishima, T. (1990) Neuropeptide Y modulates vasoconstriction in coronary microvessels in the beating canine heart. Circ. Res. 67, 1142–1151 Rudehill, A., Sollevi, A., Franco-Cereceda, A. and Lundberg, J. M. (1986) Neuropeptide Y (NPY) and the pig heart : Release and coronary vasoconstrictor effects. Peptides 7, 821–826 Clarke, J. G., Davies, G. J., Kerwin, R. et al. (1987) Coronary artery infusion of neuropeptide Y in patients with angina pectoris. Lancet i, 1057–1059 Potter, E. K. (1987) Cardiac vagal action and plasma levels of neuropeptide Y following intravenous injection in the dog. Neurosci. Lett. 77, 243–247 Kralios, F. A., Anderson, F. L., Hanson, G. R. and Kralios, A. C. (1995) Myocardial electrophysiologic effects of neuropeptide Y in dogs. Am. J. Physiol. 268, H2195–H2201 Bryant, S. M., Ryder, K. O. and Hart, G. (1991) Effects of neuropeptide Y on cell length and membrane currents in isolated guinea pig ventricular myocytes. Circ. Res. 69, 1106–1113 Du, X.-J. and Dart, A. M. (1999) Role of sympathoadrenergic mechanisms in arrhythmogenesis. Cardiovasc. Res. 43, 832–834 Lundberg, J. M., Martinsson, A., Hemse! n, A. et al. (1985) Co-release of neuropeptide Y and catecholamines during physical exercise in man. Biochem. Biophys. Res. Commun. 133, 30–36 Pernow, J., Lundberg, J. M., Kaijser, L. et al. (1986) Plasma neuropeptide Y-like immunoreactivity and catecholamines during various degrees of sympathetic activation in man. Clin. Physiol. 6, 561–578 Ullman, B., Franco-Cereceda, A., Hulting, J., Lundberg, J. M. and Sollevi, A. (1990) Elevation of plasma neuropeptide Y-like immunoreactivity and noradrenaline during myocardial ischaemia in man. J. Intern. Med. 228, 583–589 Hulting, J., Sollevi, A., Ullman, B., Franco-Cereceda, A. and Lundberg, J. M. (1990) Plasma neuropeptide Y on admission to a coronary care unit : raised levels in patients with left heart failure. Cardiovasc. Res. 24, 102–108 Maisel, A. S., Scott, N. A., Motulsky, H. J. et al. (1989) Elevation of plasma neuropeptide Y levels in congestive heart failure. Am. J. Med. 86, 43–48 Ganz, W., Tamura, K., Marcus, H. S., Donoso, R., Yoshida, S. and Swan, H. J. C. (1971) Measurement of coronary sinus blood flow by continuous thermodilution in man. Circulation 44, 181–195 Bergfeldt, L., Melander, H. and Schenck-Gustavsson, K. (1991) Time-dependent variation in the cardiac conduction system assessed in young healthy individuals at weeks’ interval : implications for clinical trials. J. Am. Coll. Cardiol. 18, 792–800 Theodorsson-Norheim, E., Hemse! n, A. and Lundberg, J. M. (1985) Radioimmunoassay for neuropeptide Y (NPY) : chromatographic characterization of immunoreactivity in plasma and tissue extracts. Scand. J. Clin. Lab. Invest. 45, 355–365 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 Pernow, J., Lundberg, J. M. and Kaijser, L. (1987) Vasoconstrictor effects in vivo and plasma disappearance rate of neuropeptide Y in man. Life Sci. 40, 47–54 Morris, M. J., Cox, H. S. and Lambert, G. W. (1997) Region-specific neuropeptide Y overflows at rest and during sympathetic activation in humans. Hypertension 29, 137–143 Bryant, S. M. and Hart, G. (1996) Effects of neuropeptide Y on L-type calcium current in guinea pig ventricular myocytes. Br. J. Pharmacol. 118, 1455–1460 McCullough, L. A., Egan, T. M. and Westfall, T. C. (1998) Neuropeptide Y inhibition of calcium channels in PC-12 pheochromocytoma cells. Am. J. Physiol. 274, C1290–C1297 Warner, M. R. and Levy, M. N. (1989) Inhibition of cardiac vagal effects by neurally released and exogenous neuropeptide Y. Circ. Res. 65, 1536–1546 Awad, S. J., Einstein, R., Potter, E. K. and Richardson, D. P. (1991) The effects of neuropeptide Y on myocardial contractility and coronary blood flow. Br. J. Pharmacol. 104, 195–201 Alboni, P., Malcarne, C., Pedroni, C., Masoni, A. and Narula, O. S. (1982) Electrophysiology of normal sinus node with and without autonomic blockade. Circulation 65, 1236–1242 Bergfeldt, L. Schenck-Gustavsson, K. and Dahlqvist, R. (1992) Comparative class 1 electrophysiologic and anticholinergic effects of disopyramide and its main metabolite (mono-N-dealkylated disopyramide) in healthy humans. Cardiovasc. Drugs Ther. 6, 529–537 Englund, A., Bergfeldt, L. and Rosenqvist, M. (1998) Pharmacological stress testing of the His-Purkinje system in patients with bifascicular block. PACE Pacing Clin. Electrophysiol. 21, 1979–1987 Kenneba$ ck, G., Bergfeldt, L., Vallin, H., Tomson, T. and Edhag, O. (1991) Electrophysiologic effects and clinical hazards of carbamazepine treatment for neurologic disorders in patients with abnormalities of the cardiac conduction system. Am. Heart J. 121, 1421–1429 Kenneba$ ck, G., Bergfeldt, L. and Tomson, T. (1995) Electrophysiological evaluation of the sodium-channel blocker carbamazepine in healthy human subjects. Cardiovasc. Drugs Ther. 9, 709–714 McDermott, J. R., Gibson, A. M., Boublik, J. and Biggins, J. A. (1992) Dipeptidylpeptidase IV initiates the degradation of neuropeptide Y in cardiac muscle membranes. Biochem. Soc. Trans. 4, 351S Kaijser, L., Pernow, J., Berglund, B. and Lundberg, J. M. (1990) Neuropeptide Y is released together with noradrenaline from the human heart during exercise and hypoxia. Clin. Physiol. 10, 179–188 Warner, M. R., Senanayake, P. D., Ferrario, C. M. and Levy, M. N. (1991) Sympathetic stimulation-evoked overflow of norepinephrine and neuropeptide Y from the heart. Circ. Res. 69, 455–465 Tanaka, E., Mori, H., Chujo, M., Yamakawa, A. and Minhaz, U. (1997) Coronary vasoconstrictive effects of neuropeptide Y and their modulation by the ATPsensitive potassium channel in anesthetized dogs. J. Am. Coll. Cardiol. 29, 1380–1389 Received 12 July 2002; accepted 13 August 2002 # 2002 The Biochemical Society and the Medical Research Society