Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
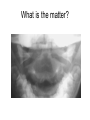
C- Spine Adult vs Pediatric Caroline Kowal C – spine views • • • • • AP Lateral Odontoid Swimmers: lower C - spine Oblique: posterior structures of vertebral column (e.g. intervertebral foramen and articular facet joints. R/O facet dislocation) • Lateral flexion/extension: exclude ligamentous injury and potential instability ABC’s • A – adequacy/alignment – Vertebral curves on lateral view – Dens equidistant from lateral masses of C1 • Facets of C1/C2 should align – AP – spinous processes should align • B – bones • Boney deformity or # lines – Ant/post height nearly equal – Pedicles, facets, spinous processes ABC’s Pediatric Emerg Med Reports 1996;1:83. • C – Cartilage – Disc spaces (symmetrical and similar) • S – Soft Tissue – Lateral view can tell you about occult fracture and rupture of transverse ligament – Predental space < 3mm (< 5 mm if <8 y.o.) – Prevertebral space at C3 < 5mm (< 7 mm kids or <1/3 width vertebral body) – Prevertebral space at C7 < 22mm (<14mm C6) • Lateral view to r/o retropharyngeal abcess • If true prevertebral swelling, increased space will persist despite neck positioning • No “step off” at C4 Optimal if pt neck extended (and x ray taken at END inspiration – less false +). Subglottic narrowing • Normally a "step-off" between the posterior wall of the pharynx and the posterior wall of the trachea at the level of the larynx (approximately at the level of C4). Retropharngeal Abcess • Air-soft tissue interface is indistinct • Contour of prevertebral soft tissues should follow anterior vertebrae • Retropharyngeal abscesses are the 2nd most common deep neck infections in children (first is peritonsillar abscesses which account for up to 50% of the deep neck infections) Neck alignment • Normally positioned with lordosis (extension). • In adults, a straight C-spine (lack of lordosis) indicates the presence of muscle spasm and a possible occult fracture. • In children, the absence of lordosis is commonly seen. • When on a spine board, the large occiput of most children positions their neck in a straight positoin. – This is common and does not necessarily indicate the presence of a significant injury. Nexus Criteria • According to NEXUS low-risk criteria, cervical spine radiography is indicated for trauma patients unless they exhibit all of the following criteria: • 1. No posterior midline cervical tenderness • 2. No evidence of intoxication (EtoH, ataxia, dysmetria, cerebellar findings) • 3. Normal level of alertness (GSC >14, A&O x3) • 4. No focal neurologic deficit • 5. No painful distracting injuries – long bone #, burn, degloving injury Canadian C – Spine Criteria • GCS 15 • High risk factors? – >65 years age – Dangerous mechanism – Paresthesias in extremities • Dangerous mechanism – Fall >1 m or 5 stairs, axial load, MVC >100km/h, rollover or ejection, bike collision • Low risk factors? – Simple rear end MVC, sitting position in ED, ambulatory at any time, delayed onset neck pain, no midline tenderness – If have low risk criteria and no high risk and can rotate neck 45 degrees with no pain – NO RADIOGRAPHS. Anatomy Review • 7 cervical vertebra C1 – C7 – C1, C2, and occiput are called the cervicocranium – C1 and C2 are atypical vertebrae – As many as 80-90% of cervical spine injuries can be detected on the lateral view alone. • Neural arch ( pedicles, laminae,spinous process, articular processes and facets, and transverse processes) – – – – structures dorsal to the vertebral body protect the spinal cord attachment sites for ligaments and muscles forms synovial joints that facilitate movement of the vertebral column. Ligaments SP - spinous process L - lamina (forms roof of the neural arch) P - pedicle (forms supports of the neural arch) SC - spinal canal VB - vertebral body SAF - superior articular facet IAF - inferior articular facet TF - transverse foramen Gr - groove for spinal nerve (transverse process) U - uncinate process Child vs. Teen Lateral View Lateral film, the body is a rhomboid with the posterior portion slightly taller than the anterior portion Cervical Lines • • • • Anterior longitudnal line Posterior longitudnal line Posterior facet margins Spinolaminal line – anterior border with the laminae – Posterior limits of spinal canal F - facet joint SP - spinous process L - lamina Od odontoid AP View On an AP view, the lateral superior edges of the body form bilateral ridges, called the uncinate processes (U). Fractures to the Unicate • Axial compression • Strong lateral force with shearing • Hyperflexion or hyperextension – Teardrop # to lateral vertebral bodies Spinous Process • Spinous processes of C3 through C6 are typically bifid at the tips • C7 is an easily visible surface landmark – vertebra prominens • Muscles attached – trapezius, the levator scapularis, and the rhomboids – Excessive load on these muscles may result in avulsion of the spinous processes of C6 and C7, commonly known as the clay shoveller's fracture Clay Shoveller’s Fracture Odontoid Views • To examine C1 – C2 complex – R/O fracture dens (ruptured transverse ligament) – Dens should be equidistant from lateral masses of C1 – Facets of C1 and C2 should align evenly – Sum of overhang of both sides should not be >7 mm Odontiod View 3 Types Odontoid Fractures • Type I is an oblique fracture through the upper portion of the odontoid. – The upper incisors can obscure portions of the upper odontoid and simulate a Type I fracture. • Type II fractures occur at the base of the odontoid where it joins the body of C2. – This is the most common odontoid fracture. Unfortunately, this is also the location of the subdental synchondrosis. • A Type III odontoid fracture extends into the vertebral body of C2 What type of odontoid # is this? Type 2 most common and most therapeutically challenging. In children the fracture breaks through the cartilage plate and heals spontaneously. Inadults due to disruption of blood supply, it may require surgery to heal. Type 1 and 3 generally heal spontaneously but in type 3 the prognosis is worse if the fracture extends into the articular facets. Type II Dens Fracture Subdental Synchondrosis • The most common normal radiographic pattern mistaken for an odontoid fracture. • A linear lucency at the base of the dens. • The dens usually fuses with the body of C2 between 3 and 6 years. – A thin, sclerotic "scar" of the synchondrosis may be appreciable on the lateral view for many years thereafter. CT image of a burst # of C1. Usually occurs with axial compression. C1 vulnerable to burst fractures because it is a ring of bone (no vertebral body). Horizontal Arrow indicates a growth plate. Child’s odontoid • The odontoid of children may have a separate ossification center at the tip of the odontoid--the os terminale. • A finding of a fragment at the superiormost tip of the odontoid may be due to a fracture or it may a normal ossification pattern. Craniocervical Junction • First, extension of a line down the slope of the clivus should point to the superior end of the dens (the os terminale). • The posterior margin of the foramen magnum should be in line with the spinolaminar line. • Such an alignment places the foramen magnum in-line with the spinal canal, this corresponds to the junction of the brain stem and the spinal cord. Extension of a line down the slope of the clivus should point to the superior end of the dens (the os terminale). Hangman’s Fracture The hangman's fracture is an unstable fracture of the C2 pedicles, with forward displacement of C1 and the body of C2 on C3. This traumatic spondylolisthesis of C2 is the result of hyperextension of the head relative to the neck. Hangman’s Fracture • The upper portion of the cervical spine (skull, C1, C2) separates from the lower cervical spine. • Hyperextension will initially cause fracture of the C2 neural arch (pedicles) and disruption of the anterior ligaments. • The return to neutral position will cause the body of C2 to become anteriorly displaced over C3. • In a hangman's fracture, the anterior and posterior cervical lines will usually be abnormal because of the anterior displacement of C2 on C3. • Spinolaminal line can be normal. Subluxation vs. Pseudosubluxation • Developmental variants of the cervical spine in young children – Make reading x – ray more difficult – In a patient with a hangman's fracture, when the fracture of the neural arch (pedicle) of C2 is not visible on the lateral neck view (an uncommon occurrence), the only evidence of the fracture may be modest malalignment of C2-C3. Pseudosubluxation vs. Hangman’s # • 1.Mechanism inj in pseudosubluxation is generally more benign. – A hangman's fracture is typically an acceleration/deceleration mechanism (motor vehicle crash) or a hanging mechanism. • 2. A pseudosubluxation is ONLY seen on lateral neck radiograph views that are positioned without lordosis (i.e., in flexion, or neutral). – If C2-C3 malalignment is noted on a lateral neck radiograph with good lordotic (extension) positioning, this is probably a TRUE subluxation (a hangman's fracture), and NOT a pseudosubluxation. • 3. A visible fracture of the neural arch is usually evident on the lateral neck view in a hangman's fracture. The absence of a visible fracture does not rule out a hangman's fracture since it may be difficult to visualize radiographically at times. Swischuk line Anterior aspect of the posterior arch of C1 to the anterior aspect of the posterior arch of C3. The anterior aspect of the posterior arch of C2 should be within 1-2 mm of this line. If it is deviated > 2 mm, this is indicative of a true subluxation. Hangman’s # - N line Normal pt – head in flexion with pseudosubluxation If it is deviated < 2 mm, it is consistent with a pseudosubluxation, (this alone is insufficient to r/o a hangman's fracture.) Case • A 7-year-old male was diving off a ledge when he landed head first in shallow water. He was pulled semiconscious from the water by lifeguards. While maintaining his airway, the lifeguards placed the patient in full C-spine immobilization. When the patient became more alert, he complained of pain to his upper neck region. Paramedics transported the patient to the ED. Jefferson’s fracture • Lateral displacement of one or both of the atlantal lateral masses (black arrow) is suggestive of a Jefferson fracture in which the ring of C1 is fractured, bursting it open displacing the lateral masses outward. What is the matter? Lateral masses displaced! The lateral masses of C1 are displaced outward, indicating a "bursting" of the ring of C1 (the Jefferson Fracture). Normal odontoid views Jefferson Fracture • Compression and/or bursting fracture of C1. – Unstable fracture secondary to axial compression load, • Fall or strike on head. • Neurologic injury is rare but can occur if there is involvement of C2. • Axial load on C1 lateral masses, causes them to be compressed against the superior articular facets of C2 Lateral Jeffersons Fracture Anterior displacement of C1 on C2 • In the most classic cases, the damage to C1 usually occurs in four places, with fractures in two sites anteriorly and two sites posteriorly. • When C1 is fractured in less than four places, transverse ligament tears are common and can lead to more instability. • If the transverse ligament is ruptured, C1 will move forward on C2, and the spinal cord will be compressed. • 1/3 of Jefferson fractures are associated with other cervical spine fractures, with C2 associated fractures being the most common. Practice radiographs . . . Summary • Do your C-spine ABC’s • C1 Fracture – Jefferson’s burst fracture • C2 Fracture – Hangman’s – Don’t forget about pseudosubluxation! • Increased prevertebral space (retropharyngeal abcess or soft tissue swelling). Predental <3 or < 5 if under 8, C3 <5 or <7 kids, C7 <22 (<14 at C6 in kids) • Clivus and Swischuk line References • • • • http://www.hawaii.edu/medicine/pediatrics/pemxray/v5c03.html Pediatric Emerg Med Reports 1996;1:83. Lecrture Notes Terry O’Brien (NYGH Emergency Medicine conference 2002) Perry, Clayton. Handbook of Fractures. McGraw Hill, 2000.